
Abstract
Objective:
To explore the key factors influencing hearing recovery in patients with sudden sensorineural hearing loss (SSNHL) and provide a basis for clinical prognosis evaluation and individualized treatment.
Methods:
Clinical data of 164 inpatients with SSNHL at a tertiary hospital in Fujian Province from January 2022 to December 2024 were retrospectively analyzed, including basic characteristics, hearing features, examination findings, and treatment measures. Univariate analyses (Chi-square test, Kruskal-Wallis H test) and a multivariate logistic regression model were used to identify prognostic factors, and a neural network model was constructed to evaluate its predictive performance.
Results:
Among the 164 patients, 27 (16.46%) showed no response, 61 (37.20%) responded, 32 (19.51%) showed marked response, and 44 (26.83%) were cured. Univariate analysis revealed that age, length of hospital stay, degree of hearing loss, type of hearing loss, brain MRI findings, triglyceride (TG) levels, low-density lipoprotein (LDL-C) levels, and the use of glucocorticoids and batroxobin were associated with treatment outcomes (all P < .05). Multivariate logistic regression indicated that TG (OR = 0.559, P = .002) and LDL-C (OR = 0.352, P = .001) were independent risk factors, while glucocorticoid use was a protective factor (OR = 8.564, P = .004). The neural network model exhibited good predictive performance (AUC = 0.889, accuracy rate 86.5%).
Conclusion:
Advanced age, severe hearing loss (especially total deafness), abnormal brain MRI findings, and elevated TG and LDL-C levels may lead to poor prognosis in SSNHL, while early use of glucocorticoids can improve outcomes. The neural network model can effectively evaluate patients’ potential for hearing recovery.
Introduction
Sudden sensorineural hearing loss (SSNHL) is an acute sensorineural hearing disorder of unknown etiology, characterized by a sudden unilateral or bilateral significant hearing loss (≥30 dB across two or more consecutive frequencies) within 72 hours, often accompanied by tinnitus, aural fullness, and vestibular symptoms such as vertigo. 1 Epidemiological studies have shown that the global annual incidence of SSNHL ranges from approximately 5 to 27 per 100 000 population. Due to its complex etiology, it may be linked to viral infections, microcirculatory dysfunction, and immune dysregulation. 2 Given such complexity, there is no specific treatment modality, and some patients may develop permanent hearing impairment. Current clinical management primarily involves comprehensive treatment regimens, including glucocorticoids combined with vasodilators and microcirculation-improving agents. However, therapeutic efficacy varies significantly among individuals, and controversies remain regarding the impact of patients’ clinical characteristics (eg, age, degree of hearing loss, and concomitant symptoms), laboratory indicators (eg, blood lipids and blood glucose), ultrasonic imaging findings, and the efficacy of traditional Chinese medicine (TCM) interventions on prognosis.
Abnormal lipid metabolism is associated with SSNHL by impairing inner ear microcirculation. 3 In contrast, glucocorticoids have emerged as the core therapeutic agent for SSNHL, as they inhibit inflammatory responses, reduce endolymphatic hydrops, and improve blood-labyrinth barrier function. 4 TCM is a commonly used component of comprehensive SSNHL treatment in China and some East Asian regions; however, critical evidence supporting its efficacy and safety remains insufficient to guide clinical practice. 5 Although previous studies have identified several prognostic factors for SSNHL, including the negative correlation between age, severity of hearing loss, and treatment outcomes, as well as the impact of metabolic indicators on disease progression.6 -8 No efficient multifactor predictive model has been established to integrate these variables for clinical application. Addressing these gaps, this study retrospectively analyzes the clinical data of SSNHL inpatients from a tertiary hospital in Fujian Province, focusing on the disease’s clinical characteristics and therapeutic factors (eg, lipid metabolism, glucocorticoids, and TCM) to identify key prognostic indicators and construct practical prediction tools. Ultimately, this work aims to provide evidence-based insights for the individualized treatment of SSNHL and the selection of therapeutic regimens across different regions.
Material and Methods
Sample Size Estimation
This study was a single-center retrospective observational analysis. The sample size was estimated based on the Events Per Variable principle: considering 12 key predictive variables included in the study (eg, age, degree of hearing loss, and blood lipid profiles), the minimum Events Per Variable value was set at 10, resulting in a minimum required sample size of 120 cases. A total of 164 cases were actually included, which met the statistical power requirements (power >80%, α = .05). The sample size was validated using PASS 15.0 software, showing that power for the primary outcome (efficacy categories) reached 89.3% with α = .05 and β = .2, meeting the standards for clinical study design.
Diagnostic Criteria
SSNHL was diagnosed in accordance with the 2019 Clinical Practice Guideline of the American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS), 9 Hearing loss was classified by severity based on pure-tone audiometry results: mild hearing loss (26-40 dB HL), moderate hearing loss (41-55 dB HL), moderately severe hearing loss (56-70 dB HL), severe hearing loss (71-90 dB HL), and profound hearing loss (>91 dB HL).
