
Abstract
Objective
The assessment of bone conduction thresholds in patients with conductive hearing loss is not a full measure of the function of the inner ear due to the weakening of the influence of middle ear components on bone conduction. This relationship has been called the ‘Carhart effect’.
Methods
The retrospective analysis covered 977 patients diagnosed and treated for middle ear diseases from 2010 to 2020. The Carhart effect was considered to be an increase in the bone conduction threshold by a minimum of 10 dB relative to adjacent frequencies. The study was performed with the aim of assessing the presence of the Carhart effect in the course of middle ear diseases in pretreatment analysis.
Results
The Carhart effect was observed in 532 cases, most often in patients with chronic otitis media and otosclerosis. It was least often observed in patients with otitis media with effusion. In otitis media with effusion, the Carhart effect was more often noted for the frequency of 4000 Hz, in otosclerosis for the frequency of 2000 Hz. In patients with chronic otitis media, this effect for the frequency of 4000 Hz was correlated with the location of inflammatory changes in the attic area. The presence of inflammatory lesions in the oval window area was associated with the presence of the Carhart effect for the frequency of 2000 Hz.
Conclusions
1. The frequency of the Carhart effect observed in diseases of the middle ear does not depend on the disease entity but on the type and location of abnormalities in the middle ear. 2. The Carhart effect observed for the frequency of 4000 Hz coexists with the localization of lesions in the range of the malleus and incus, and for the frequency of 2000 Hz, it is partially associated with abnormalities in the range of stapes and oval window.
Introduction
According to Tonndorf's theory, bone conduction thresholds are determined by three components. The first is the vibration of the skull bones, which, by stimulating the bony labyrinth, causes distortions of the membranous labyrinth and then stimulates the auditory receptors. 1
The assessment of bone conduction thresholds in patients with conductive hearing loss is not a full measure of the function of the inner ear due to the weakening of the influence of the above-described components of bone conduction. In the course of diseases of the middle ear, such as chronic otitis media, otitis media with effusion, and otosclerosis, the influence of the sound transmission system in the middle ear on the inner ear is weakened, which in some patients is reflected in the shift of the bone conduction threshold curve. This relationship has been called the ‘Carhart effect’.
This phenomenon owes its name to Raymond Carhart, who in 1950 described an increase in the bone conduction threshold in an audiometric study for the 2000 Hz frequency in patients with otosclerosis.2,3 The increase in the bone conduction threshold in patients in this case was conventionally called ‘Carhart's notch’. Subsequent studies confirmed that a similar increase in the bone conduction threshold in the frequency range of 500–4000 Hz was observed in other middle ear diseases that limit the mobility of the auditory ossicles, such as chronic otitis media or otitis media with effusion.4-7 Due to the commonness of the phenomenon in diseases of the middle ear, Gatehouse proposed extending the term ‘notch’ to the ‘Carhart effect’ to cover all pathologies in which it occurs. 8
Treatment of diseases of the middle ear not only removes the abnormalities of this part of the auditory pathway but also in many cases leads to a measurable improvement in bone conduction, often in the range of repetitive frequencies typical of the type of disease. The observed relationship explains the need for this study and further analyses.
The study was performed with the aim of assessing the presence of the Carhart effect in the course of middle ear diseases by an audiometric assessment performed before starting treatment.
Materials and methods
The retrospective analysis covered 977 patients diagnosed and treated for middle ear diseases from 2010 to 2020. The study included 241 patients with otitis media with effusion (OME), 226 patients treated for otosclerosis (OTO), and 510 patients operated on for chronic otitis media (OMC). In the group of patients with chronic otitis media, subgroups were distinguished depending on the type of abnormalities observed: chronic simple otitis media (a total of 236 patients, which is 46.2% of all patients with OMC), chronic otitis media with the presence of inflammatory granulation tissue (110 patients, which is 21.6% of all patients with OMC), and chronic cholesteatoma otitis media (164 patients, which is 32.2% of all examined patients with OMC).
Age of Patients in Considered Diseases of the Middle Ear.
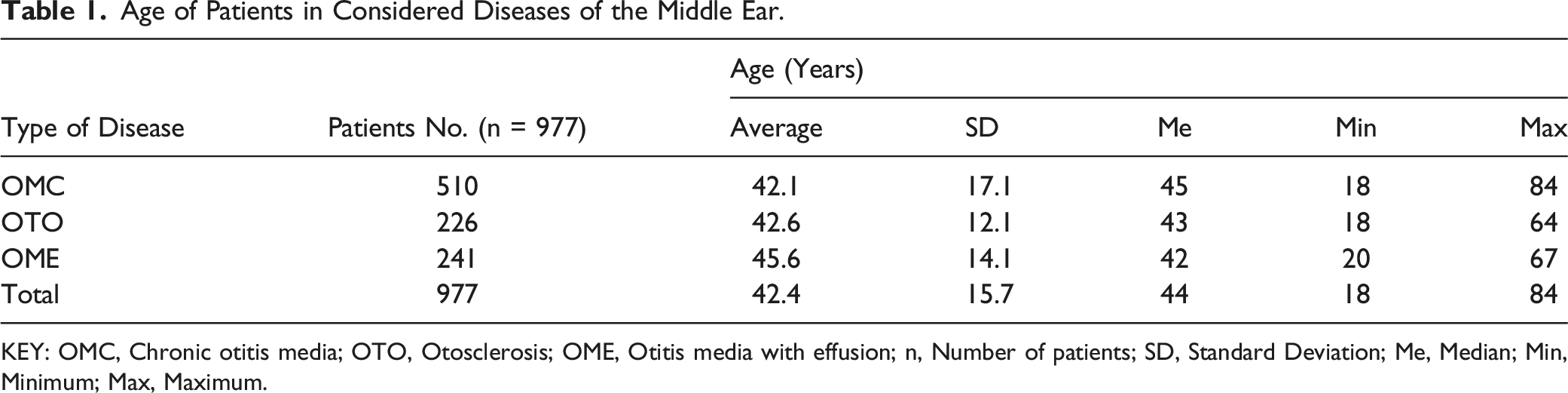
KEY: OMC, Chronic otitis media; OTO, Otosclerosis; OME, Otitis media with effusion; n, Number of patients; SD, Standard Deviation; Me, Median; Min, Minimum; Max, Maximum.
