
Abstract
Objectives:
To compare postoperative auditory outcomes after cochlear implantation (CI) between patients with chronic otitis media (COM) and those with noninflammatory sensorineural hearing loss (SNHL) and to evaluate the impact of labyrinthitis and duration of deafness.
Methods:
We retrospectively analyzed 33 postlingual COM cases and 70 age- and sex-matched SNHL controls. Pre- and postoperative audiologic tests were obtained, and preoperative computed tomography and magnetic resonance imaging were reviewed for labyrinthitis. The surgical status and stage (single- or 2-stage procedure) of cases with COM cases were documented.
Results:
Postoperative aided thresholds and word recognition scores (WRS) did not differ significantly between the groups. Complete bone conduction scale-out was more frequent in the SNHL group (P = .003). Labyrinthitis, found in 3 patients with COM (9.1%), was associated with a significantly lower WRS (P = .007 vs SNHL; P = .024 vs COM without labyrinthitis). In contrast to the SNHL group, patients with COM maintained stable WRS even with long-term deafness (>20 years).
Conclusion:
CI in COM yields auditory outcomes comparable to non-COM cases. In the absence of labyrinthitis, patients with COM showed preserved speech performance despite long-standing deafness, suggesting preserved cochlear/neural integrity. Preoperative imaging is valuable for detecting labyrinthitis, which predicts poorer postoperative results.
Highlights
Cochlear implantation (CI) in chronic otitis media (COM) yielded auditory outcomes comparable to non-COM cases.
Patients with COM maintained good word recognition scores even with deafness duration over 20 years.
Preoperative labyrinthitis was associated with significantly-poorer CI performance.
Introduction
Cochlear implantation (CI) is a revolutionary and now widely accepted intervention for patients with severe-to-profound sensorineural hearing loss (SNHL). CI is now considered the standard of care for individuals who receive limited benefit from conventional hearing aids. Its indications continue to expand, and surgical refinements have facilitated implantation in patients with anatomically-altered or disease-affected temporal bones.
Historically, chronic otitis media (COM) was considered a relative or absolute contraindication for CI. This concern stemmed from the presence of chronic infection and anatomic disruption in the middle ear and mastoid, both of which posed risks for electrode extrusion, persistent infection, and intracranial complications.1 -3 Moreover, in cases of accompanying cholesteatoma, the risk of residual or recurrent disease poses a further diagnostic and therapeutic challenge, particularly after implantation.2,4
To address these aforementioned challenges, Fisch et al introduced the concept of a subtotal petrosectomy in 1986, which involves blind sac closure of the external auditory canal, Eustachian tube obliteration, and mastoid cavity obliteration. 5 This technique was later adapted for CI in patients with COM and complex middle ear pathology. Depending on the condition of the middle ear and mastoid cavity, CI in patients with COM may be performed either as a single- or multi-staged procedure. Recently, this strategy has been established as a safe and effective treatment modality in the management of such cases.6 -8 Despite increasing reports of successful CI in patients with COM however, comparative outcome data between COM and SNHL patients remain relatively scarce.
This current study evaluated the effect of COM on auditory outcomes following CI by comparing patients with and without COM who underwent surgery using current surgical strategies. The impact of labyrinthitis on these outcomes was also investigated.
Materials and Methods
A retrospective medical chart review was conducted at a single tertiary care institution of patients who had undergone CI between July 1, 2006, and July 31, 2021. Patients aged 18 years or younger and those with prelingual deafness were excluded from further analysis. The final study cohort consisted of COM cases who underwent CI combined with subtotal petrosectomy and had available preoperative and 1 year postoperative audiometric evaluations. The SNHL group included patients with a normal cochlear, middle ear, and mastoid anatomy who received a standard CI without additional procedures. The SNHL group was matched to the study group at a 2:1 ratio based on age, gender, and surgical period. Matching by surgical period was designed to minimize any variability related to advancements in CI technology and surgical techniques. The presence of labyrinthitis in the COM group was identified using preoperative CT and MRI. The study protocol was approved by the institutional review board of our institution (IRB no 2023-1512). Informed consent was waived by the IRB.
Audiologic and Imaging Evaluation
Audiometric assessments included both aided and unaided pure tone audiometry and monosyllabic word recognition scores (WRS), obtained preoperatively and at the 1st year postoperatively. Audiometric assessments were performed using routinely calibrated devices in accordance with established measurement standards. 9 For each patient, bone conduction (BC) thresholds were measured at 500, 1000, 2000, and 4000 Hz. A case was defined as complete scale-out when BC thresholds exceeded the audiometer output limits at all 4 frequencies (60, 70, 70, and 60 dB HL, respectively). The duration of deafness was defined as the period during which patients reported no meaningful hearing even with hearing aid use. Preoperative imaging evaluations included high-resolution temporal bone CT and internal auditory canal MRI. The same CT and MRI protocol was performed for both the COM and SNHL groups. Labyrinthitis was defined radiologically as (1) loss of the normal T2 hyperintense fluid signal or a filling defect within the cochlear turns on high-resolution T2-weighted MRI, consistent with the fibrous or ossificans phase of labyrinthitis ossificans 10 and/or (2) visualization of ossification within the cochlea on high-resolution CT scans.11,12
Surgical Procedures
The SNHL group underwent CI using the standardized transmastoid facial recess approach in which electrodes were inserted via a round window approach in all of the patient subjects. In the COM group, surgery involved a subtotal petrosectomy, which entailed removing all pneumatic tracts of the temporal bone, completely eliminating the mastoid cells, mucosa, and epithelium, and isolating the middle ear cleft from both the external auditory canal (EAC) and the nasopharynx by closing the EAC in a blind sac fashion and sealing the eustachian tube. The cochlear implant devices used included Cochlear™ Contour Advance® (CI512, Nucleus24), Slim Straight® (CI422), and Slim Modiolar® (CI532, CI632) from Cochlear™ (NSW, Australia), as well as Flex28 and FlexSoft from MED-EL (Innsbruck, Austria).
Statistical Analysis
All statistical analyses were conducted using IBM SPSS for Windows, version 20.0 (IBM Corp, Armonk, NY, USA). Data are presented as mean values ± standard deviation. The Mann-Whitney test, paired t-test, 1-way ANOVA test, multivariate linear regression, and chi-squared test were used to compare continuous and categorical variables between groups. A P < .05 was considered statistically significant.
Results
A total of 103 patients were included in the final study cohort: 33 in the COM group and 70 in the SNHL group. There were no statistically-significant differences found between the 2 groups in terms of age, sex, or type of electrodes used. The characteristics of each group are described in Table 1. Notably, the proportion of patients with a complete BC scale-out was significantly higher in the SNHL group (P = .003). At the 1st year after CI, the COM group cases demonstrated a comparable postoperative performance to those in the SNHL group, with similar WRS and pure tone average at 500, 1000, 2000, and 4000 Hz (PTA4; P = .269 and .435, respectively). In the COM group, electrode insertion was performed via a round window approach in 18 patients (54.5%) and via cochleostomy in 14 patients (42.4%), while 1 case (3.0%) could not be confirmed from operative records. The mean postoperative WRS was slightly higher in the round window group (59.6% ± 25.3%) than in the cochleostomy group (42.3% ± 27.5%), but the difference was not statistically significant (P = .075). Two patients in the COM group experienced postoperative device extrusion through the scalp skin, requiring revision surgery.
Demographic and Audiologic Characteristics of Patients With SNHL and COM.
