
Abstract
Introduction
Tympanoplasty is a standard surgical procedure which aims to repair tympanic membrane perforation and restore auditory function under the premise of removing middle ear lesions. 1 Since Zollner and Wullstein invented tympanoplasty in 1956 for the first time,2,3 it has been regarded as a practical and effective intervention for middle ear disease. The successful graft uptake rate is very high (>90%) 4 ; However, differing variables lead to discrepant hearing outcomes and many clinical studies have evaluated the factors that impact hearing recovery.
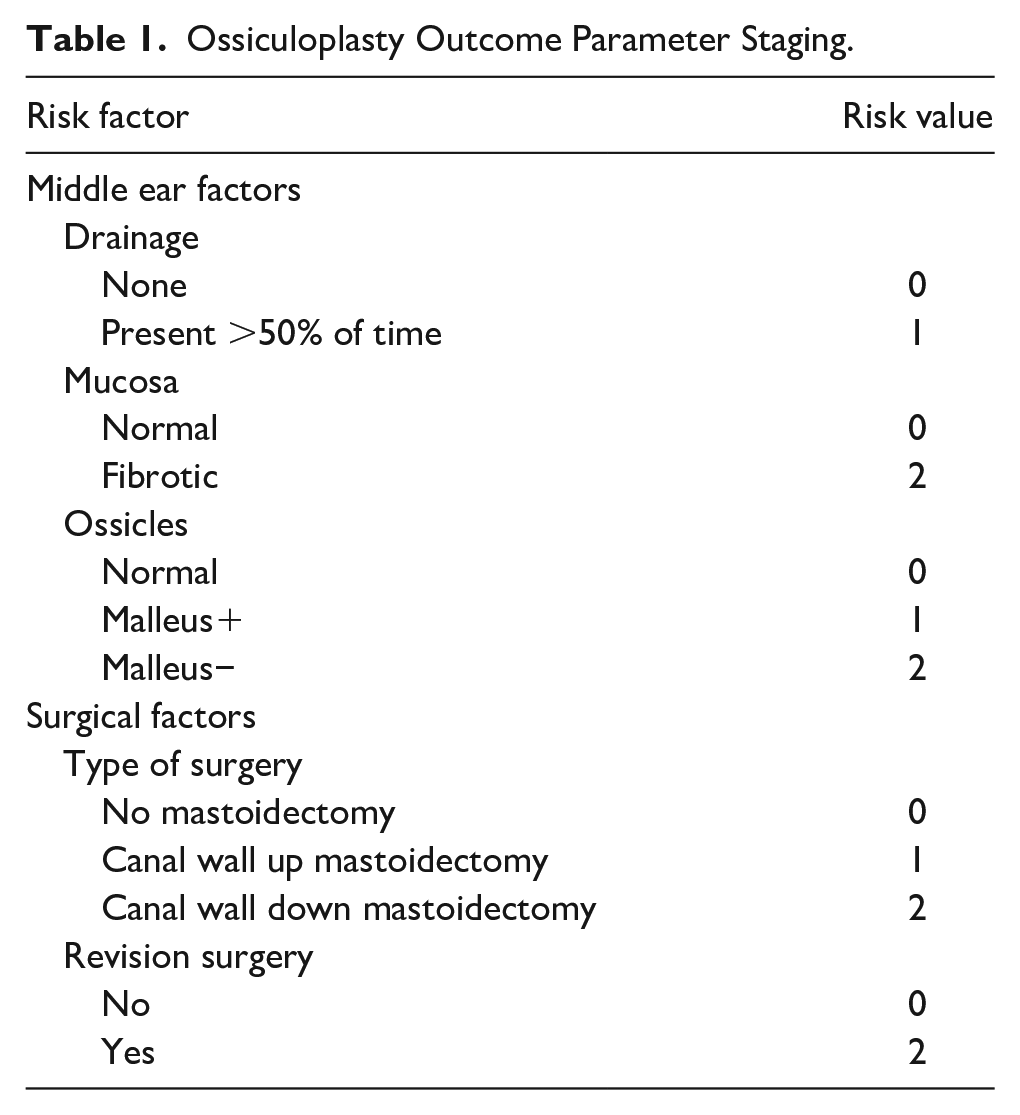
Dornhoffer and Gardner developed an index titled Ossiculoplasty Outcome Parameter Staging (OOPS) to predict hearing outcomes in ossicular chain reconstruction, 5 including prognostic variables such as drainage, mucosa, ossicles, type of surgery, and revision surgery (Table 1). To date, however, there has not been a consensus on the use of OOPS index to predict hearing outcomes following tympanoplasty.6-8 Additionally, it is worth exploring possible factors (such as smoking and perforation) that are not included in this index compared to the Middle Ear Risk Index (MERI).9,10
Ossiculoplasty Outcome Parameter Staging.
In addition to the anatomical and functional outcomes, health-related quality of life has been an increasingly important outcome parameter after middle ear surgery. 11 The most common complaints of patients are social interaction impediments, due to discharge from the ear, the need to avoid water, and frequent medical examinations after surgery, 12 which can affect the quality of life and the emotional sphere. Therefore, achievement of a dry and self-cleaning ear cavity is another important goal of tympanoplasty. 13 Previous studies have paid little attention to this goal, and the predictors associated with dry ear time or recovery time are currently unknown.
This research aimed to verify the effectiveness of OOPS in predicting hearing and find out the potential factors that can predict the postoperative recovery time, to provide better guidance for the surgeon to perform tympanoplasty.
Patients and Methods
Participants and Study Design
This research was a single-center retrospective observational study. A total of 185 patients confirmed with chronic suppurative otitis media (CSOM) or cholesteatoma who underwent tympanoplasty at Department of Otolaryngology, Peking Union Medical College Hospital were enrolled in this study between January 2019 and July 2022. The diagnosis of cholesteatoma depended on clinical manifestations, imaging features, and pathological diagnosis. Cholesteatoma epithelium can be seen under endoscopy in patients with perforated tympanic membrane. Computed tomography (CT) showed increased soft tissue density with bone resorption and destruction. For atypical imaging findings, the patient was further treated with MRI. And the intraoperative specimen was confirmed by the pathologist ultimately. Patients aged <18 years, at risk for general anesthesia or severe infection like meningitis, with less than 6 months of follow-up and missed data on pure tone audiometry (PTA) were excluded. Finally, 138 patients and 151 ears were enrolled. This study was reviewed and approved by the Ethics Review Committee of Chinese Academy of Medical Sciences & Peking Union Medical College Hospital (approval no. I-22PJ375) and patient agreement was waived due to the retrospective nature of this analysis.