Inclusion Criteria
Patients were included in the study if they met the following criteria: a definite diagnosis confirmed to meet the clinical diagnostic criteria for SSNHL as specified in Section “Diagnostic Criteria”; an onset-to-admission interval (from symptom onset to hospital admission) of ≤7 days; no prior targeted treatment (including glucocorticoids, vasodilators, and TCM) before admission, and no history of prior treatment in outpatient clinics or other hospitals; and complete documentation of medical records, including details of disease course, audiological examinations (pure-tone audiometry), and other relevant laboratory and imaging data during hospitalization.
Exclusion Criteria
Patients were excluded from the study if they met any of the following criteria: secondary hearing loss due to underlying cranial organic lesions (eg, stroke, acoustic neuroma, and intracranial tumor) or otologic organic diseases (eg, Ménière’s disease, otitis media, and external auditory canal atresia); documented infectious etiologies, including a confirmed history of viral infections (eg, mumps and herpes zoster) or acute suppurative infections with pathogen detection; severe systemic diseases such as severe dysfunction of major organs (eg, heart, liver, and kidney) or active malignant tumors (including nasopharyngeal carcinoma, lymphoma, among others); special physiological conditions, specifically women who were pregnant or lactating; or incomplete data, defined as medical records with a missing rate of key variables ≥20%.
Study Population and Data Collection
Patient data were extracted from the hospital’s Hospital Information System and Laboratory Information System, with cross-verification by a second reviewer to establish an electronic database. The study cohort comprised patients with SSNHL hospitalized at a tertiary hospital in Fujian Province between January 2022 and December 2024. Initially, 186 patients with a confirmed diagnosis of SSNHL were identified, but 22 were excluded due to incomplete data: 5 cases with inconsistent diagnosis (eg, Ménière’s disease and posterior circulation ischemia), 6 cases with missing hearing curve patterns, 8 cases with incomplete imaging or laboratory findings, and 3 cases with missing treatment records. Analysis of missing data via Little’s Missing Completely at Random test confirmed a random missing pattern (P = .312), resulting in a final sample of 164 patients. Collection indicators are shown in Table 1.
Data Collection Framework for Predictive Modeling of SSNHL Recovery.
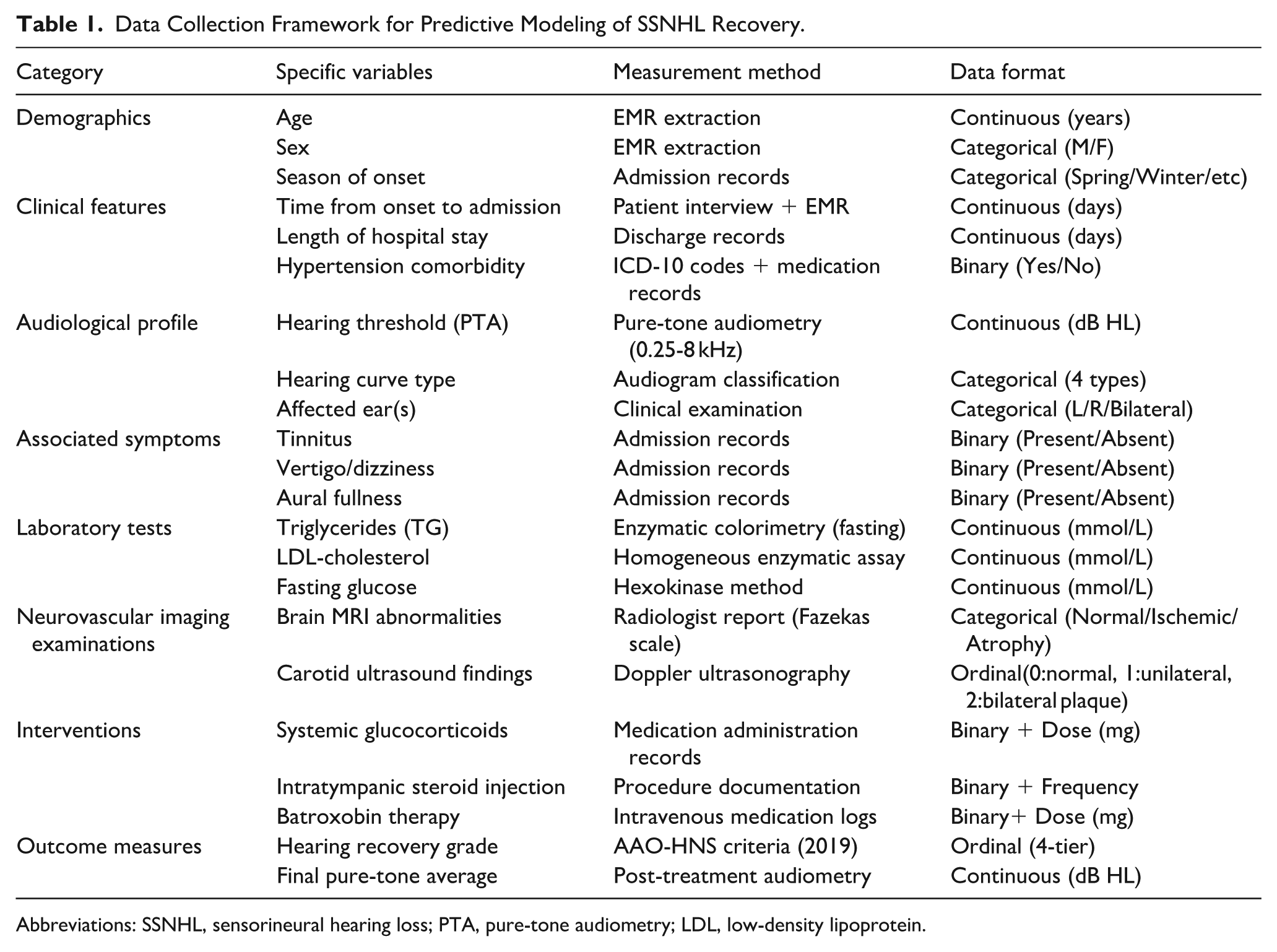
Abbreviations: SSNHL, sensorineural hearing loss; PTA, pure-tone audiometry; LDL, low-density lipoprotein.