Gender of the Analysed Patients With Middle Ear Diseases.
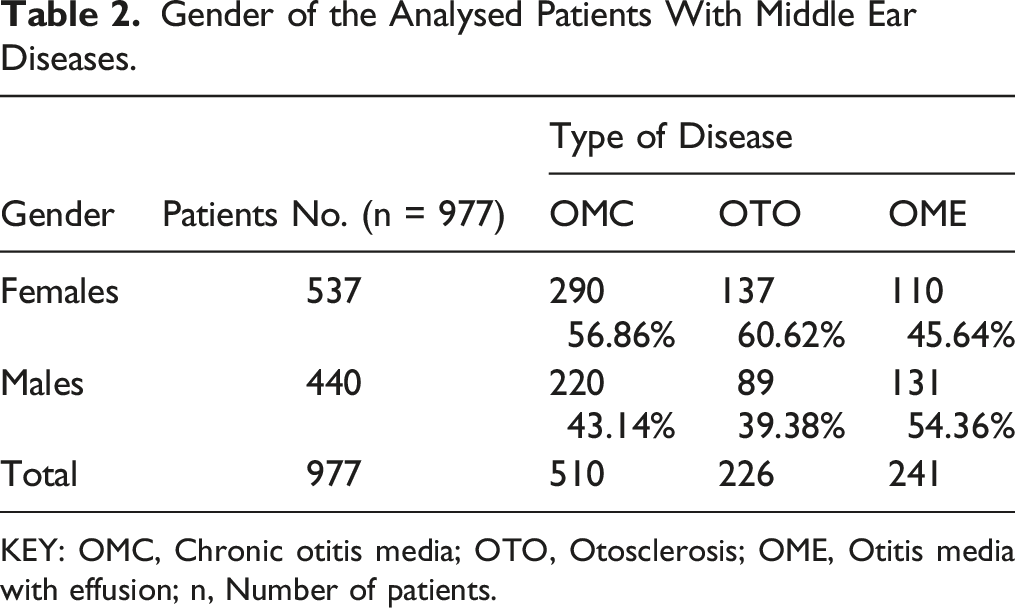
KEY: OMC, Chronic otitis media; OTO, Otosclerosis; OME, Otitis media with effusion; n, Number of patients.
The criteria for inclusion in the study were as follows: age over 18 years, presence of chronic otitis media, otosclerosis or otitis media with effusion and informed consent of the patient to participate in the study.
The criteria for exclusion from the study were as follows: condition after acoustic trauma, condition after head or craniofacial trauma, congenital ear diseases, previous middle ear surgery, refusal to participate in the study, and patient death.
Surgical treatment was performed by three otosurgeons with similar experience in operations on the middle ear using the same surgical technique and instruments. This made it possible to treat the analysed patients as a homogeneous group. The same surgical procedures were performed according to the same methodology using the same tools.
Pure-tone audiometry was performed in all patients by the same team of technicians. The study considered the results obtained immediately before treatment in the otolaryngology department and during follow-up examinations in the period of 18 to 24 months after treatment. The tests were performed in a soundproof and sound-absorbing room using a MIDIMATE 622 Audiometer (Madsen, Budapest, Hungary) and TDK 39 headphones (TDH, Tokyo, Japan). The audiometer met the standards for air and bone conduction measurements (ISO ISO0389-1985 and ISO7566-1987, respectively). The air conduction (AC) threshold was measured at 250 Hz, 500 Hz, 1 kHz, 2 kHz, 3 kHz, 4 kHz, and 8 kHz, and the bone conduction (BC) threshold was measured at 0.5 kHz, 1 kHz, 2 kHz, 3 kHz, and 4 kHz.
The Carhart effect was considered to be an increase in the bone conduction threshold by a minimum of 10 dB relative to adjacent frequencies.2,3
All patients included in the analysis gave their informed consent to participate in the study. The project was approved by the local Bioethics Committee (no. 1072.6120.116.2021).
The obtained results were subjected to statistical analysis. The result analysis was carried out using the STATISTICA 13 suite (StatSoft Polska, Kraków, Poland). Chi-squared test, Pearson’s linear correlation, Student’s t test, and one-way analysis of variance with small group adjustments were used. Statistically significant results of the variance analysis were examined posthoc using Tukey’s test.
Statistical significance was established at P < .05.
Results
Average Bone Conduction Thresholds Before and After Treatment in Considered Diseases of the Middle Ear.

KEY: OMC, Chronic otitis media; OTO, Otosclerosis; OME, Otitis media with effusion; n, Number of patients; BC, Bone conduction threshold; dB, decibel.
Percentage of Patients With the Carhart Effect by Middle Ear Disease.
