
Abstract
Myeloid sarcoma (MS) is a rare extramedullary myeloid malignancy that may occur with or without bone marrow involvement. Nasopharyngeal cases are exceedingly rare, making diagnosis challenging, and most reported cases present with local symptoms caused by a bulky mass. We report a 64-year-old man with a history of myelodysplastic syndrome who presented with cervical lymphadenopathy without any nasal or otologic symptoms. Endoscopic examination revealed a small, smooth bulging lesion on the left nasopharyngeal wall. Contrast-enhanced computed tomography demonstrated a polypoid mass with bilateral cervical lymphadenopathy. Histopathological and immunohistochemical analyses confirmed MS. Bone marrow evaluation revealed leukemic transformation to acute myeloid leukemia. The patient received combination chemotherapy with venetoclax and azacitidine but died 2 months after treatment initiation. This asymptomatic presentation emphasizes the diagnostic difficulty of MS arising in atypical anatomical locations. Early tissue biopsy and prompt hematologic assessment are essential for accurate diagnosis and timely management. Nasopharyngeal MS should be considered in the differential diagnosis of nasopharyngeal masses, particularly in patients with a history of myelodysplastic or myeloproliferative disorders.
Keywords
Introduction
Myeloid sarcoma (MS) is a rare extramedullary tumor characterized by the proliferation of myeloid blasts that disrupt the normal architecture of affected tissues. The organs most frequently involved include the skin, lymph nodes, gastrointestinal tract, bone, and central nervous system.1 -3 MS can occur concurrently with acute myeloid leukemia (AML) or present as a manifestation of relapsed AML or develop as a progression of a preexisting myeloproliferative disorder. 4 Although MS can arise in virtually any anatomical site, nasopharyngeal localization is particularly uncommon, posing considerable diagnostic challenges. Its rarity and nonspecific clinical manifestations often delay accurate diagnosis.
Here, we report a rare case of nasopharyngeal MS in a patient with a history of myelodysplastic syndrome (MDS) who presented with cervical lymphadenopathy. This case underscores the importance of maintaining a high index of clinical suspicion and performing prompt diagnostic evaluation when MS is encountered in atypical anatomical sites.
Case Report
A 64-year-old man with a history of MDS previously treated with chemotherapy presented to the otolaryngology department with a palpable mass on the left side of the neck. Endoscopic examination revealed a smooth, whitish-to-yellowish, elevated bulging lesion on the left upper nasopharyngeal wall (Figure 1). Both tympanic membranes appeared normal.
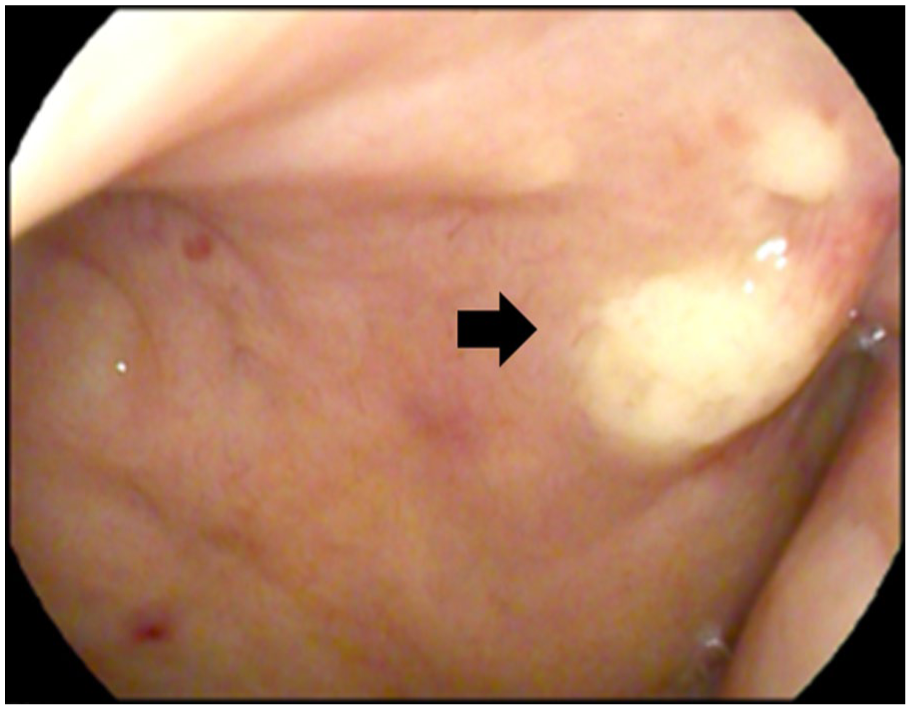
Endoscopic image showing a smooth, whitish-yellow, bulging lesion arising from the left upper nasopharyngeal wall.