Data Collection
Demographic information, duration of the dry period, type of otitis media, preoperative otorrhea, tympanic membrane perforation, anesthesia time, volume of blood loss, aditus ad antrum patency, and surgical characteristics were collected retrospectively from electronic medical records. Intraoperative blood loss was the total amount of fluid in the aspirator bottle, minus the amount of irrigation fluid used during the operation, and plus the weight added by the gauze and cotton pads used. As there was no consensus of guideline on the amount of blood loss during middle ear surgery, we chose the median 10 mL as the cutoff value. The perforation of tympanic membrane was assessed by transcanal endoscopic examination. The tympanic membrane was divided into 4 quadrants according to the position of the malleus handle, and damage in any quadrant was defined as perforation of the tympanic membrane. 10 All patients underwent a CT in coronal and axial positions with a scanning thickness of 2 mm and a radiation dose of 2~4 mSv. A soft tissue density greater than 50% at the aditus ad antrum on CT was defined as a blocked aditus ad antrum. 14 The OOPS index was used to evaluate middle ear disease burden and incorporated factors of drainage, mucosal inflammation, status of the ossicular chain, type of surgery performed, and previous surgery history. According to the OOPS score, the patients were classified into 3 groups: low-risk group (OOPS equal to or less than 3), intermediate-risk group (OOPS of 4-6), and high-risk group (OOPS equal to or greater than 7) when predicting hearing outcomes after ossiculoplasty.6,8 The PTA audiogram was measured at the last visit before surgery and included pure tone air and bone conduction thresholds at 0.5 kHz, 1 kHz, 2 kHz, and 4 kHz.
Surgical Technique
All surgeries were performed under general anesthesia by an experienced surgeon. For patients with milder lesions, tympanoplasty is performed under endoscopic guidance from the outer ear canal into the middle ear. For patients with cholesteatoma otitis media or CSOM with extensive lesions, endoscopic or microscopic guided tympanoplasty was performed behind the ear through the temporal bone into the middle ear cavity to remove the lesions, and then mastoidectomy was performed. The canal wall up (CWU) or canal wall down (CWD) mastoidectomy was adapted according to preoperative and intraoperative evaluation of clinical symptoms and imaging character. The procedure of mastoidectomy was to make a C-type incision after disinfection, enter the tympanic sinus through the recess of the facial nerve and tympanic diaphragm, fully open the mastoid and tympanic sinus, and remove the lesion tissue. CWU maintained the integrity of the contour of the external auditory canal (EAC) by completely preserving the posterior wall of the EAC or reconstructing the local defect after removal of the diseased tissue. Temporal fascia, perichondrium, or cartilage-perichondrium grafts were used in myringoplasty depending on the patients. After completion of the procedure, the EAC was filled with gelatin sponge.
Outcome Measures
The main evaluation index of tympanoplasty was to achieve graft success and improve listening competence based on the removal of lesions from the middle ear. In addition, we focused on postoperative recovery time to reduce patient’s medical burden and quality of life. This study defined graft success as intact graft healing without atelectasis at 6-month follow-up visit. Hearing success was considered as a PTA air-bone gap (PTA-ABG) of 20 dB or less at the 6-month follow-up visit. The PTA was calculated as the average thresholds at 4 frequencies at 0.5 kHz, 1 kHz, 2 kHz, and 4 kHz. Kartush classification has been used to establish the association between hearing and OOPS. In the Kartush classification, postoperative PTA-ABG is excellent at 0 to 10 dB, good at 11 to 20 dB, fair at 21 to 30 dB, and poor at more than 30dB. 15 Recovery time was recorded when there was no fluid or exudate and a clean tympanic cavity in the EAC under otoscopy at weekly follow-up postoperatively until fully recovered.
Data Analysis
Categorical variables were presented as frequencies with percentages. Continuous variables were presented as mean ± standard deviation. Binary logistic regression was applied to the predictive factors for graft success and hearing success. When continuous variables were converted to categorical variables, if guidelines and consensus were not available, means or medians were used. Only variables with P-value < .05 in the univariable analysis were entered into multivariable analysis. Kaplan–Meier survival curves and Cox univariate regression analysis were applied to identify independent factors for recovery time and the Cox multivariate regression analysis was ultimately performed with P-value < .05. All analyzes were performed with SPSS version 25 (SPSS Inc., Chicago, IL, USA).
Results and Analysis
Hearing Outcomes of Tympanoplasty
A total of 138 patients and 151 ears were included from January 2019 to July 2022 in the study, as shown in Table 2. The overall mean preoperative and postoperative PTA-ABG was 32.2 ± 10.9, 25.3 ± 13.2 dB, respectively. Table 3 displays preoperative and postoperative PTA-ABG in 3 OOPS categories. The mean preoperative PTA-ABG was 30.0 dB in low-risk, 37.8 dB in intermediate-risk, and 33.8 dB in high-risk group. Patients in low-risk group had significantly (P = .000) better hearing than those in intermediate-risk group. After tympanoplasty, the mean PTA-ABG was 23.1 dB, 29.8 dB, and 36.8 dB, respectively. The patients in low-risk group had a lower PTA-ABG compared to the intermediate-risk (P = .006) and high-risk group (P = 0.021).
Characteristics of Patients and Surgical Parameters.