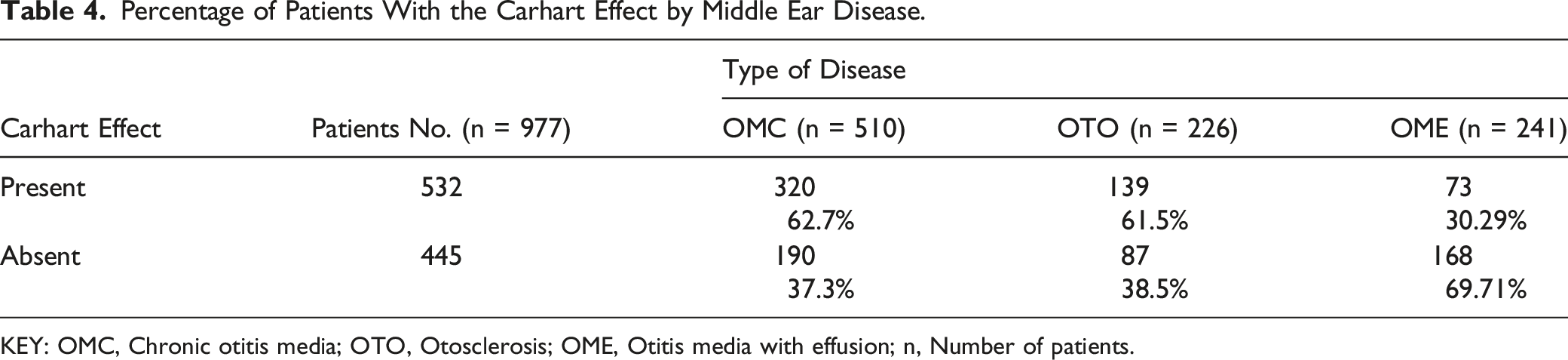
KEY: OMC, Chronic otitis media; OTO, Otosclerosis; OME, Otitis media with effusion; n, Number of patients.
Frequency at Which the Occurrence of the Carhart Effect was Observed in the Analysed Groups of Patients.
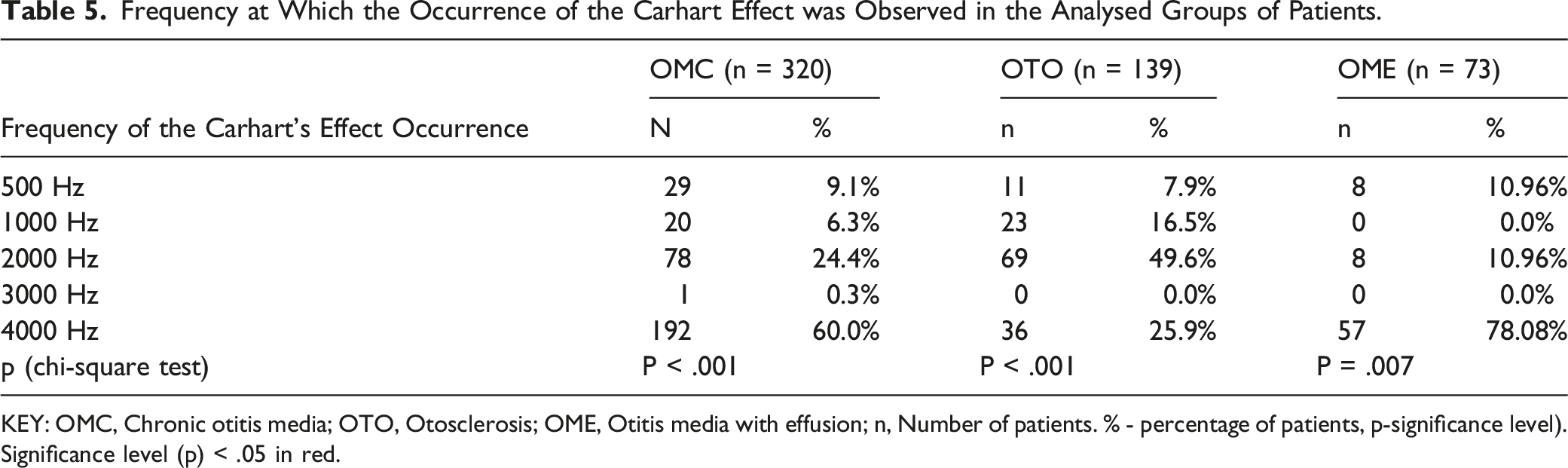
KEY: OMC, Chronic otitis media; OTO, Otosclerosis; OME, Otitis media with effusion; n, Number of patients. % - percentage of patients, p-significance level). Significance level (p) < .05 in red.
In chronic otitis media, the Carhart effect was present in more than half of the subjects (62.7%). In this group, the Carhart effect was observed significantly more often (P < .001) for the frequency of 4000 Hz.
In patients with otosclerosis, the Carhart effect was statistically significantly (P < 0.001) dependent on the resonant frequency of the ossicular chain. The Carhart wave occurred in almost half of the subjects (49.6%) at 2000 Hz.
In otitis media with effusion, the Carhart effect was statistically significantly more frequent compared to other frequencies (P = .007) for 4000 Hz. In this group, in more than ¾ of the subjects (78.08%), the Carhart effect was observed for 4000 Hz. In nearly 11% of patients, the Carhart effect was present at 500 and 2000 Hz.
Percentage of Patients With the Carhart Effect in Patients With Chronic Simple Otitis Media, Chronic Otitis Media With Inflammatory Granulation Tissue, and Chronic Cholesteatoma Otitis Media.