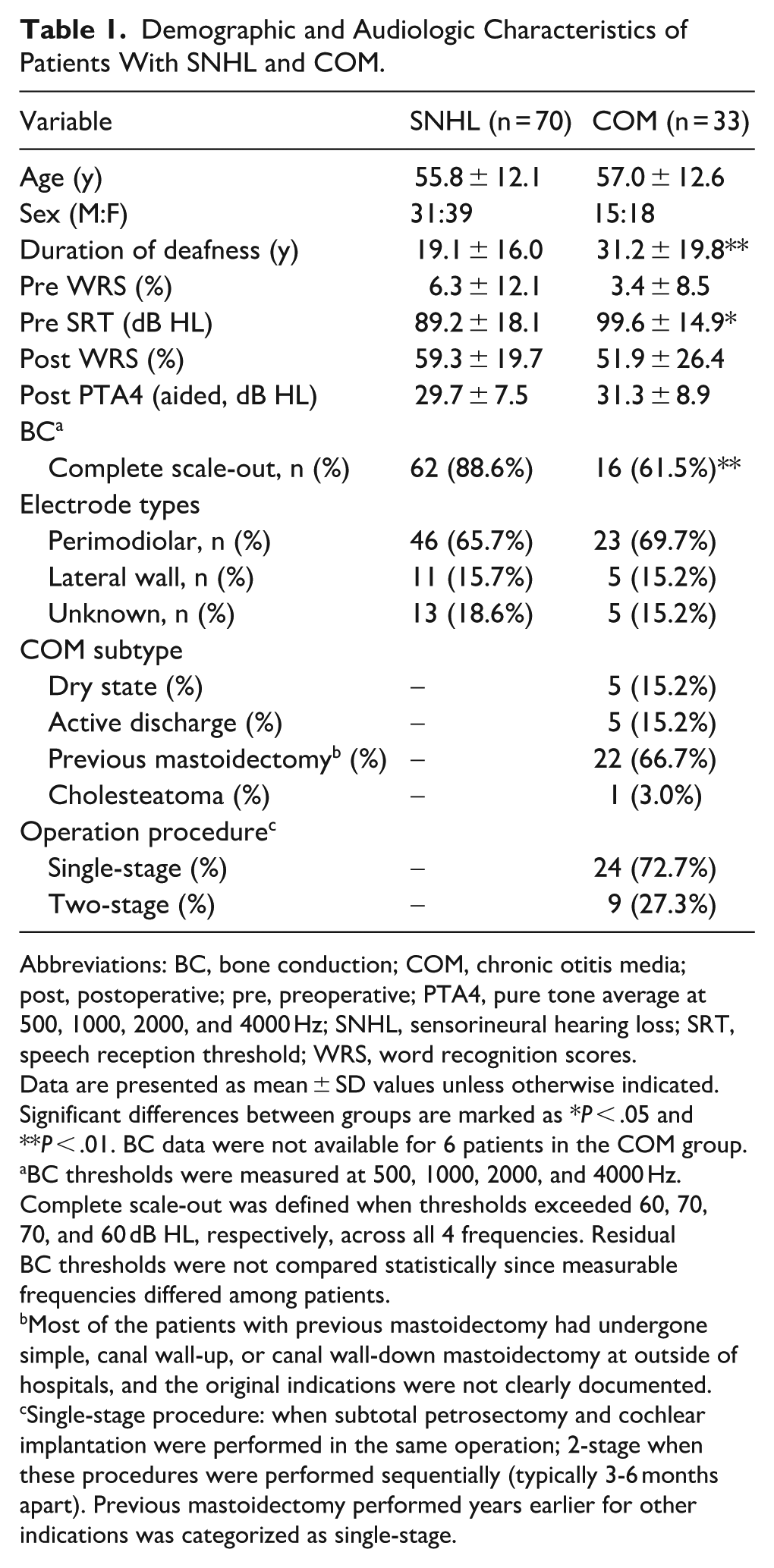
Abbreviations: BC, bone conduction; COM, chronic otitis media; post, postoperative; pre, preoperative; PTA4, pure tone average at 500, 1000, 2000, and 4000 Hz; SNHL, sensorineural hearing loss; SRT, speech reception threshold; WRS, word recognition scores.
Data are presented as mean ± SD values unless otherwise indicated. Significant differences between groups are marked as *P < .05 and **P < .01. BC data were not available for 6 patients in the COM group.
BC thresholds were measured at 500, 1000, 2000, and 4000 Hz. Complete scale-out was defined when thresholds exceeded 60, 70, 70, and 60 dB HL, respectively, across all 4 frequencies. Residual BC thresholds were not compared statistically since measurable frequencies differed among patients.
Most of the patients with previous mastoidectomy had undergone simple, canal wall-up, or canal wall-down mastoidectomy at outside of hospitals, and the original indications were not clearly documented.
Single-stage procedure: when subtotal petrosectomy and cochlear implantation were performed in the same operation; 2-stage when these procedures were performed sequentially (typically 3-6 months apart). Previous mastoidectomy performed years earlier for other indications was categorized as single-stage.
A multivariate linear regression analysis was performed to identify independent factors associated with postoperative WRS. After adjusting for age, sex, duration of deafness, and preoperative audiologic measures, group etiology (COM vs SNHL) was not associated with postoperative WRS (P = .884). Duration of deafness was the only significant predictor (B = −0.534, β = −.434, P < .001). Complete regression results are summarized in Table 2.
Multivariate Linear Regression Analysis of Factors Associated With Postoperative WRS at 1 Year.
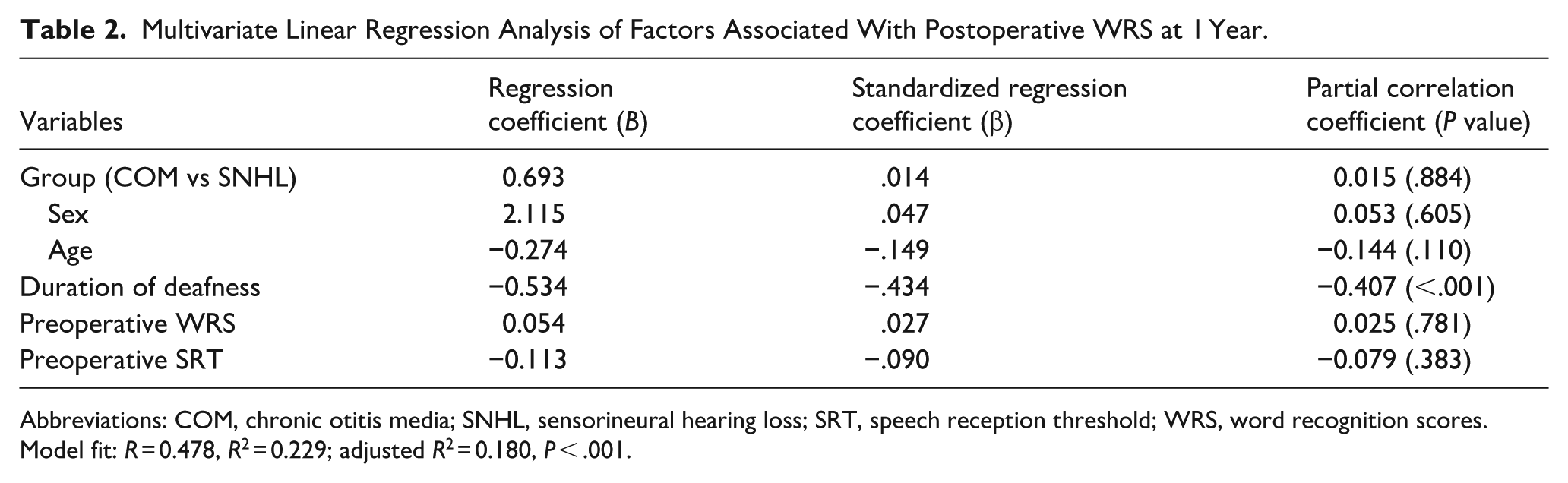
Abbreviations: COM, chronic otitis media; SNHL, sensorineural hearing loss; SRT, speech reception threshold; WRS, word recognition scores.
Model fit: R = 0.478, R2 = 0.229; adjusted R2 = 0.180, P < .001.
In the COM group, patients with labyrinthitis showed a significantly-lower postoperative WRS than both the SNHL group and the COM patients without labyrinthitis, while postoperative PTA4 did not differ significantly among the 3 groups. A post hoc test confirmed significantly-poorer WRS in the labyrinthitis subgroup than in both the SNHL group (P = .007) and the COM without labyrinthitis group (P = .024), whereas no significant difference was observed between the latter 2 groups (Figure 1). When the duration of deafness was evaluated in decades, the SNHL group showed a significant WRS loss above 20 years, whereas no such decline was observed in the COM patients without labyrinthitis (Figure 2). Labyrinthitis was identified in 3 of the current study patients (9.1%) and was associated with a poorer postoperative WRS. All 3 of these cases showed labyrinthitis on both CT and MRI. No patient in the SNHL group demonstrated any radiologic evidence of labyrinthitis. Figure 3 highlights the characteristic CT and MRI findings observed in one of these patients. The COM patients without labyrinthitis showed comparable WRS to the SNHL group (59.3% vs 55.1%).
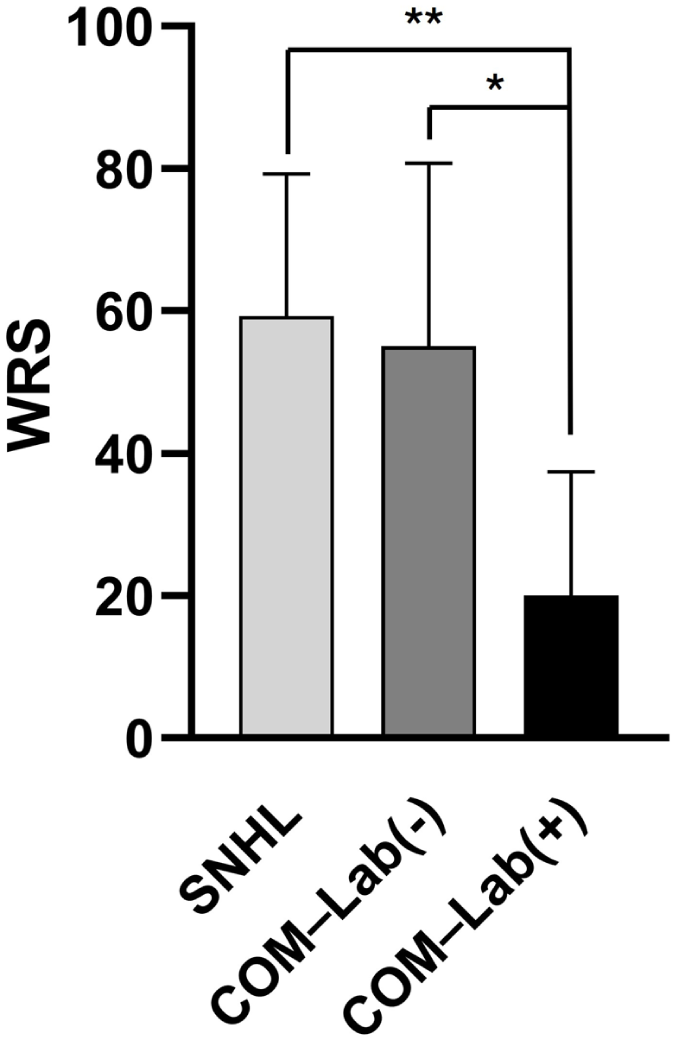
Comparison of the postoperative WRS at 1 year after cochlear implantation in the SNHL group (59.3%), and COM groups without (55.1%) and with (20.0%) labyrinthitis. The WRS was significantly lower in the labyrinthitis patients than in the SNHL group (P = .007) and COM patients without labyrinthitis (P = .024). COM, chronic otitis media; Lab: labyrinthitis; SNHL, sensorineural hearing loss; WRS, word recognition scores.