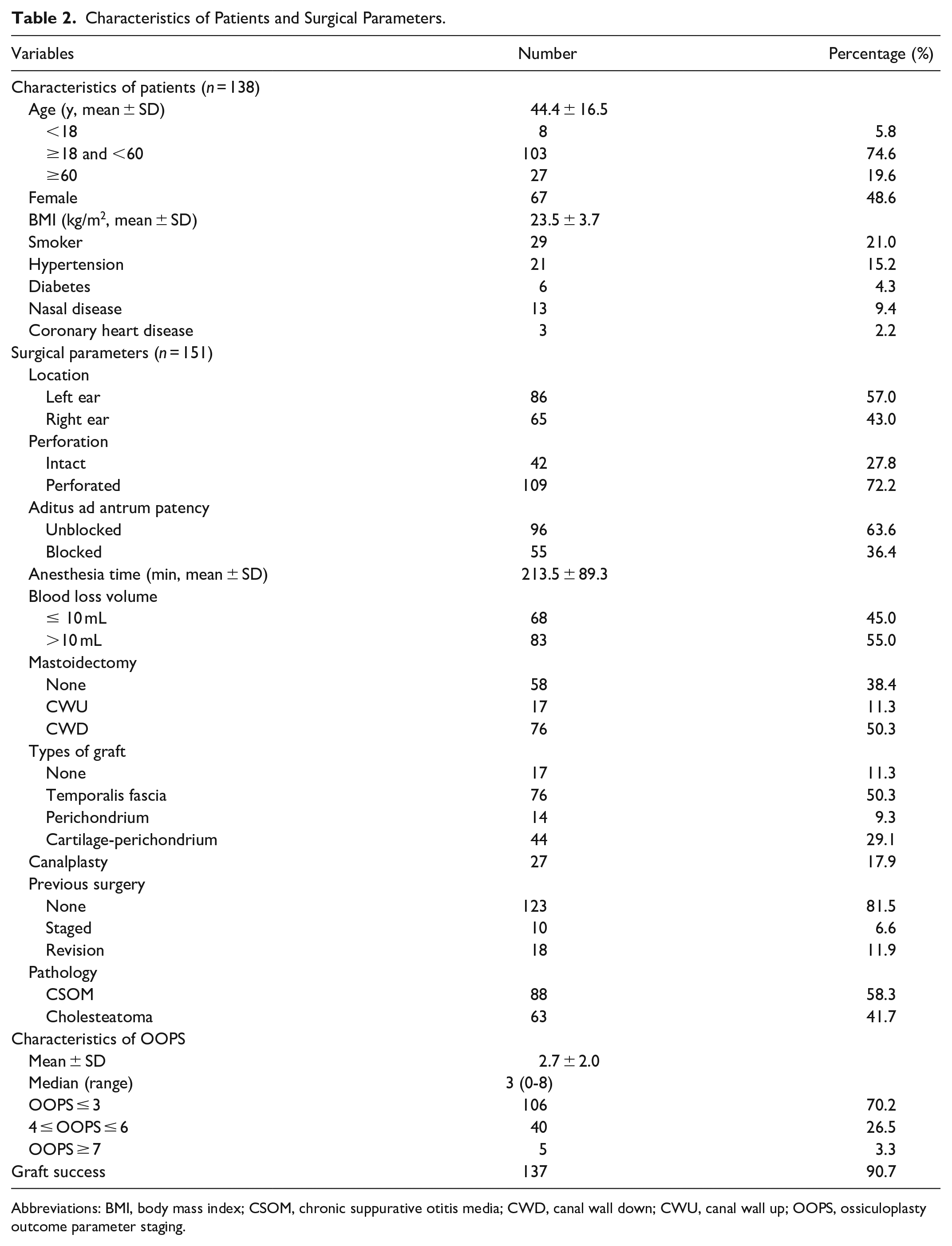
Abbreviations: BMI, body mass index; CSOM, chronic suppurative otitis media; CWD, canal wall down; CWU, canal wall up; OOPS, ossiculoplasty outcome parameter staging.
Mean Comparisons of Preoperative and Postoperative PTA-ABG (dB HL) Between Three Groups: Low-, Intermediate-, and High-Risk Groups OOPS Categories.
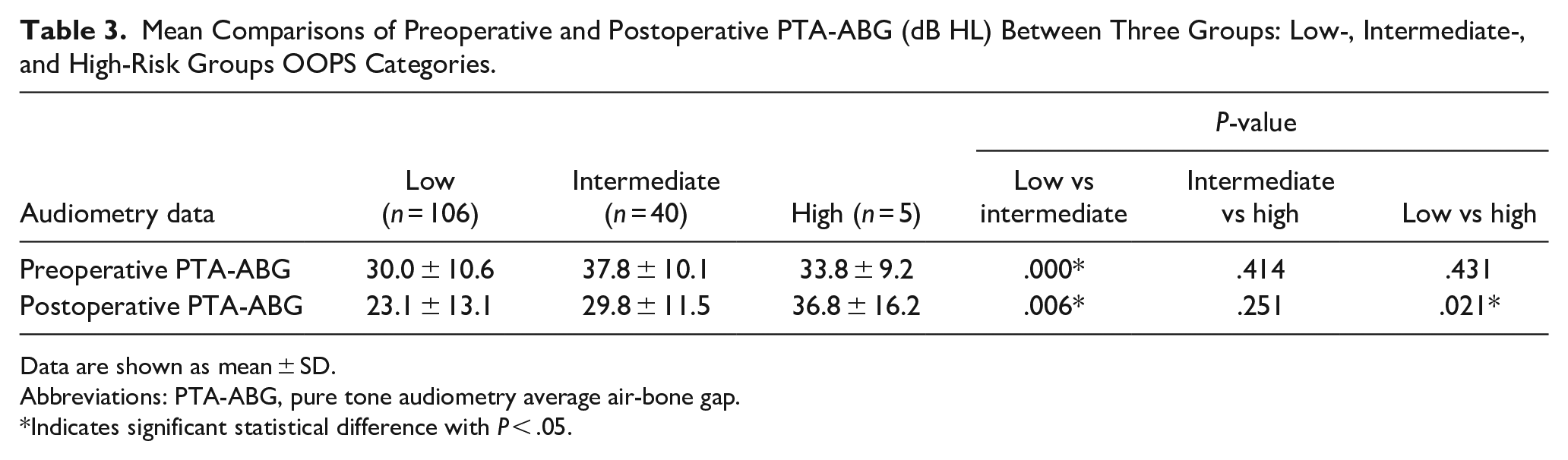
Data are shown as mean ± SD.
Abbreviations: PTA-ABG, pure tone audiometry average air-bone gap.
Indicates significant statistical difference with P < .05.
A total of 61 procedures (40.4%) were reported to have hearing success. Figure 1 shows postoperative PTA-ABG based on OOPS categories according to Kartush classification. Patients in low-risk group had a high proportion of obtaining better hearing outcomes, while patients in intermediate- or high-risk group were more likely to have relatively poor hearing outcomes. There existed a moderate correlation between OOPS categories and postoperative PTA-ABG (Spearman r = 0.322, P = .000).
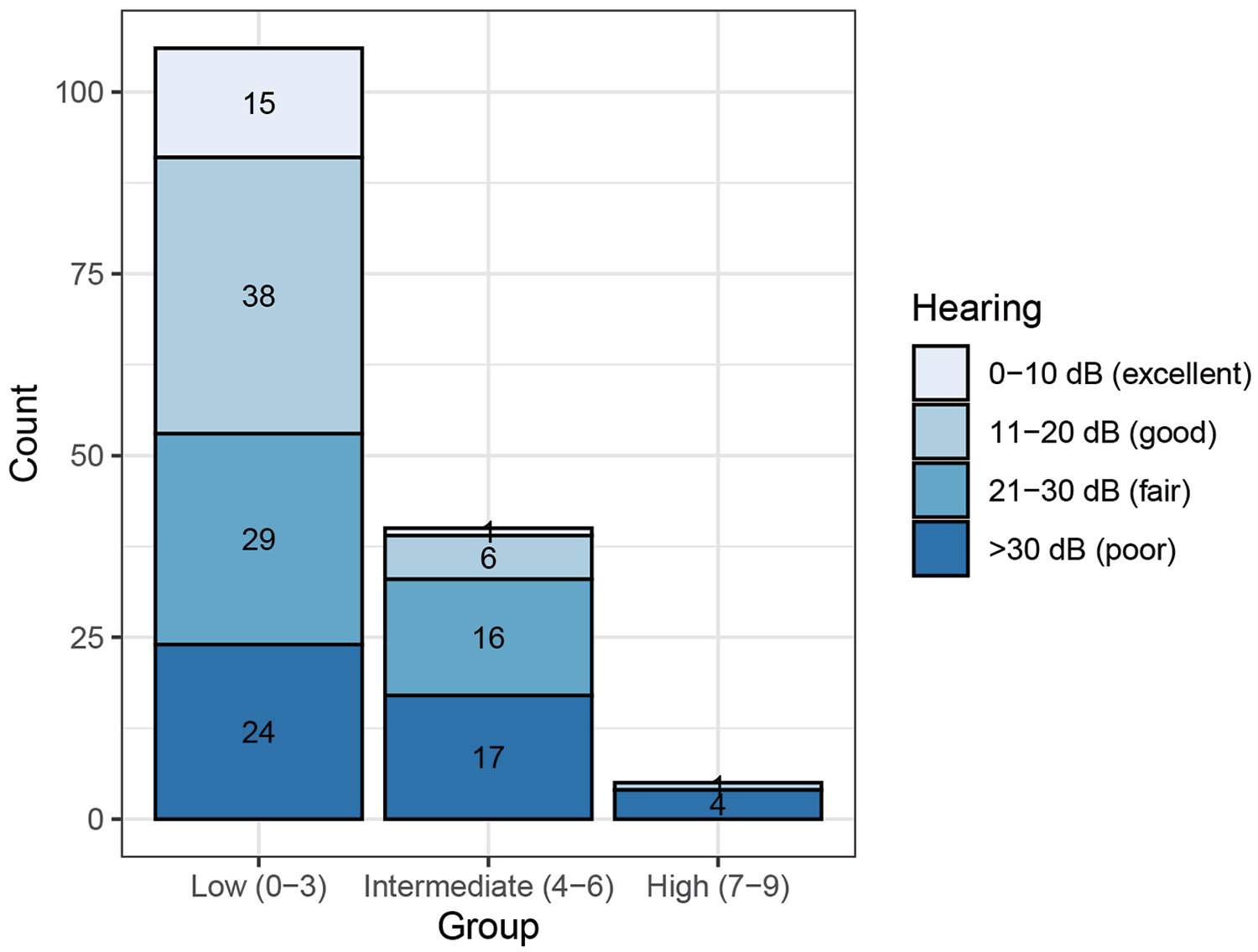
Postoperative PTA-ABG (Kartush classification) based on low-, intermediate- and high-risk OOPS categories. The Spearman rank coefficient was 0.322, which indicated a moderate correlation. The P-value was .000 and tested at the .01 level (2-tailed)
Factors Affecting the Graft and Hearing Outcomes
Table 4 shows the predictive factors for graft success and hearing outcomes using logistic regression analysis. Only a blocked aditus ad antrum (P = .008) was confirmed as a significant independent predictor of the graft outcome. In the univariate analysis of hearing outcomes, blood loss > 10 ml (P = .000), duration of anesthesia >210 minutes (P = .038), the presence of cholesteatoma (P = .009), a blocked aditus ad antrum (P = .008), perforation (P = .012), types of mastoids, types of graft, and OOPS grade ≥ 4 (P = .001) were significant factors for hearing failure. A forest plot with various factors is shown in Figure 2A. In the multivariate analysis, blood loss > 10 ml (P = .000) and OOPS grade ≥ 4 (P = .006) were significant independent predictors of hearing failure (PTA-ABG > 20 dB).
Predictors of Graft and Hearing Outcomes.
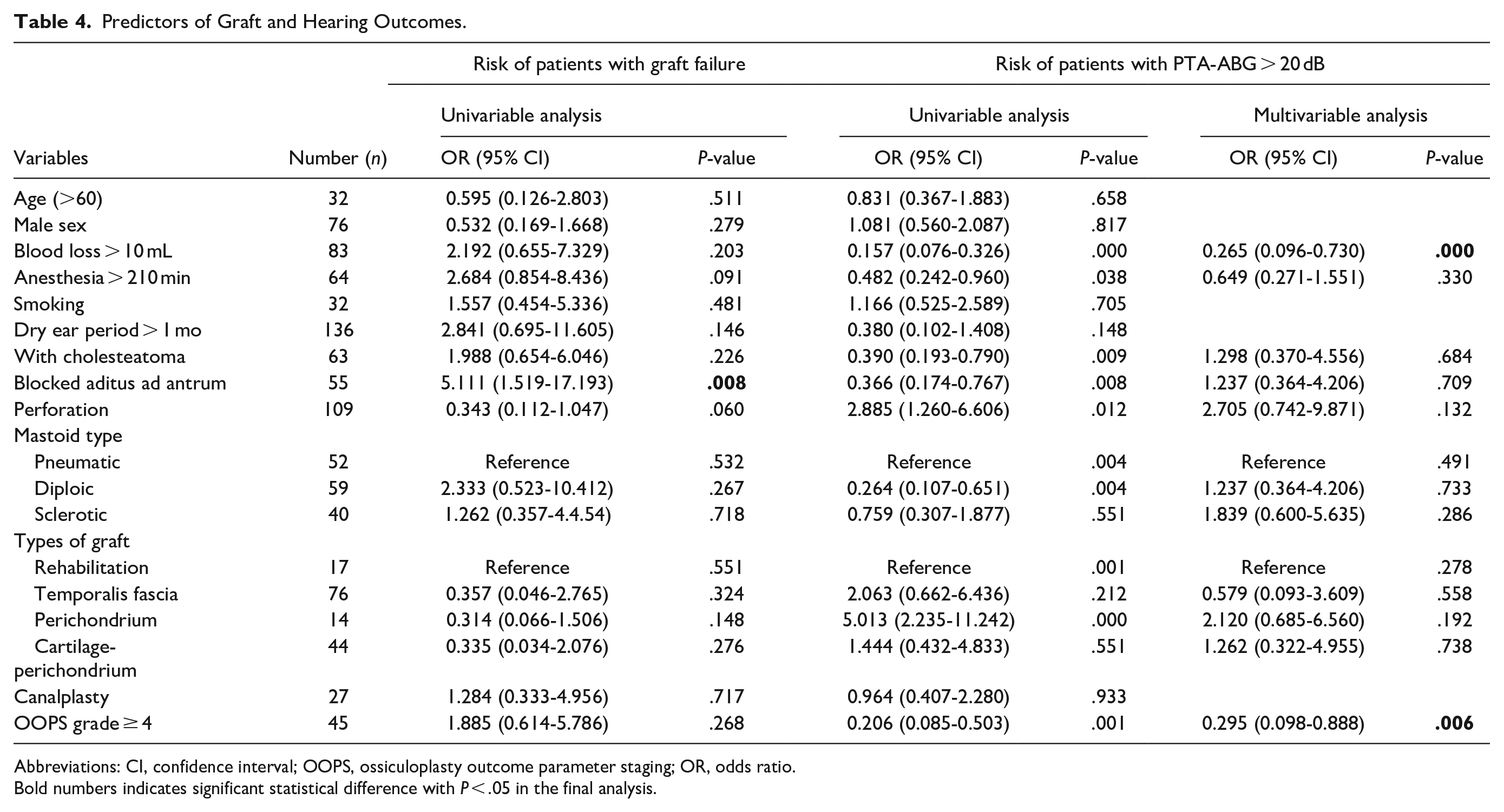
Abbreviations: CI, confidence interval; OOPS, ossiculoplasty outcome parameter staging; OR, odds ratio.
Bold numbers indicates significant statistical difference with P < .05 in the final analysis.
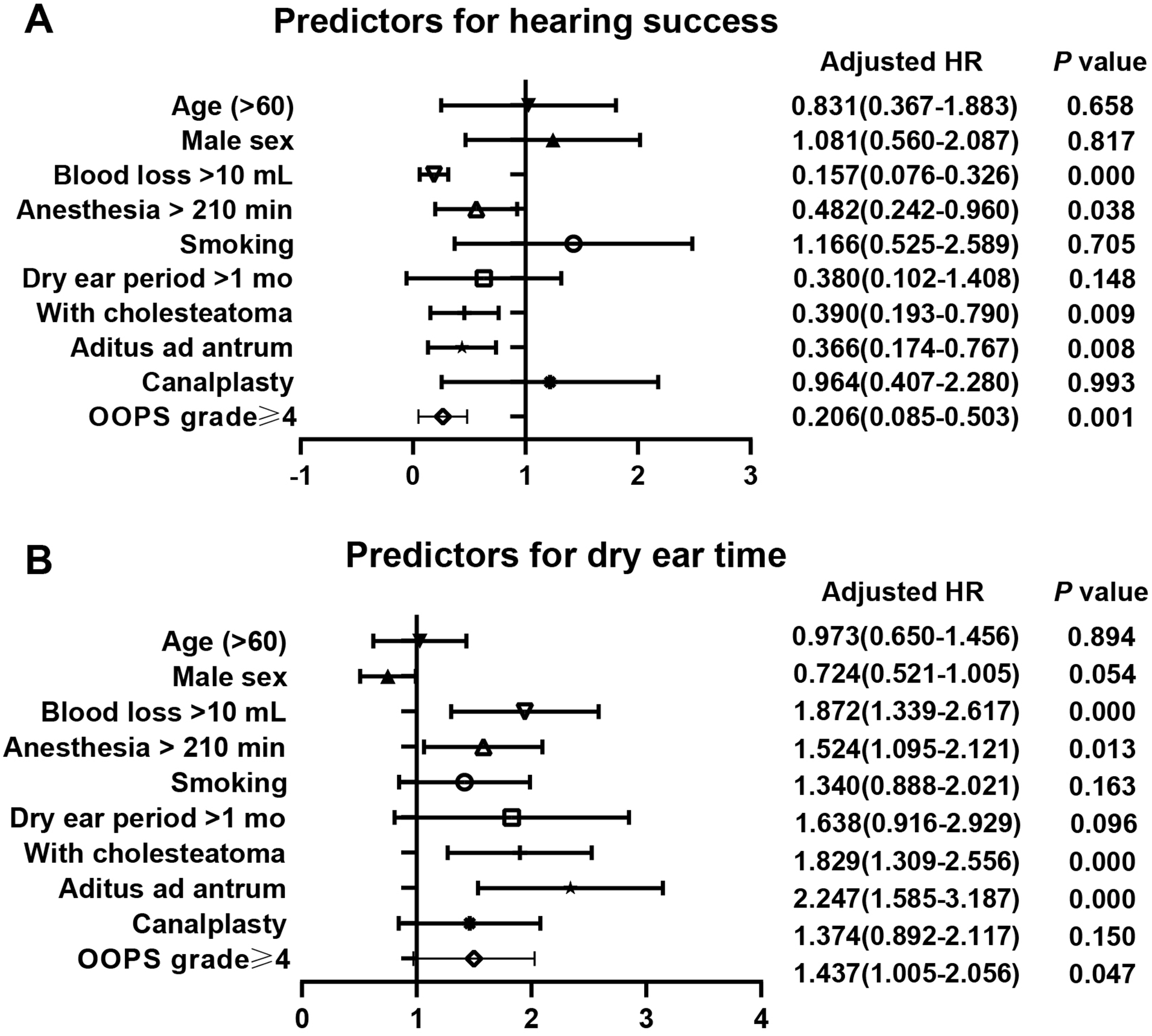
Multivariate analysis of risk factors for postoperative hearing outcomes and recovery time. (A) Predictors for hearing success. (B) Predictors for dry ear time.
Factors Affecting the Recovery Time
Figure 3 presents a typical recovery process at 9 days, 16 days, 30 days, and 51 days after tympanoplasty. The former 3 stages were accompanied by fluid exudation and sticky secretions in EAC under the endoscope, which was considered as wet ear. At the last stage, there was no exudation of fluids or abnormal secretions, which was considered as dry ear. In this research, the mean dry ear time was 44 days. Only 4 (2.6%) patients were still in wet ear state at the end of the study. Predictive factors for dry ear time are summarized in Table 5 and shown in Figure 2B. In the Cox univariate analysis, blood loss >10 ml (P = .000), duration of anesthesia >210 minutes (P = .013), the presence of cholesteatoma (P = .000), a blocked aditus ad antrum (P = .000), perforation (P = .044), types of mastoids, types of graft, and OOPS grade ≥ 4 (P = .047) were significant factors for prolonged recovery time. Meanwhile, Kaplan–Meier survival analysis was also performed to test the significance of variables, as well as the concordance index (Figure 4). In the multivariate Cox analysis, blood loss >10 mL (P = .038) and blocked aditus ad antrum (P = .000) were significant independent predictors.
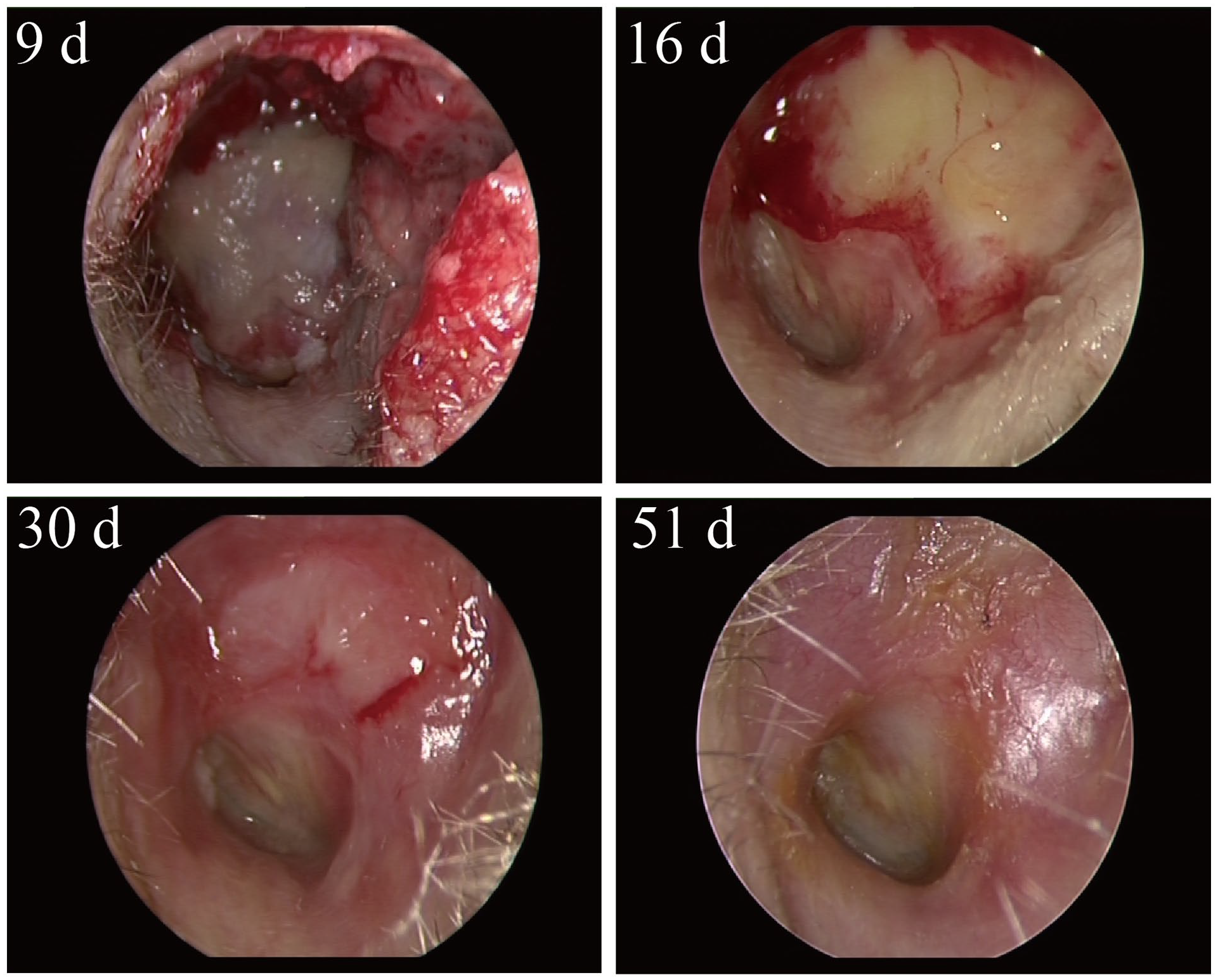
A typical recovery process at 9 days, 16 days, 30 days, and 51 days after otitis media surgery. The former 3 stages represent wet ear state and the last stage represents dry ear state.
Predictors of Dry Ear Time.
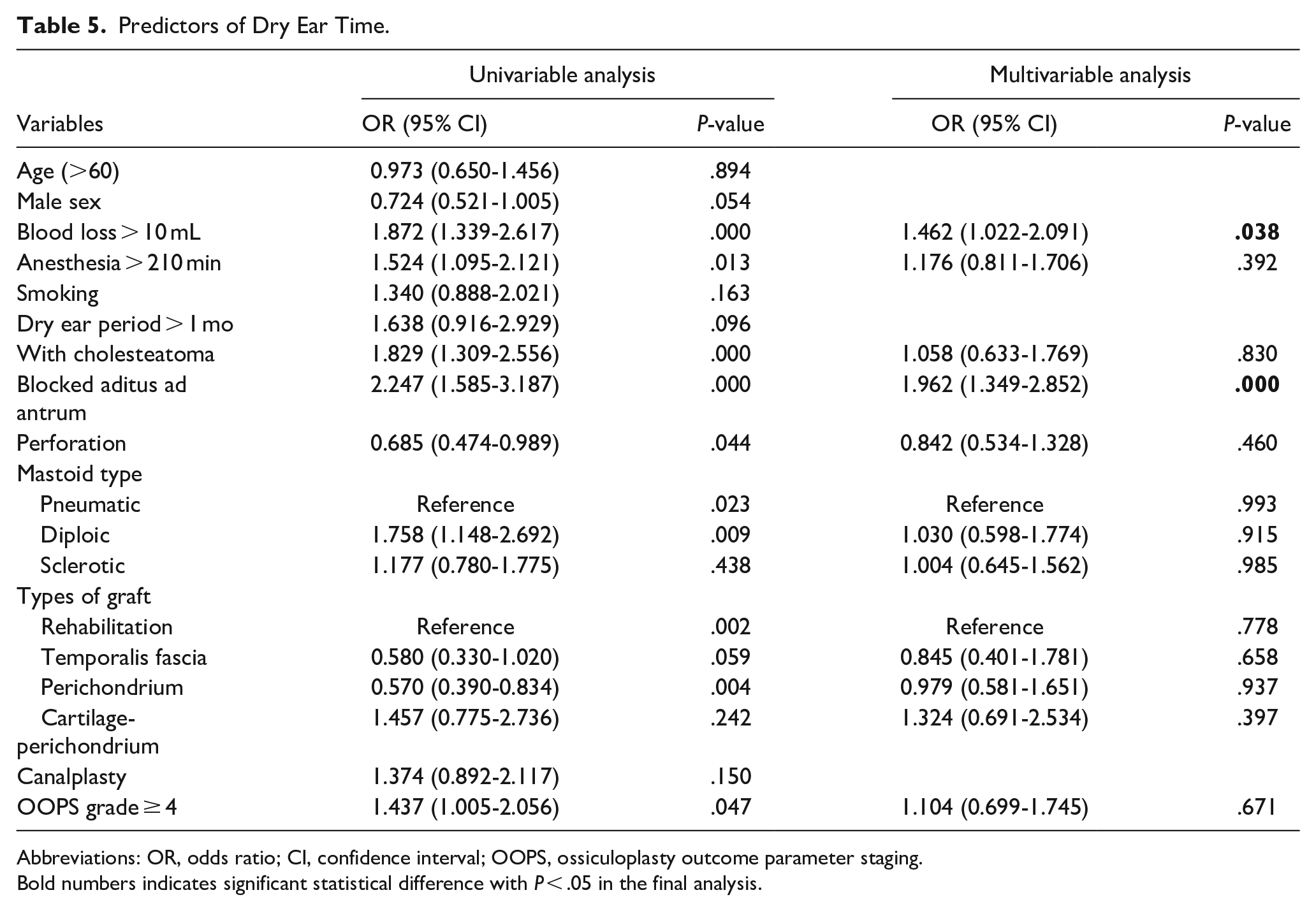
Abbreviations: OR, odds ratio; CI, confidence interval; OOPS, ossiculoplasty outcome parameter staging.
Bold numbers indicates significant statistical difference with P < .05 in the final analysis.
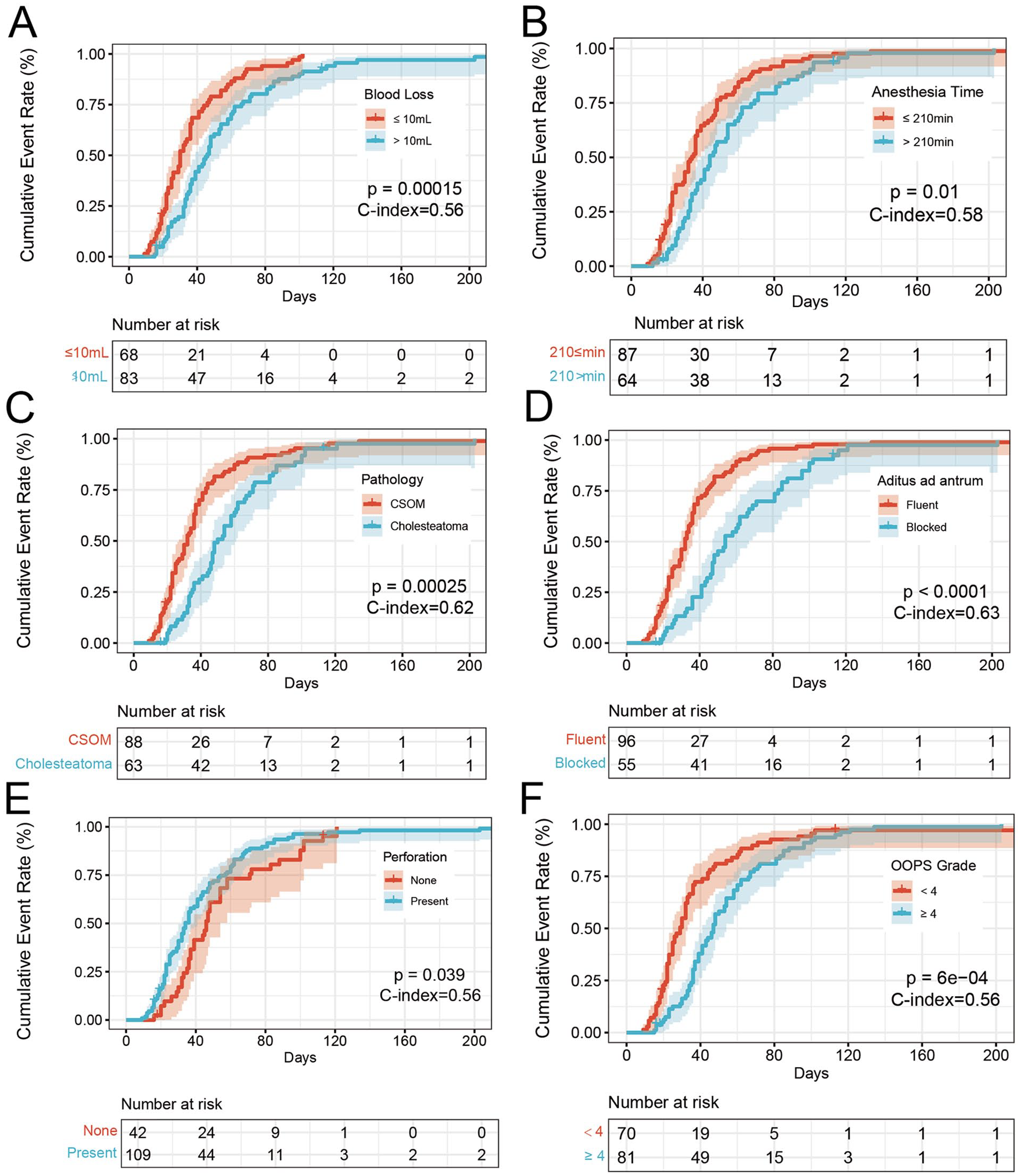
Kaplan–Meier survival curves in 151 procedures with tympanoplasty. (A) Blood loss volume. (B) Anesthesia time. (C) Pathology. (D) Aditus ad antrum. (E) Perforation. (F) OOPS Grade.
Discussion
The objective of tympanoplasty is to repair tympanic membrane, provide a dry ear, and restore the sound-conducting system of the middle ear. In our study, the overall 6-month graft success was 90.7% and was consistent with reported success rates (>90%).4,15,16 A total of 61 (40.4%) patients presented with hearing success (PTA-ABG ≤20 dB) at 6-month follow-up visit and the results were below average for other series with similar follow-up duration.6,15,17 This could be caused by the large number of patients with cholesteatoma otitis media (41.7%) in our sample cohort. The mean preoperative PTA-ABG was 32.2 dB and decreased to 25.3 dB after tympanoplasty, showing an improvement of 6.9 dB. The mean recovery time in this study was 44 days after tympanoplasty.
The degree of hemorrhage encountered during tympanoplasty emerged as an autonomous prognosticator for both auditory outcomes and the duration until the ear reaches dryness. Regrettably, this variable has a confounding influence, limiting its practical value in the clinical domain. Firstly, the quantification of intraoperative blood loss presents inherent challenges. In this investigation, we collated the volume of aggregate fluid within the aspirator receptacle, the amount of irrigation fluid used during the surgical procedure, and the increase in mass due to the deployment of gauze and cotton pads. During routine operations, there exists no intentional effort to calculate the additional weight resulting from the utilization of such materials. Furthermore, intraoperative blood loss is a multifaceted factor intricately linked to the gravity of middle ear pathologies. The duration of anesthesia, similar to the volume of blood loss, mirrors the complexity of the surgical intervention. Suzuki et al. discovered a notable association between prolonged anesthesia duration and an extended period necessitating localized post-tympanoplasty treatment. 18
Aditus ad antrum patency was an independent predictor of graft success and dry ear time. The general condition of the aditus ad antrum can be obtained through high resolution computed tomography preoperatively and postoperatively. 19 Patients with blocked aditus ad antrum have and suffer from graft atelectasis and prolonged wet ear time. Kurien and Bahgat et al. reported similar results.20,21 Some believe that aditus ad antrum plays a key role in the ventilation of the mastoid air cell system (MACS). This system plays an important role in maintaining ventilation between the middle ear and the external environment, excreting metabolic wastes in the middle ear cavity through ciliated epithelium, preventing pathogens from the nasopharynx from retrograde to the middle ear mucosa, and playing a role in immune defense. Blocked aditus ad antrum is caused by granulation or inflammatory hyperplasia of the mucosa at the entrance of the mastoid process and may lead to the obstruction of MACS ventilation, reduce the transmucosal gas exchange function, affect the middle ear pressure regulation, and thus impact graft success and recovery time. 22 Surgeons should carefully clean the lesions in epitympanum and maintain the patency of aditus ad antrum. For patients who undergo mastoidectomy, the structure of aditus ad antrum is severely damaged, and the function of MACS needs to be further studied.
The use of OOPS index allows surgeons to compare patients in different environments and can help predict hearing outcomes and the risk of complications or recurrence. It can also be useful to patients, providing them with useful information about the disease and adjusting expectations of the effect of treatment. In particular, it is important to acknowledge that the original purpose of OOPS development was to evaluate the results of ossicular chain reconstruction, rather than to predict the hearing results after tympanoplasty. Previous studies have shown different results on postoperative hearing prediction by MERI and OOPS index. Kotzias 6 and Tihanyi et al. 7 contended that the MERI surpasses the OOPS index in terms of precision when predicting hearing outcomes. On the contrary, Jung 8 and Cox et al. 17 proposed a significant correlation between postoperative PTA-ABG values and the OOPS index. These discrepancies can be attributed to disparities in study design. In this current study, we establish that the OOPS index independently and significantly prognosticates hearing outcomes after tympanoplasty. Furthermore, our findings indicate a correlation between OOPS scores and specific postoperative PTA-ABG values (according to Kartush scale), in line with the observations made by Cox. 17 Moreover, we found that more than half of the patients (70.2%) were classified as low risk, and only 5 (3.3%) patients belonged to high-risk group. Patients who meet the four criteria of OOPS index (total of 5 criteria) can achieve a score of 7 and be classified as high risk. In studies by others, the percentage of patients assigned to the high-risk group ranged from 0% to 4.2%.6,23,24 If the sample size of high-risk group is too small, it will not be comprehensive and representative, which will lead to over fitting and increase the error in data analysis.
Quality of life assessment represents a well-established parameter in healthcare, serving as a valuable metric to evaluate the efficacy and cost-effectiveness of treatment. Extended recuperation allows patients to resume their normal lifestyle quickly. Lucidi et al. demonstrated, through multivariate analysis, that extended follow-up duration was a significant determinant associated with postoperative improvements in Chronic Ear Survey scores. 12 Within our own investigation, decreased intraoperative blood loss and unobstructed aditus ad antrum were identified as factors that contributed to a faster achievement of dry ear status and a substantial reduction in the number of required follow-up visits. Drawing from the results of univariate analysis, we advocate for surgeons to consider evaluating the recovery time of tympanoplasty by assessing the presence of cholesteatoma, aditus ad antrum blockage, tympanic membrane perforation, and preoperative OOPS grade, thus allowing them to provide guidance regarding the postoperative frequency of follow-up appointments. However, it is important to note that we solely recorded objective data related to postoperative recovery time, and the correlations between recovery time and quality of life require further evaluation by administering relevant questionnaires to patients.
This study has several limitations. As a retrospective study, the rough description of physical examination in outpatient records made the specific time of recovery time was not exact. The research samples were small because some patients could not come for follow-up due to many reasons. We had to exclude patients without complete records as a retrospective study. Besides, we only analyzed the parameters that we could obtain accurately; some factors reported as possible effects were not included. As a single-center and single-surgeon decision, further prospective studies from multiple centers are required to confirm our study findings. Additionally, dry ear time was correlated with quality of life in this research. But we did not quantify this index by means of a questionnaire survey. Despite the limitations mentioned above, the study confirmed the role of the OOPS index in predicting hearing outcomes after tympanoplasty and analyzed the recovery time, which has received less attention from scholars previously.
Conclusions
In addition to its utility in ossicular chain reconstruction, the OOPS index also exhibits a favorable predictive capacity for hearing outcomes after tympanoplasty. Patients categorized as low risk are more likely to achieve successful hearing restoration after the procedure. The development of a prediction model that incorporates variables including the amount of blood loss and blockage of aditus ad antrum can serve as a valuable tool for surgeons, allowing them to predict postoperative recovery time and provide guidance regarding the optimal frequency of follow-up visits prior to performing tympanoplasty.
Footnotes
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further inquiries can be directed to the corresponding author.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Wu Xuan and Zhang Qing contributed equally to the work and should be regarded as co-first authors. We declare that we have no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Beijing Science and Technology Project (grant number: Z191100007619040); the Special Research project of Capital Health Development (grant number: 2020-2Z-40115); and Innovation and Entrepreneurship Training Program for College Students of Peking Union Medical College (grant number: 2023zglc06056).
Ethical Approval
This study was approved by the Ethics Review Committee of Chinese Academy of Medical Sciences & Peking Union Medical College Hospital (approval number I-22PJ375).
Statement of Human and Animal Rights
This article does not contain any studies with animal subjects.
Statement of Informed Consent
Informed consent for patient information to be published in this article was not obtained as this is a retrospective analysis.