Audiological Examinations
Pure-tone audiometry (PTA) was performed using a MAICO-MA51 clinical audiometer. All enrolled patients were adults without cognitive impairment or poor compliance, and tests were conducted in a standard sound-attenuated booth. For some patients, objective audiological examinations, including auditory brainstem response and distortion product otoacoustic emissions, were combined to ensure the accuracy of hearing results. The PTA test covered 7 frequencies (125-8000 Hz), with corresponding maximum sound outputs of 80, 100, 115, 120, 120, 120, and 105 dB HL, respectively. If no response was elicited at the maximum output, the threshold was recorded as the maximum output + 5 dB. Hearing results were documented, and the PTA was calculated.
Hearing at admission was defined as the initial audiometric assessment, while the final audiometric assessment was the last test result obtained when the patient achieved complete recovery or within 1 month after treatment initiation.
Treatment Regimens and Efficacy Evaluation Methods
Treatment regimens in this study were formulated in reference to China’s Guidelines for the Diagnosis and Treatment of Sudden Deafness (2015 Edition) and the AAO-HNS 2019 Guidelines, with the core protocols as follows: (1) Systemic glucocorticoids: Initiated within 72 hours of symptom onset, prednisone 30 to 60 mg/day (0.5-1 mg/kg body weight) for a course of 7 to 14 days; (2) Intratympanic injection: Dexamethasone 5 mg per dose, administered once or twice weekly (course duration: 7-14 days), reserved for patients with contraindications to systemic glucocorticoids or poor initial therapeutic response; (3) Batroxobin: Initial dose of 10 BU, followed by 5 BU every other day via intravenous infusion, for a total of 3 to 5 administrations; (4) TCM therapy: TCMs with blood circulation-promoting and collateral-dredging effects (based on the principles of “promoting blood circulation to remove blood stasis” and “dredging collaterals to open the orifices”) were adopted, with the course of treatment consistent with the hospitalization period. None of the enrolled patients had received targeted treatment in outpatient clinics or other hospitals prior to admission, ensuring no interference from treatment regimen heterogeneity.
Efficacy was strictly evaluated in accordance with guideline standards and classified into 4 grades: (1) Complete recovery: Hearing thresholds at the affected frequencies recovered to normal levels, matched the contralateral healthy ear, or restored to the pre-illness baseline; (2) Partial recovery: The average hearing threshold at the affected frequencies improved by ≥30 dB HL; (3) Slight recovery: The average hearing threshold at the affected frequencies improved by 15 to 30 dB HL; (4) No recovery: The average hearing threshold at the affected frequencies improved by <15 dB HL.
Statistics
Continuous data were first tested for normality using the Shapiro-Wilk test and for homogeneity of variance using Levene’s test.
Data conforming to a normal distribution were expressed as “mean ± standard deviation (χ− ± s),” where χ− denotes the mean and s denotes the standard deviation; intergroup comparisons were performed using one-way analysis of variance (one-way ANOVA). If the variance was heterogeneous, Welch’s ANOVA was used as an alternative. 10 Data not conforming to a normal distribution were expressed as “median (M) (25th percentile, 75th percentile; P25, P75),” where M denotes the median, and P25 and P75 represent the 25th percentile and 75th percentile, respectively. Intergroup comparisons for non-normally distributed data were conducted using the Kruskal-Wallis H test. 11
Categorical data were expressed as “n (%),” and intergroup comparisons were performed using the Chi-square test. 12 Unidirectional ordinal data refer to data with a clear hierarchical order among categories (eg, Complete recovery/Partial recovery/Slight recovery/No recovery); when the sample size is small, the Ridit analysis was adopted as a supplementary method. 13 Bidirectional ordinal data refer to data where both variables are ordinal categories (eg, degree of hearing loss and efficacy grading), and Kendall’s tau-b rank correlation analysis was used to evaluate the correlation between the two. 14
In the multivariate analysis, variables with P < .05 in the univariate analysis or those with clear clinical significance were included in the multivariate logistic regression model. Variables were screened using the backward stepwise method, and multicollinearity was evaluated via the variance inflation factor (VIF). A VIF < 10 indicates no significant multicollinearity.