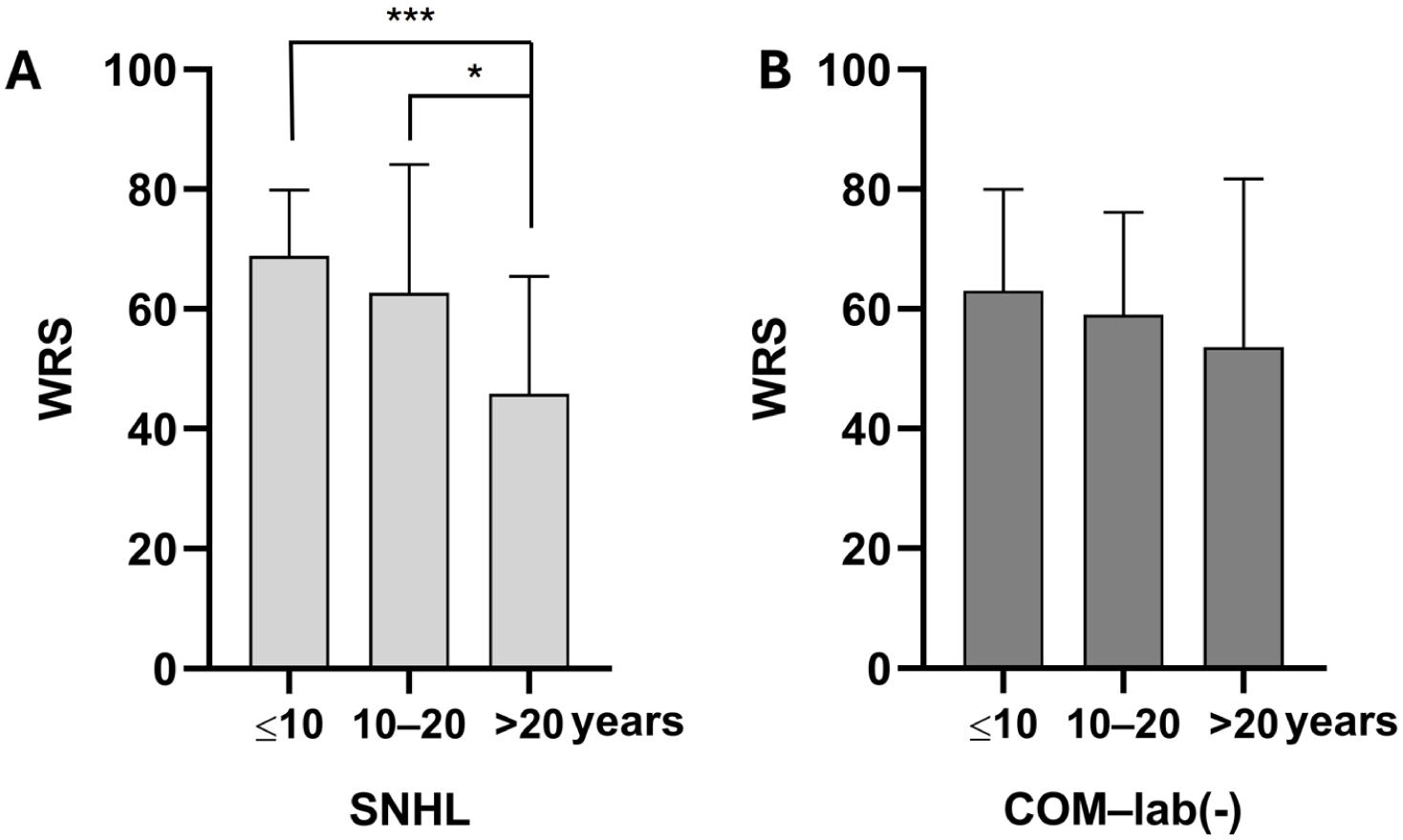
Postoperative WRS according to the DoD. (A) In the SNHL group, the WRS decreased significantly when the DoD exceeded 20 years. (B) In the COM group, patients without labyrinthitis showed no significant difference in their WRS with increasing DoD. DoD, duration of deafness; SNHL, sensorineural hearing loss; WRS, word recognition scores.
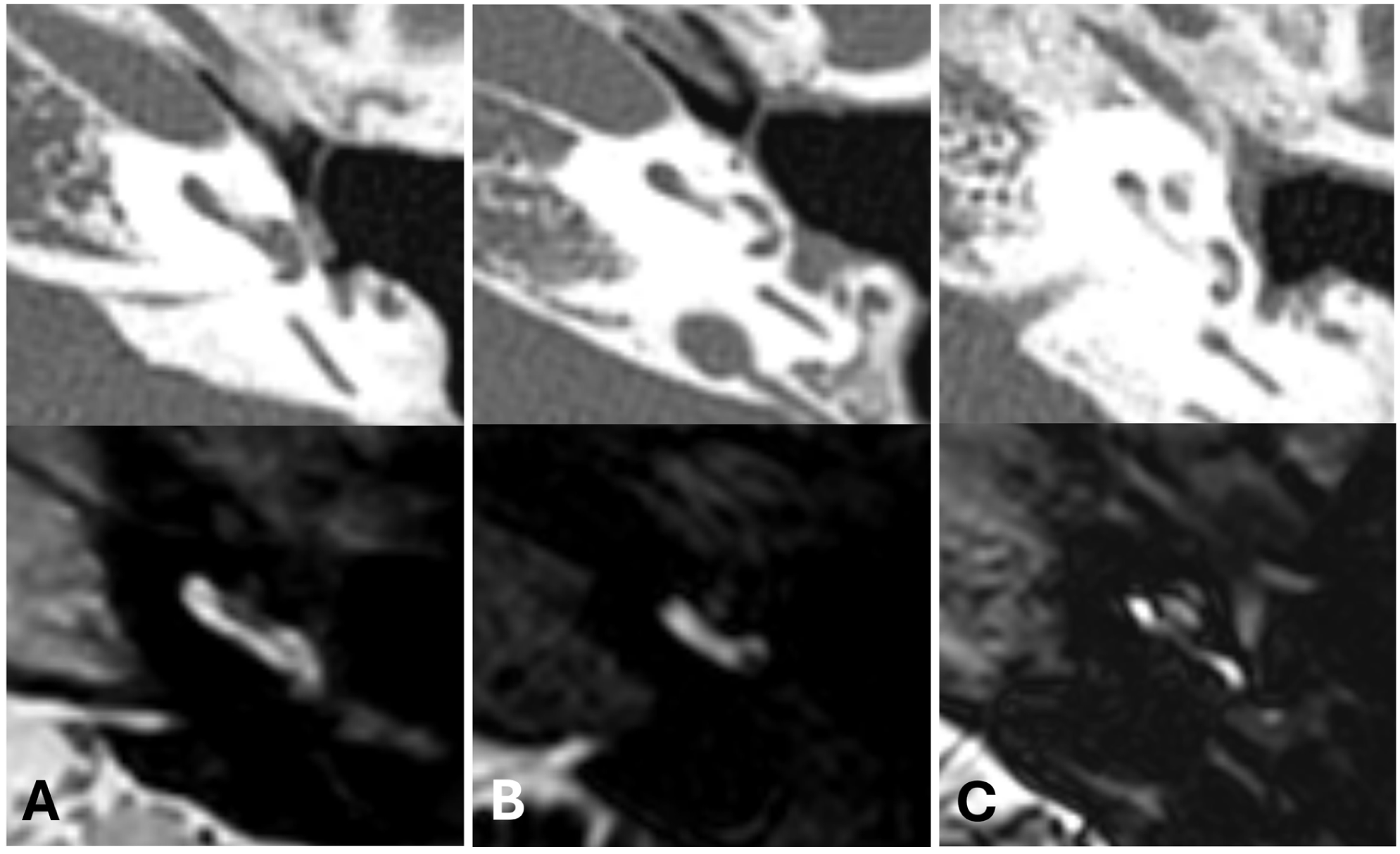
MRI and CT image in patients with patent scala tympani (A) and ossified scala tympani (B, C). New bone formation evident on CT scans (upper panel) could be found in the scala tympani near the round window only (B) and in the whole basal turn of the scala tympani (C). Filling defects in the scala tympani were found on MRI scans at the same sites.
Discussion
We compared postoperative cochlear implant performance between patients with COM with hearing loss and those with noninflammatory SNHL. The COM group demonstrated comparable postoperative WRS to the SNHL group. Notably however, the COM patients with long-term deafness, even above 20 years, showed comparable WRS to those with short-term hearing loss. MRI proved to be a sensitive modality in detecting the presence of labyrinthitis, a condition that had a negative impact on post-cochlear implant performance.
Previous studies have consistently reported that patients with COM can achieve postoperative auditory outcomes comparable to those of standard CI candidates when appropriate surgical management is applied.13 -15 This has been attributed to the refinement and development of the surgical techniques involved, which established the safety of the subtotal petrosectomy approach when performed alongside CI.5,16 -18 In line with these findings, several prior reports demonstrated that the postoperative infection rate in COM ears managed with obliterative procedures was similar to that of ordinary CI cases.19 -23 Consistently, in the present study population, the COM patient implants showed no infection-related complications in our cohort.
This present study also confirmed that the COM group showed comparable cochlear implant performances to the SNHL group. Interestingly, no deterioration of CI performance in patients with long-term deafness of more than 20 years was observed in our patients with COM. In contrast, such a decline in post-cochlear implant performance when the duration of deafness exceeds 20 or 30 years has been observed in SNHL cases.24 -26 We speculate that the better-preserved BC observed in patients with COM may have contributed to this more favorable outcome. In our cohort, multivariate regression analysis similarly identified duration of deafness as the only independent predictor of postoperative WRS. However, despite this negative association in the overall population, COM patients without labyrinthitis did not demonstrate the expected deterioration in performance, even with long-standing deafness. This pattern may reflect relatively-preserved auditory pathway function in patients with COM, potentially supported by residual BC-mediated auditory stimulation. Previous studies have shown that continuous auditory input through hearing aids can support neural integrity within the auditory pathway and improve CI outcomes.27,28 Residual BC hearing in patients with COM may provide a comparable form of stimulation that helps maintain afferent auditory activity.
We additionally found that cases of labyrinthitis as a consequence of long-standing COM had a poor postoperative performance. Patients in our present cohort with evidence of labyrinthitis ossificans on CT or MRI, or with intraoperative findings suggestive of this condition, showed a markedly-lower postoperative WRS, consistent with previous reports.29-31 In this study also, 3 (9%) out of 33 patients had labyrinthitis caused by COM, and all showed findings on both CT and MRI. As partially demonstrated in Figure 3, some lesions were not clearly visualized on CT but appeared as filling defects on MRI, which is consistent with the fibrous stage of labyrinthitis.32,33
This study had some limitations of note. First, measurements of the duration of deafness may have been subject to recall bias, as it relied on subjective reporting by the patients themselves to define the onset of hearing loss, which was not serviceable even with hearing aids. Second, many factors such as individual variations between patients, and differences in surgical techniques, electrode characteristics, and CI mapping parameters could have influenced the outcomes. 34 Additionally, the number of patients with labyrinthitis was small. Future prospective studies with larger sample populations are warranted to validate our current findings and further explore the factors affecting the outcomes in patients with COM undergoing CI.
In conclusion, CI in ears affected by COM yields auditory outcomes comparable to those in non-COM SNHL. Notably in this regard, the COM group cases in this present study maintained a stable WRS even under a prolonged duration of deafness, whereas the normal CI group showed a significant decline in this indicator beyond 20 years of deafness. These findings support performing CI in appropriately-selected patients with COM as a safe and effective procedure, showing resilience of cochlear implant performance even in chronically-diseased ears. Further studies involving standardized surgical protocols are warranted to confirm these results and to further elucidate the mechanisms underlying the preservation of auditory performance in patients with COM despite their long-standing deafness.
Footnotes
Ethical Considerations
The study protocol was approved by the Institutional Review Board of Asan Medical Center (IRB no 2023-1512). Informed consent was waived by the IRB. The study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
Conceptualization: H.J.P. Data curation: T.U.C., J.Y.G., S.S.R., D.Y.K. Formal analysis: T.U.C., H.J.P. Methodology: T.U.C., J.Y.G., S.S.R., D.Y.K., H.J.P. Project administration: H.J.P. Visualization: T.U.C., J.Y.G., S.S.R., D.Y.K. Writing – original draft: T.U.C. Writing – review and editing: T.U.C., H.J.P. All authors read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Asan Medical Center (2021IF0005).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.