A non-tender, palpable mass ~1 cm in diameter was noted in the left level III cervical region, and additional palpable masses in both inguinal areas. Complete blood count revealed a white blood cell count of 156 900/μL, hemoglobin of 7.5 g/dL, and platelet count of 63 000/μL. Given the abnormal hematologic profile and prior history of MDS, a punch biopsy of the nasopharyngeal lesion was performed.
Contrast-enhanced neck computed tomography (CT) demonstrated a polypoid mass arising from the left nasopharynx wall with bilateral cervical lymphadenopathy (Figure 2). Histopathological examination of the biopsy specimen confirmed the diagnosis of MS. Immunohistochemistry analysis showed positivity for leukocyte common antigen (LCA), myeloperoxidase (MPO), CD33, lysozyme, and CD68, while cytokeratin, C-kit, CD20, and CD3 were negative. BCL-2 expression was 15%, CD10 was negative, and the Ki-67 labeling index was 70%. Epstein-Barr virus (EBV) in situ hybridization was negative.
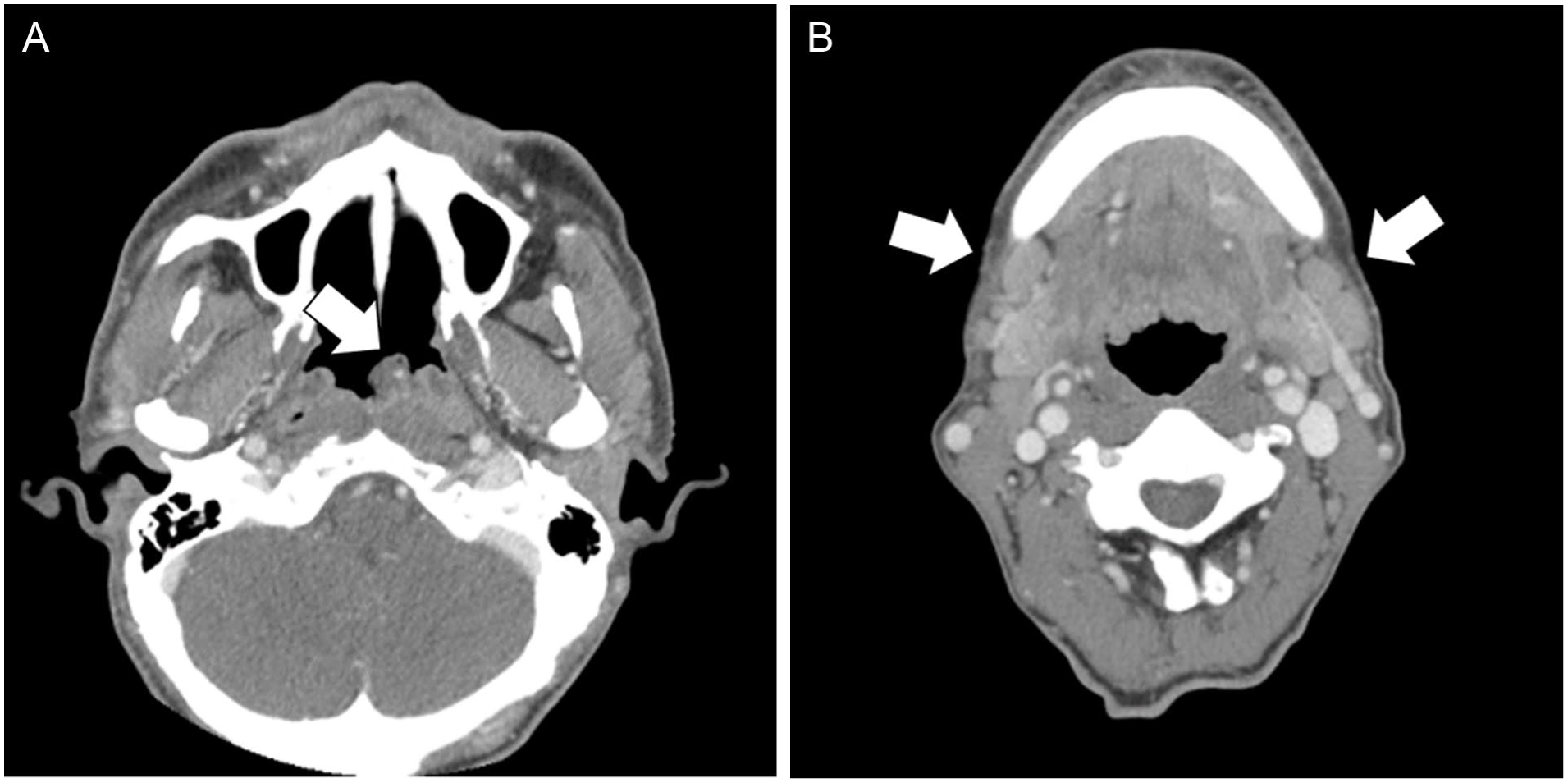
Contrast-enhanced neck CT images demonstrating (A) a polypoid mass (arrow) in the left nasopharynx and (B) bilateral cervical lymphadenopathy (arrows). CT, computed tomography.