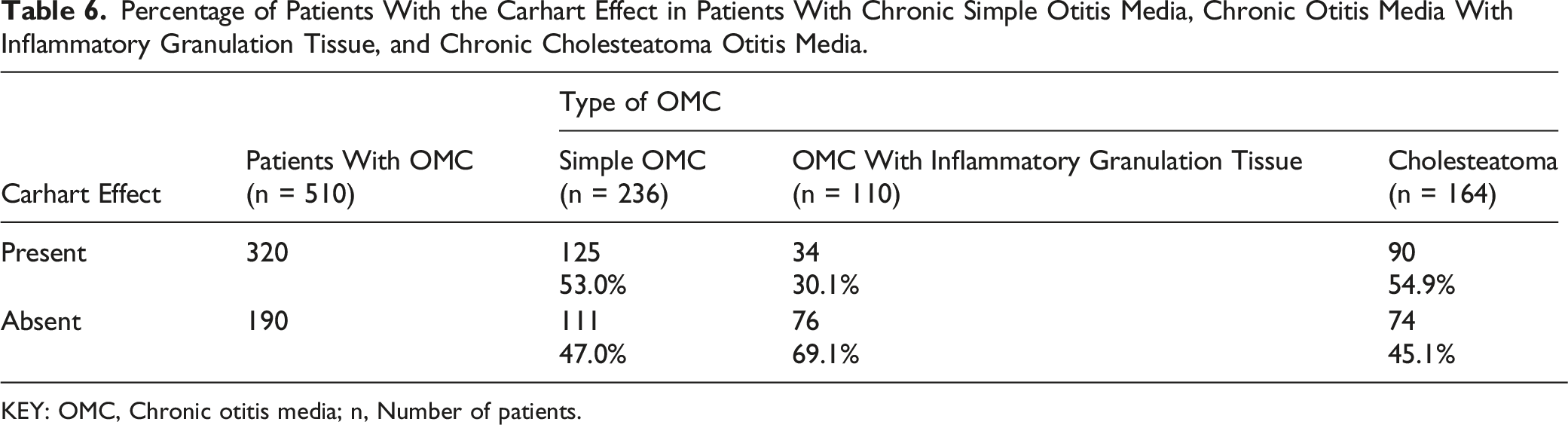
KEY: OMC, Chronic otitis media; n, Number of patients.
Among patients with chronic simple inflammation, 2 additional groups were distinguished: • with adhesions in the absence of other lining abnormalities (83 patients, which was 35.3% of patients with simple OMC), and • with chain disconnection in the absence of other abnormalities (44 patients, which accounted for 18.64% of all patients with simple OMC). In further analysis, the behaviour of the Carhart effect in the course of chronic otitis media in its various forms was considered.
The Carhart effect was statistically significantly (P = .011) correlated with the presence of cholesteatoma. In the analysed material, cholesteatoma changes in the area of the attic in the immediate vicinity of the auditory ossicular chain were significantly more frequent. Changes in the bone conduction threshold corresponding to the adopted criteria for the description of the Carhart effect were found in 90 patients with cholesteatoma, which corresponds to nearly 55% of patients with this type of chronic inflammatory change.
The Occurrence of the Carhart Effect in the Case of Chronic Cholesteatoma Otitis Media Compared to Other Types of OMC.
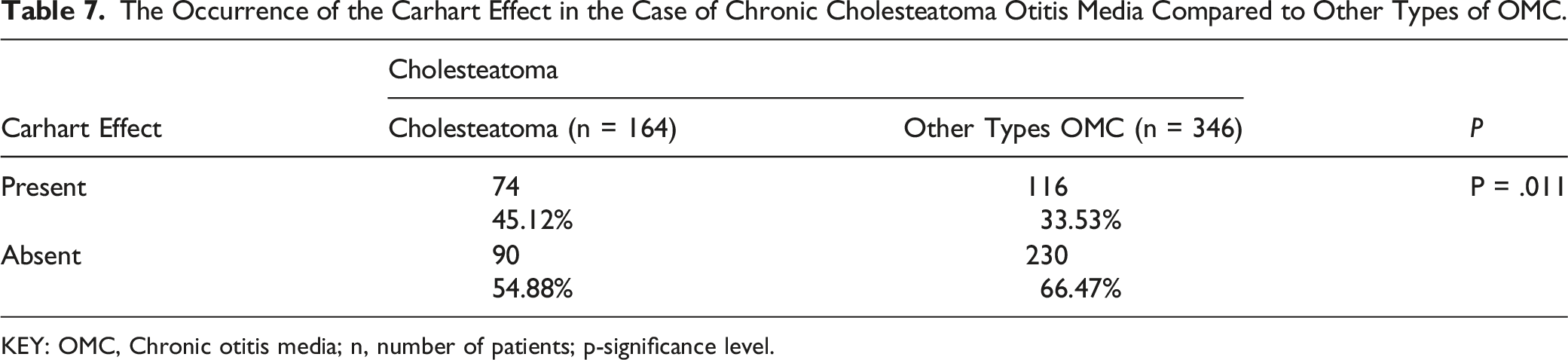
KEY: OMC, Chronic otitis media; n, number of patients; p-significance level.
Frequencies for Which the Carhart Effect was Observed in the Course of Chronic Cholesteatoma Otitis Media.
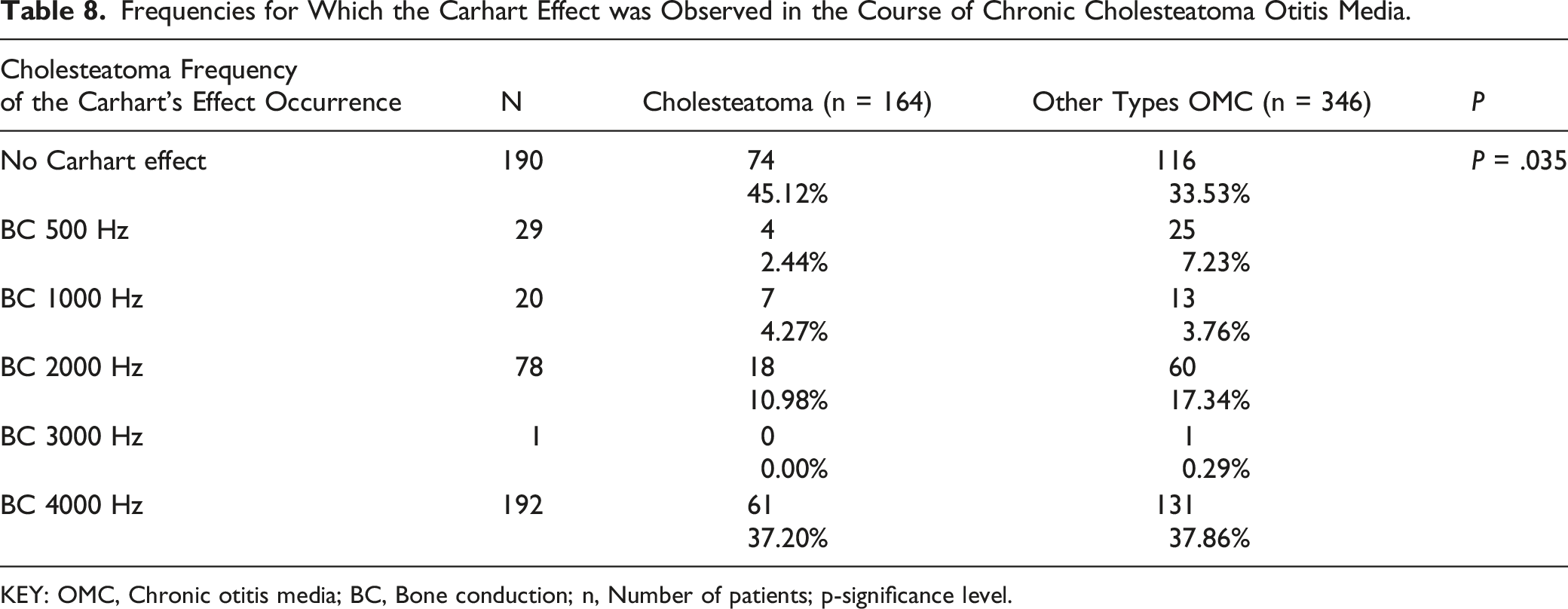
KEY: OMC, Chronic otitis media; BC, Bone conduction; n, Number of patients; p-significance level.
The occurrence of the Carhart Effect in the Case of Chronic Otitis Media With the Presence of Inflammatory Granulation Tissue Compared to Other Types of OMC.
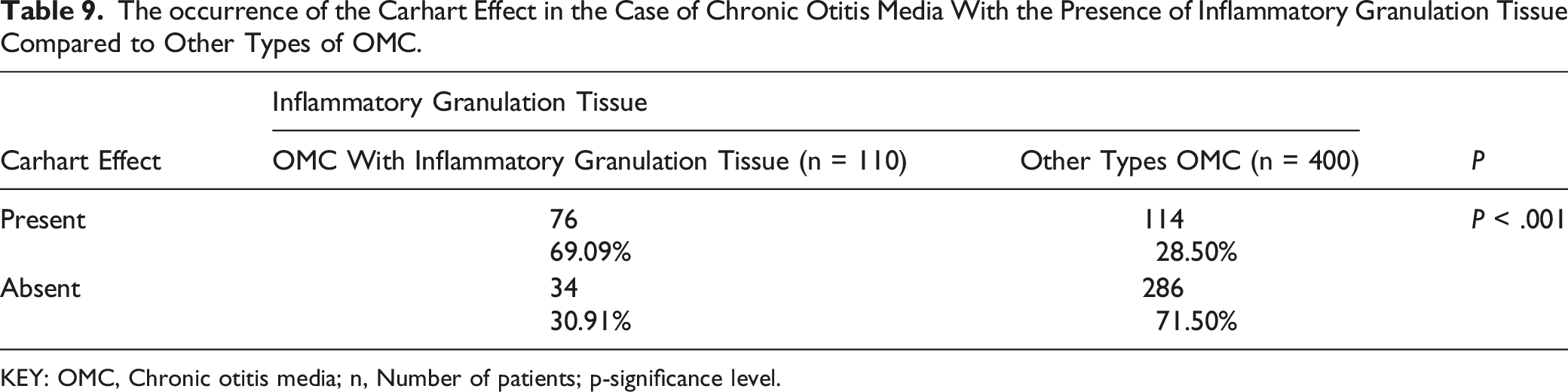
KEY: OMC, Chronic otitis media; n, Number of patients; p-significance level.
Frequencies for Which the Carhart Effect was Observed in the Course of Chronic Otitis Media With Inflammatory Granulation Tissue.
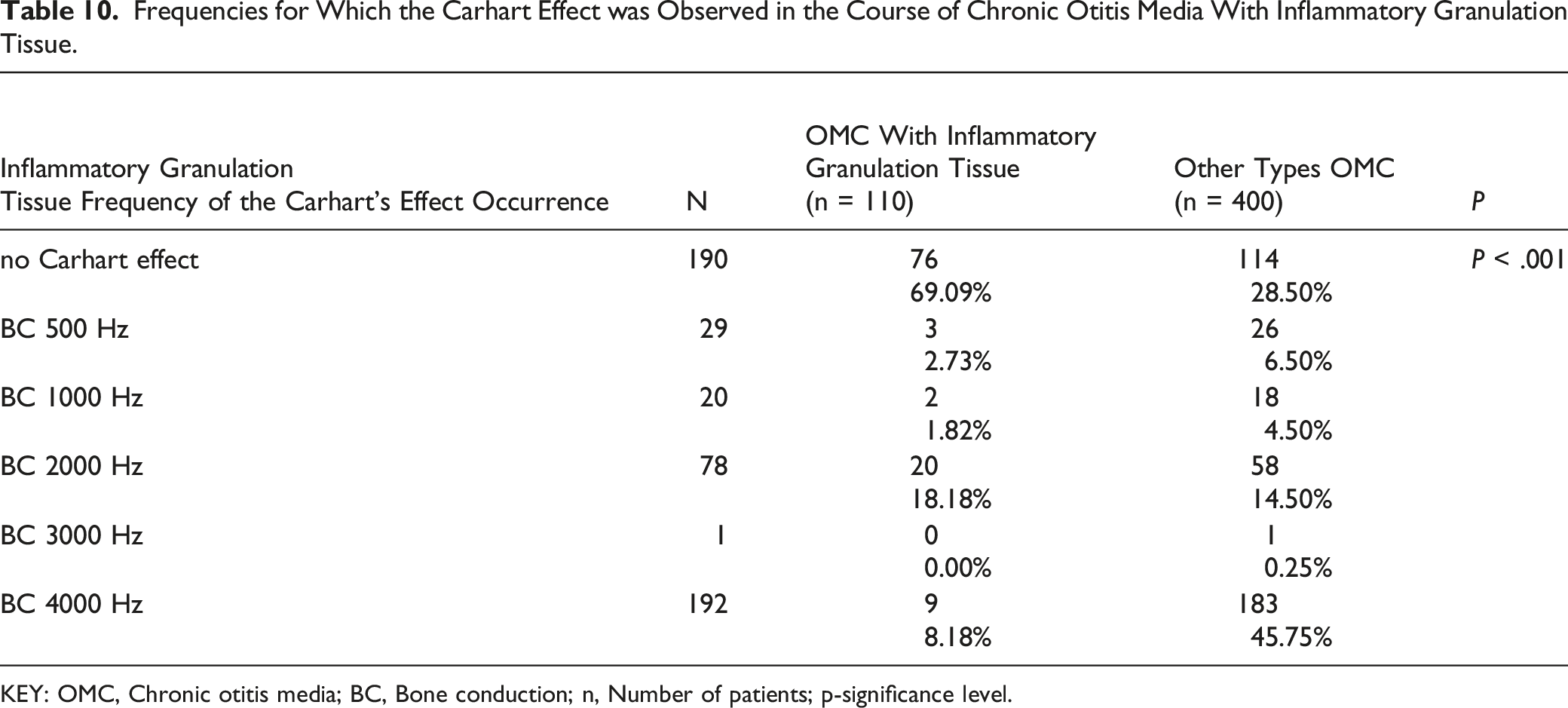
KEY: OMC, Chronic otitis media; BC, Bone conduction; n, Number of patients; p-significance level.
In the next step, the behaviour of the Carhart effect in chronic simple otitis media was considered.
After excluding patients with other abnormalities in chronic simple otitis media (e.g. hypertrophy of the mucosa and polypoid mucosa), 83 patients with synechiae in the tympanic cavity were analysed as the only abnormality in the course of chronic simple otitis media. In this group, the Carhart effect occurred in 53 subjects.
Occurrence of the Carhart Effect in the Case of Adhesions That Reduce the Mobility of the Ossicular Chain in the Course of Chronic Simple Otitis Media.
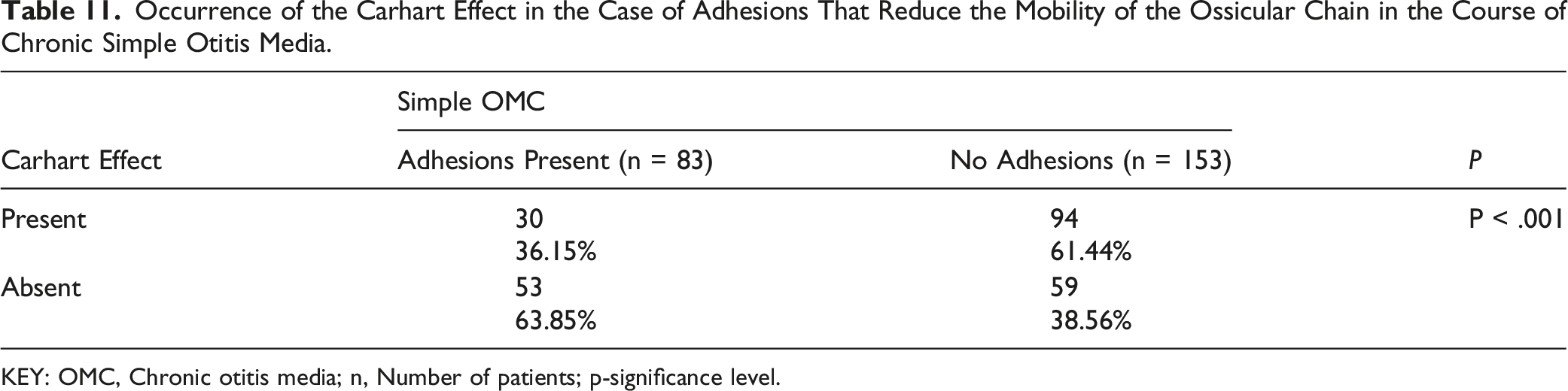
KEY: OMC, Chronic otitis media; n, Number of patients; p-significance level.
Frequencies at Which the Carhart Effect was Observed in the Case of Adhesions as the Only Abnormality in the Course of Chronic Simple Otitis Media.
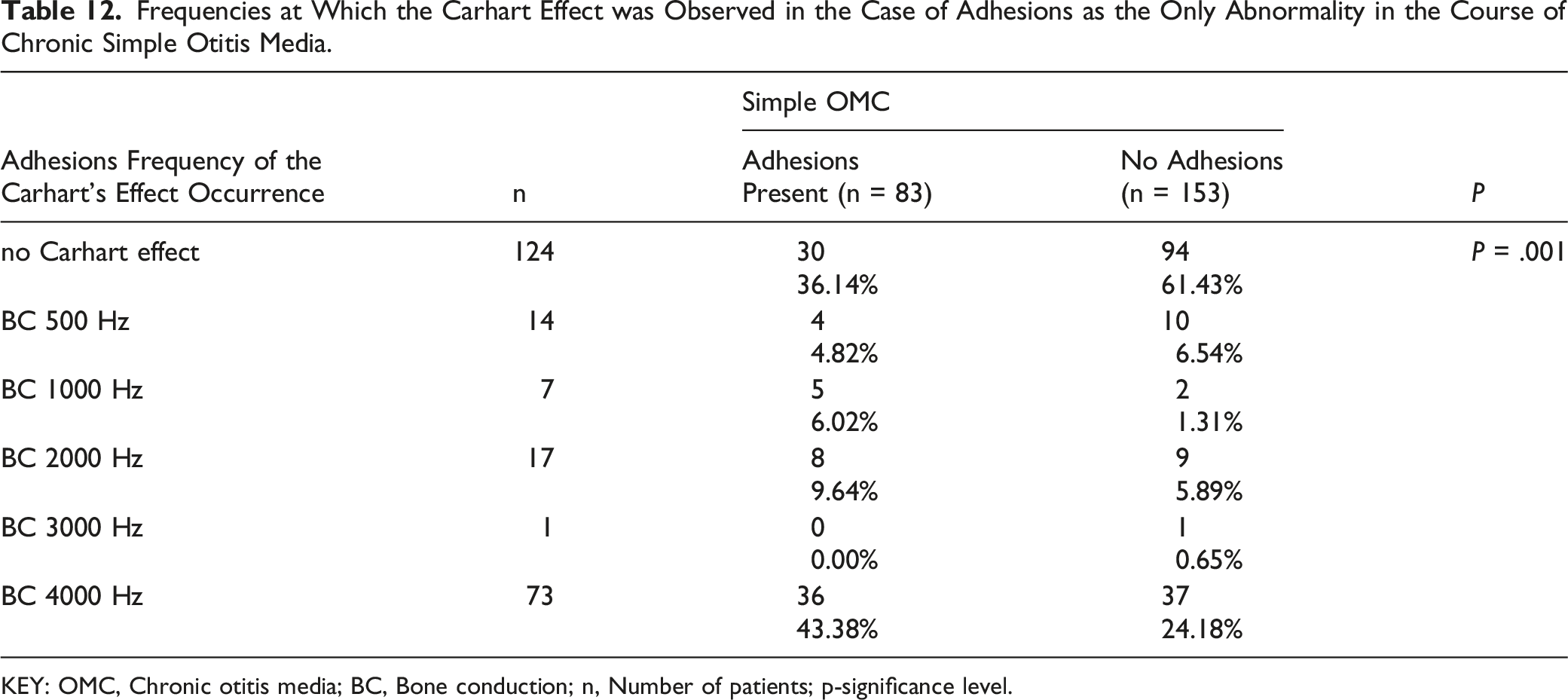
KEY: OMC, Chronic otitis media; BC, Bone conduction; n, Number of patients; p-significance level.
The influence of ossicular chain disconnection in the course of chronic simple otitis media on the occurrence of the Carhart effect was also analysed. The conducted analysis showed no statistically significant relationship between the disconnection of the ossicular chain and the occurrence of the Carhart effect (P = .238).
Discussion
The authors of the study, analysing the change in bone conduction thresholds in a group of patients with middle ear diseases such as otitis media with effusion, otosclerosis, or chronic otitis media, found the presence of the Carhart effect in 532 cases, which is 54.5% of all analysed patients. The Carhart effect was least often observed in patients with otitis media with effusion (30.29%); in otosclerosis, it was found in 61.5%, and the Carhart effect was most often seen in patients with chronic otitis media (62.7% of all OMCs).
The incidence of the Carhart effect in chronic otitis media with effusion, according to various authors, ranged from 25.3% to 35.8% and spanned the frequency of 2000 Hz (94% of cases).9,10 Single, statistically insignificant cases included a frequency of 4000 Hz. 6
In our observation, the Carhart effect in otitis media with effusion was significantly more often observed for the frequency of 4000 Hz (78.08% of cases) and in individual cases for 500 and 2000 Hz.
Most authors described the Carhart effect in the case of OME in the presence of thick and abundant exudate, as opposed to the group with serous, watery exudate, in which the Carhart effect was not observed. 6 Comparison of the results with other studies is difficult because the studies concerned patients belonging to the developmental age group, as opposed to the group of adult patients, with an average age of 42 years, analysed in our study.9,11
The disturbance of mobility at the base of the stapes in the oval window is conducive to the presence of the Carhart effect for 2000 Hz. In our observation, the Carhart effect affected 49.6% of all patients with otosclerosis and was most often observed at the frequency of 2000 Hz; in a significant percentage of patients, it also affected the frequency of 4000 Hz (25.9%). The presence of the Carhart notch at 2000 Hz was comparable to the reports in the available literature, while other authors rarely described the Carhart effect at 4000 Hz.12,13
The presence of the Carhart effect in the course of otosclerosis for the frequency of 4000 Hz may result from disturbances in the effective vibration of the ossicular chain by immobilizing the base of the stapes in the oval window and the resulting stiffness of the ossicular chain. 14
The Carhart effect for the frequency of 4000 Hz was also observed by the authors in 37.2% of patients with chronic cholesteatoma otitis media. In the analysed material, cholesteatoma changes were observed significantly more often in the attic area in the immediate vicinity of the ossicular chain. The presence of cholesteatoma masses in the oval window area was associated with the presence of the Carhart effect for the frequency of 2000 Hz and affected 10.98% of patients with chronic cholesteatoma otitis media. Localization of cholesteatoma masses in the round or oval window presses on the secondary tympanic membrane or the base of the stirrup, reduces the movement of the fluid in the inner ear, and mechanically affects the mobility of the stapes.
Mejzlik J et al. observed the influence of the location of cholesteatoma masses on changes in the value of bone conduction thresholds. Changes in the postoperative bone conduction threshold for frequencies of 500, 1000, and 2000 Hz were typical for cholesteatoma located in the mastoid process, while the presence of cholesteatoma masses in the attic was statistically significantly correlated with the change in bone conduction thresholds for the frequency of 4000 Hz. For other cholesteatoma locations, no effect on bone conduction threshold values was found. 15
The Carhart effect at 2000 Hz has also been observed for chronic otitis media with inflammatory granulation tissue. Increasing the bone conduction threshold in the range of 2000 Hz affected almost 60% of patients with the Carhart effect in this group of patients. The mechanism of these changes seems to be similar to cholesteatoma lesions located in the vicinity of the oval or round window and similar to otosclerosis.
In the case of chronic simple otitis media, the presence of the Carhart effect in our observation depended on the presence of synechiae in the tympanic cavity. Immobilization of the ossicular chain by the presence of adhesions, mainly in the malleus and promontorium, significantly increased the bone conduction threshold to 4000 Hz. This mechanism seems to be similar to the previously described immobilization of the ossicular chain in the range of the malleus in cholesteatoma of the attic. 16
In our observation, the analysis of the effect of ossicular chain disconnection on bone conduction threshold values in the course of chronic simple otitis media did not show a statistically significant relationship. Lee et al. showed that removal of the lesions alone without reconstruction of the ossicular chain (in the first stage of the two-stage operation) does not improve postoperative bone conduction values. 17 Similar observations were made by Linstrom et al., who noted an improvement in the bone conduction threshold from 4.0 to 9.3 dB across a range of frequencies in patients undergoing ossicular reconstruction, with the highest average improvement observed for the frequency of 2000 Hz. 18
Measurement of bone conduction and air conduction thresholds is an integral part of the audiological assessment of middle ear disease.
Disease processes that disturb the mechanism of sound conduction through the middle ear, apart from increasing the air conduction threshold, also have an adverse effect on the bone conduction threshold values.
This phenomenon was observed between 500 and 4000 Hz, with the highest value being reached for the frequency of 2000 Hz. 19
Elevation of the bone conduction threshold in the range of 2 kHz mainly characterizes disease states associated with otosclerotic changes and immobilization of the base of the stapes in the oval window. Immobilization of the stapes in the oval window as a result of the development of otosclerotic foci contributes to the increase in rigidity of the ossicular chain, inhibits its effective vibration, and changes the mechanics of the distribution of forces along the ossicular chain. 20
The mechanism of increasing the bone conduction threshold in cases of chronic otitis media is not fully understood. In studies of the influence of middle ear mechanics on the value of bone conduction in patients with chronic otitis media, three different modes have been described: compression, inertial, and osteomuscular. In compression mode, sound-induced vibrations of the skull directly cause the fluids of the inner ear to vibrate. The ossicular chain is not involved in this mode, unlike in inertial and osseotympanic movements. 17
Preoperative bone conduction threshold measurement for conductive hearing loss due to outer or middle ear pathology is not a complete measure of inner ear function. Huizing experimentally proved this variability of the bone conduction threshold and called this phenomenon middle ear bone conduction loss or pseudoperceptual deafness. Gatehouse defined this behaviour of the bone conduction threshold as the Carhart effect.8,21
Mechanical occlusion of the round window with inflammatory granulation tissue, ossicular chain motility disorder due to inflammatory changes, ossicular chain abnormalities, and tympanic membrane perforation seem to be the basic mechanical factors affecting bone conduction thresholds in chronic otitis media.
The observations of Paparella et al. showed that in addition to the component related to the involvement of the middle ear in the development of sensorineural hearing loss in chronic otitis media, the spread of inflammation to the inner ear also plays an important role. 22 Browning and Gatehouse, on the other hand, showed that elevated bone conduction thresholds in chronic otitis media probably reflect the Carhart effect and not damage to the inner ear. 23
Similar observations were made by Walbyet et al, who emphasized that there is no evidence that the inflammatory factors found in chronic otitis media cause damage to hair cells or cochlear neurons. Their results show that the extension of inflammation to the inner ear is not the main cause of the sensorineural component of hearing loss in chronic otitis media. In this condition, the Carhart effect, which refers to an increase in the bone conduction threshold, seems to be a consequence of conductive hearing loss. 24
The influence of the mechanics of the middle ear on the function of the inner ear is an important issue in clinical practice that should be taken into account in audiological diagnostics when assessing the function of the sensorineural part of the hearing organ before treatment of diseases involving the middle ear.
Conclusions
1. Threshold values of bone conduction in diseases of the middle ear are derived from the activity of the sensory-nervous part of the hearing organ and the Carhart effect, which describes the impact of the disease process taking place in the middle ear on the change in the threshold of bone conduction. 2. The frequency of the Carhart effect observed in diseases of the middle ear does not depend on the disease entity but on the type and location of abnormalities in the middle ear. 3. The Carhart effect observed for the frequency of 4000 Hz coexists with the localization of lesions in the range of the malleus and incus, and for the frequency of 2000 Hz, it is partially associated with abnormalities in the range of the stapes and oval window.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.