To address the clinical demand for precise prognostic evaluation, the present study employed a neural network model to establish and analyze a predictive model for hearing recovery in SSNHL. Hearing recovery in SSNHL is influenced by multiple factors, including lipid metabolism indices, glucocorticoid use, and clinical characteristics. Neural network models exhibit strong adaptability and can effectively handle mixed data types (continuous, categorical, ordinal) included in this study. 15 In prognostic studies of SSNHL, neural networks have demonstrated superior predictive performance compared to conventional statistical models. 16
For the prediction model, the total sample was randomly divided into a training set (112 cases) and a test set (52 cases) at a ratio of approximately 7:3 using simple random sampling. A neural network model was constructed using the training set, and 5-fold cross-validation within the training set was performed to optimize model parameters and evaluate internal stability. The test set was used independently to assess the model’s generalization performance.
The performance of the predictive model was evaluated using the area under the receiver operating characteristic curve (AUC) and the Youden index: AUC was used to quantify the model’s discriminative ability, with an AUC > 0.7 indicating good predictive performance; the Youden index (calculated as: sensitivity + specificity − 1) was applied to determine the optimal cut-off value of the predictive model. 17
All statistical analyses were performed using SPSS26.0. Two-tailed P < .05 was considered statistically significant.
Results
General Characteristics
Of the 164 patients, 80 were male (48.78%) and 84 were female (51.22%). Gender distribution showed no significant association with treatment efficacy (P = .716). The median age was 43.00 (27.00, 60.00) years. The age difference between the ineffective group and the other 3 groups was significant (P = .000). Seasonal distribution was as follows: 34 cases (20.73%) in spring, 53 cases (32.32%) in summer, 45 cases (27.44%) in autumn, and 32 cases (19.51%) in winter. No significant association was found between seasonal distribution and treatment efficacy (P = .920).
Regarding affected ear laterality, most cases were unilateral (78 left ears, 69 right ears), with 17 cases (10.37%) involving both ears. Ear laterality was not significantly associated with efficacy (P = .852). The median duration from onset to admission was 4.00 (2.00, 7.75) days, and the median length of hospital stay was 8.00 (6.00, 11.00) days. The length of hospital stay showed a weak positive correlation with treatment efficacy (P = .036), suggesting that an appropriate extension of the treatment course may improve prognosis. Hypertension was present in 39 cases (23.78%), with no significant association with treatment efficacy (P = .124).
Clinical Features
Degree of hearing loss: A total of 135 cases (82.31%) presented with moderate-to-severe hearing loss. Spearman correlation analysis (both variables were ordinal) showed a negative correlation between the degree of hearing loss and efficacy grade (defined as cure, marked improvement, improvement, or ineffectiveness) (r = −0.306, P = .003), indicating that more severe hearing loss was associated with poorer prognosis (with a cure rate of 0% in the profound hearing loss subgroup).
Hearing curve patterns: The flat-type pattern was the most common, accounting for 80 cases (48.78%). Among the subgroups, the low-frequency type (29 cases) had the best prognosis, with 18 of 29 cases (62.07%) achieving a cure. This was significantly different from the high-frequency type (7 of 37 cases cured, 18.92%), flat type (19 of 80 cases cured, 23.75%), and total deafness type (0 cured) (P < .001). Post-hoc pairwise comparisons confirmed significant differences between the low-frequency type and the other 3 patterns.
Concomitant symptoms: Tinnitus was present in 147 cases (89.63%), dizziness/vertigo in 47 cases (28.66%), and aural symptoms (eg, aural fullness) in 49 cases (29.88%). None of these symptoms was significantly associated with treatment efficacy (tinnitus: P = .522; dizziness/vertigo: P = .357; aural symptoms: P = .107).
Inspection and Test Results
Brain MRI findings: Abnormalities were detected in 74 cases (45.12%), including 62 cases of ischemic lesions and 12 cases of brain atrophy. The difference in the proportion of patients with different curative effects between the 2 groups was statistically significant (P = .004 ).
Neck vascular color Doppler sonography findings: Abnormalities were observed in 66 cases (40.24%), including 20 cases (12.20%) with bilateral abnormalities. The cure rate in the bilateral abnormalities subgroup (1/20, 5.00%) was lower than that in patients with normal neck vascular CDS (31/98, 31.63%), but the difference was not statistically significant (P = .101).
Lipid profiles and metabolic indicators: In the ineffective group, TG levels (2.33 [1.08, 4.49] mmol/L, non-normal distribution, Kruskal-Wallis H test) and LDL-C levels (3.48 ± 0.95 mmol/L, normal distribution, one-way ANOVA) were significantly higher than those in the other 3 groups (P = .006 and P = .001, respectively). There were no significant differences in total cholesterol or fasting blood glucose between the ineffective group and the other 3 groups (all P > .05, with statistical methods adjusted according to data distribution).
Treatment Measures
The overall usage rate of batroxobin was 80.49% (132/164) across all patients, with notable variations among the 4 efficacy groups: 59.3% (16/27) in the ineffective group, 83.6% (51/61) in the effective group, 84.4% (27/32) in the markedly effective group, and 86.4% (38/44) in the cured group. Glucocorticoids were administered to 89.02% (146/164) of patients, with distribution across efficacy groups as follows: 66.7% (18/27) in the ineffective group, 95.1% (58/61) in the effective group, 96.9% (31/32) in the markedly effective group, and 88.6% (39/44) in the cured group. Chi-square tests confirmed significant differences in the usage rates of both batroxobin and glucocorticoids among the 4 efficacy groups (P = .022 for batroxobin; P = .043 for glucocorticoids). TCM was used in 51.22% (84/164) of patients, and intratympanic injection in 47.56% (78/164). However, no statistically significant differences in efficacy were observed among the groups for either intervention (P = .374 for TCM; P = .295 for intratympanic injection).
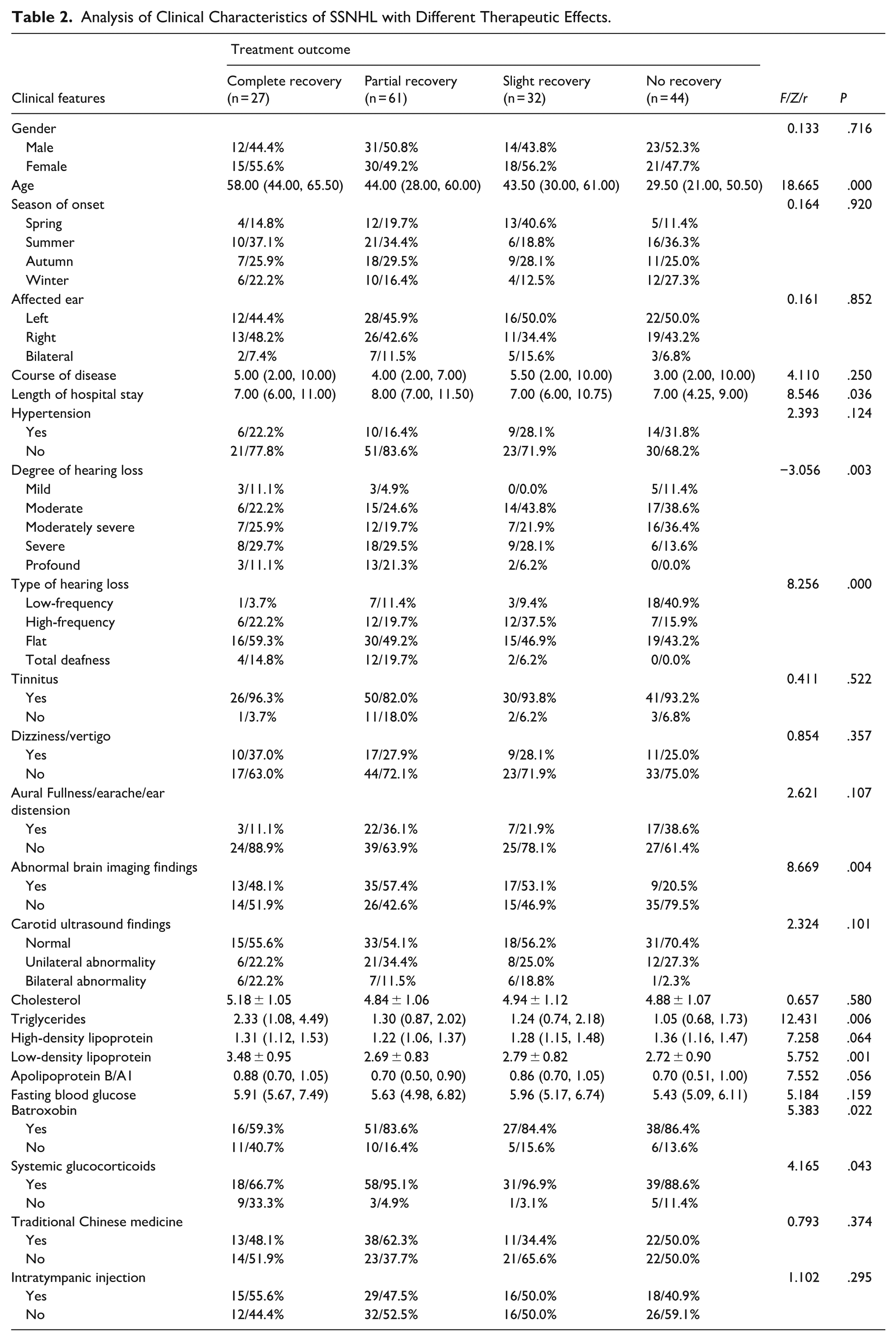
The above data results are shown in Table 2.
Analysis of Clinical Characteristics of SSNHL with Different Therapeutic Effects.
Predictive Model
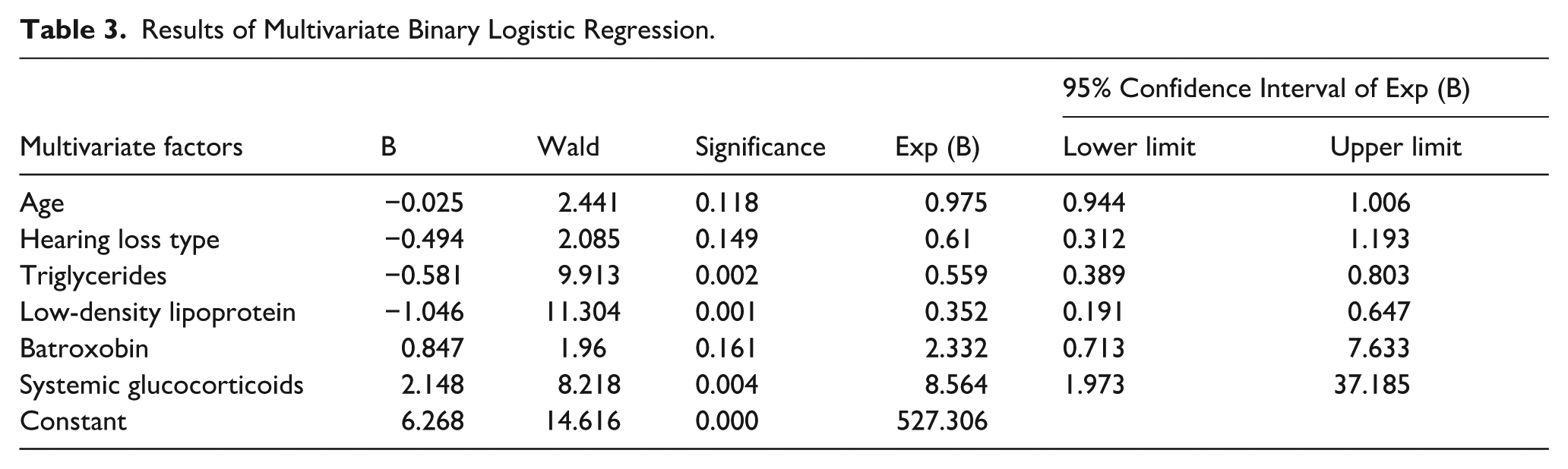
The area under the receiver operating characteristic (ROC) curve (AUC) of the backpropagation (BP) neural network model (2 hidden layers with 12 and 8 nodes, ReLU activation) was 0.889 (95% confidence interval [CI]: 0.821-0.957), with an overall accuracy of 86.5% in the test set. Multivariate logistic regression (variables selected via backward stepwise likelihood ratio test, α = .05) showed that triglyceride (OR = 0.559, P = .002) and LDL-C (OR = 0.352, P = .001) were independent risk factors, while glucocorticoid use (OR = 8.564, P = .004) was a protective factor (Table 3).
Results of Multivariate Binary Logistic Regression.
A combined prediction model integrating the neural network and logistic regression yielded an AUC of 0.864 (95% CI: 0.794-0.935), with a maximum Youden index of 0.61, a cut-off value of 0.754 (determined by the maximum Youden index), a sensitivity of 86.9%, and a specificity of 74.1%, indicating that it effectively evaluates prognosis (Figure 1).
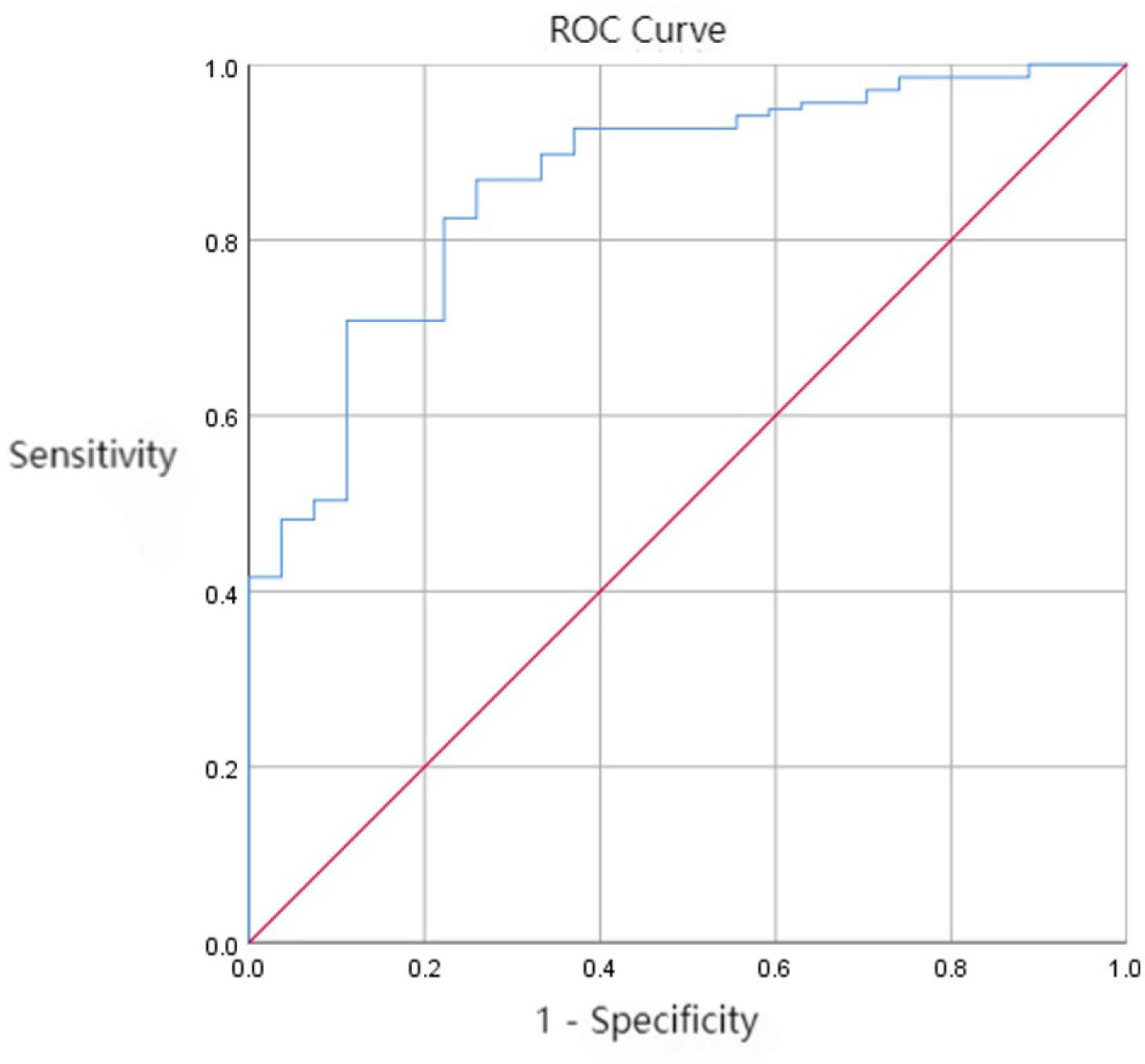
ROC curve of the neural network model.
Discussion
Through the analysis of 164 patients with SSNHL, this study confirmed that age, degree of hearing loss, type of hearing loss, dyslipidemia, and the use of batroxobin and glucocorticoids are key prognostic factors. The finding that older age is associated with poorer prognosis is consistent with the conclusions of studies by Ha 18 and Vukelic, 19 which may be attributed to the decline in regenerative capacity of inner ear hair cells and insufficient microcirculatory reserve due to vascular sclerosis. 20 The negative correlation between the degree of hearing loss and prognosis indicates that severe to profound hearing loss often implies extensive inner ear damage, severe impairment of hair cell function, and potential involvement of nerve conduction pathways. 21 Thus, even with aggressive treatment, the possibility of hearing recovery remains low, 22 supporting the view proposed by Edwige Gombert that “severe hearing loss requires intensive treatment.” 23
The low-frequency hearing loss type shows a more significant advantage in prognostic improvement, which may be related to the physiological characteristic that hair cells in the basal turn of the cochlea (high-frequency region) are more sensitive to damage. 24 Elevated triglycerides and LDL-C exacerbate poor prognosis, and the underlying mechanism may involve dyslipidemia promoting thrombus formation, which obstructs the spiral artery. 25 Occlusion of the labyrinthine artery may cause hearing loss, vertigo, and tinnitus. 26 High triglyceride levels are a risk factor for SSNHL 27 ; therefore, it is recommended to strengthen lipid control in SHL patients with hyperlipidemia, and combined intervention with statins when necessary, which may help improve hearing prognosis. 3
Jelena Todic suggested that abnormal brain tissue findings on cranial MRI predict poor hearing recovery in the high-frequency range. 28 This study found that abnormal brain MRI findings (ischemic foci or brain atrophy) were associated with poor prognosis in patients with SSNHL (P = .004), and such abnormalities were significantly correlated with age: the MRI abnormality rate was 75.00% (33/44) in patients aged ≥60 years, which was significantly higher than that in patients aged <60 years (34.17%, 41/120). Increasing age leads to cerebral arteriosclerosis, which not only raises the risk of cerebral ischemia/atrophy but also impairs the blood supply to the inner ear. 29 Cerebral white matter lesions may exacerbate hearing impairment by interfering with signal processing in the auditory center. 30 Therefore, for elderly patients with SSNHL, abnormal brain MRI findings can serve as an important warning indicator for poor prognosis.
Batroxobin is not a universally recommended agent in clinical practice guidelines for the treatment of SSNHL. The relevant clinical evidence remains conflicting: batroxobin exerts therapeutic effects by improving inner ear microcirculation and other mechanisms, 31 whereas other studies have demonstrated that its efficacy is not significantly different from that of conventional therapy. 32 Although batroxobin is not listed as a first-line recommended treatment in international guidelines, our center still incorporates it as a key component of the comprehensive treatment regimen, taking into account its pharmacological properties of reducing blood viscosity, promoting fibrinolysis, and exerting antithrombotic effects. 33 Univariate analysis indicated that the usage rate of batroxobin was significantly associated with treatment efficacy (P = .022). However, this factor was not included in the final model of multivariate logistic regression analysis, suggesting that the efficacy of batroxobin may be modulated by other confounding factors.
Glucocorticoids can promote hearing recovery by inhibiting inflammatory responses, reducing endolymphatic hydrops, and improving blood-labyrinth barrier function. 4 International guidelines clearly recommend initiating systemic glucocorticoid therapy as early as possible, within 72 hours of onset, to maximize the preservation of inner ear function. 34 Regarding the efficacy of intratympanic steroid injection, although some scholars have pointed out that for patients with poor response to systemic medication or contraindications to systemic use, intratympanic injection can improve hearing thresholds through the action of high local drug concentrations, 35 the use of intratympanic injection in this study did not show a significant difference in efficacy (P = .295). This may be attributed to the inability to separately distinguish the synergistic effect of systemic and local medication, heterogeneity in injection techniques and doses, and insufficient sample size.
Although no internationally recognized unified diagnosis and treatment standards for TCM in the treatment of SSNHL have been established, TCM intervention remains one of the characteristic therapies in the comprehensive treatment of SSNHL in our center, based on the pharmacological effects of Tongqiao Huoxue Decoction in promoting angiogenesis and protecting against cerebral vascular reperfusion injury.36,37 In this study, patients who voluntarily received TCM treatment were given oral standardized Tongqiao Huoxue Decoction. Statistical analysis showed that there was no significant correlation between TCM treatment and the efficacy in SSNHL patients (P = .374), and the core reason lies in the heterogeneity in the application of TCM prescriptions: although standardized preparations were used, there were differences in the TCM syndrome differentiation types of the included patients, and no stratified analysis was performed for different syndrome types, which may introduce bias in efficacy evaluation.
Regarding the seasonal distribution characteristics of SSNHL onset, there remains controversy in the academic community with significant divergence in research conclusions: some studies have reported that the incidence peak of SSNHL occurs in spring and the trough in winter 38 ; other studies have confirmed that there are significant seasonal differences in its incidence, with the peak risk in summer (P < .001) 39 ; some scholars have also proposed that the existing evidence is insufficient to support the existence of a clear seasonal onset pattern of SSNHL. 40 The results of this study showed that there was no significant correlation between the season of SSNHL onset and treatment efficacy (P = .920). Due to the inconsistency of existing research conclusions and the limitations of this study, the correlation between the two cannot be clearly confirmed for the time being.
Conclusion
This is a single-center retrospective observational study, and the sample has geographical characteristics. It also relies on the completeness of medical records, with insufficient standardization of some treatment details (such as TCM prescriptions and hormone doses), which may introduce bias. Heterogeneity in treatment regimens (eg, adjuvant therapies not included in the analysis) and small sample sizes in some subgroups (total deafness type, bilateral abnormal color Doppler ultrasound) may affect statistical power. Efficacy assessment was based on data at discharge or within 1 month after treatment initiation, with a lack of long-term follow-up, failing to reflect long-term hearing stability and the sustained impact of interventions. Future studies need to further verify these findings through multicenter prospective studies, standardized treatment regimens, and extended follow-up periods.
Footnotes
Ethical Considerations
This study was reviewed and approved by the Ethics Committee of the Third Affiliated Hospital of Fujian University of Traditional Chinese Medicine (Ethics Approval No.: 2025KS-165-1), which granted an exemption from the requirement for informed consent, and was conducted in strict compliance with the ethical principles of the Declaration of Helsinki.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Medical Innovation Project of the Science and Education Department of Fujian Provincial Health Commission (Grant No.: 2025CXA050) and the National Traditional Chinese Medicine Advantage Specialty Construction Project (Geriatrics) [grant numbers 20250042].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statements
The data that support the findings of this study are available from the corresponding author upon reasonable request.