The patient was subsequently referred to the hematology department, where bone marrow evaluation confirmed leukemic transformation to AML, with a blast percentage of 20%. The patient underwent 2 partial cycles of combination chemotherapy with venetoclax and azacitidine. The first chemotherapy was discontinued after 4 days due to an active hemothorax secondary to a recent traumatic rib fracture, which was resolved after surgical management. During the second cycle, venetoclax was discontinued after 1 week because of fever and desaturation associated with a fungal pneumonia. Unfortunately, the patient died 2 months after initiation of therapy.
Discussion
MS is an extramedullary tumor composed of myeloid blasts that characteristically infiltrate and destroy normal tissue architecture. 5 MS was first described by Burns in 1811, and its relationship with AML was later elucidated by Dock.3,6 MS can arise at virtually any anatomical site, including the lymph nodes, 3 but involvement of the nasopharynx is exceptionally rare. All 3 cases of nasopharyngeal MS documented in the English literature presented with local symptoms. In the first 2 cases in 2001 and 2003, the patients presented with symptoms caused by bulky nasopharyngeal masses, such as serous otitis media, nasal bleeding, or nasal obstruction.7,8 In the most recent report, the patient exhibited nasal obstruction accompanied by unilateral pulsatile tinnitus. 9 By contrast, our patient had no nasal or otologic complaints, and the nasopharyngeal lesion was relatively small, resulting in nonspecific clinical signs. Nonetheless, bilateral cervical lymphadenopathy and a recent history of MDS raised suspicion for an underlying hematologic malignancy.
Given the patient’s prior MDS diagnosis and cervical lymphadenopathy, lymph node excision was initially considered; however, due to patient preference, a nasopharyngeal punch biopsy was performed first. In the nasopharyngeal region, malignancies such as nasopharyngeal carcinoma, natural killer (NK)/T-cell lymphoma, Castleman’s disease, and follicular dendritic cell sarcoma are more frequently encountered. Immunohistochemistry analysis in this case showed positivity for MPO, CD33, lysozyme, and CD68, with absence of CD20 and CD3, thereby excluding typical B-cell and T-cell lymphomas and supporting a myeloid origin. 10 Negative EBV in situ hybridization further excluded EBV-driven lymphomas such as extranodal NK/T-cell lymphoma. Positive LCA expression and a high Ki-67 labeling index were consistent with aggressive hematologic malignancies such as AML or MS. 1
A previous study suggests that MS patients without bone marrow involvement may have a more favorable prognosis. 11 The patient was diagnosed with MDS 5 months before his initial otolaryngology evaluation, and peripheral blood smear (PBS) showed rising blasts to over 10% during hematologic follow-up, but the patient declined treatment. At the time of MS diagnosis, repeat PBS confirmed transformation to AML.
Due to its rarity, no standardized treatment guidelines for MS have been established. Nonetheless, current management generally follows AML-based combination chemotherapy protocols.12,13 A recent meta-analysis demonstrated that venetoclax plus azacitidine achieved superior outcomes compared with azacitidine monotherapy in AML. 14 The venetoclax-azacitidine regimen targets a BCL-2-dependent apoptotic pathway independent of the KIT signaling axis. Prior studies reported favorable therapeutic responses with this regimen in MS patients. 14 In the present case, combination chemotherapy was promptly recommended; however, treatment initiation was delayed by 1 week due to patient hesitation. The delay, along with concurrent leukemic transformation, likely contributed to the poorer clinical outcome.
Conclusion
We report a rare case of nasopharyngeal MS presenting without significant local symptoms. MS should be considered as the differential diagnosis of nasopharyngeal mass, particularly in patients with underlying hematologic disorders. Early biopsy and prompt hematologic assessment are essential for accurate diagnosis and may improve treatment outcomes.
Footnotes
Ethical Considerations
This study was approved by the Institutional Review Board of Chonnam National University Hwasun Hospital.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images, in accordance with the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed.