
Abstract

Introduction
A perilymphatic fistula (PLF) is an abnormal communication between the perilymph-filled inner ear and the air-filled middle ear through a defect in the round or oval window membranes. It may cause fluctuating sensorineural hearing loss (SNHL), tinnitus, or vertigo. While traumatic and iatrogenic etiologies are well recognized, spontaneous cases are rare and often overlooked due to nonspecific symptoms.1 -3 Diagnosis remains challenging, as exploratory tympanotomy is invasive and often inconclusive. With advances in magnetic resonance imaging (MRI), delayed contrast-enhanced 3-dimensional fluid-attenuated inversion recovery (3D-FLAIR) sequences have become a valuable noninvasive alternative. The round window sign (RWS)—a focal delayed hyperintensity in the round window niche—has been proposed as a specific imaging marker of perilymph leakage.4 -6 We report a case of bilateral RWS in a patient with recurrent low-frequency SNHL and no vestibular symptoms, suggesting a spontaneous PLF.
Case Presentation
A 47-year-old male presented with recurrent, spontaneously resolving low-frequency hearing loss in both ears. Each episode lasted several days and had no clear trigger. He denied vertigo, tinnitus, aural fullness, head trauma, barotrauma, or ear surgery. Otoscopy was normal. Audiometry demonstrated mild, fluctuating SNHL at 250 to 1000 Hz. Tympanometry showed bilateral type-A curves with preserved acoustic reflexes and otoacoustic emissions. High-resolution computed tomography (HRCT) of the temporal bones excluded structural malformations but revealed soft tissue density in both round window niches (Figure 1A and B). Subsequent 3 T MRI (Magnetom Vida; Siemens Healthineers, Germany) was performed using pre- and delayed post-contrast (4 hours after 0.1 mmol/kg gadolinium) 3D-FLAIR and 3D-constructive interference in steady state sequences. Delayed 3D-FLAIR images showed bilateral, sharply demarcated hyperintensity in the round window niches, consistent with a positive RWS (Figure 2). No enhancement was seen in the oval window or vestibule. Cochlear and vestibular morphology was normal; no endolymphatic hydrops or inner ear malformation was present. Vestibular aqueducts were within normal limits. Because the patient’s symptoms resolved spontaneously and there were no vestibular complaints, conservative management was chosen. He was instructed to avoid Valsalva-inducing activities and maintain voice and physical rest. Oral corticosteroids (prednisone) were prescribed to reduce labyrinthine inflammation and edema. No surgical exploration was performed. At 3- and 6-month follow-up, audiograms showed stable hearing thresholds without further episodes. The final diagnosis was spontaneous bilateral PLF, based on clinical presentation and characteristic MRI findings. Written informed consent was obtained for publication.
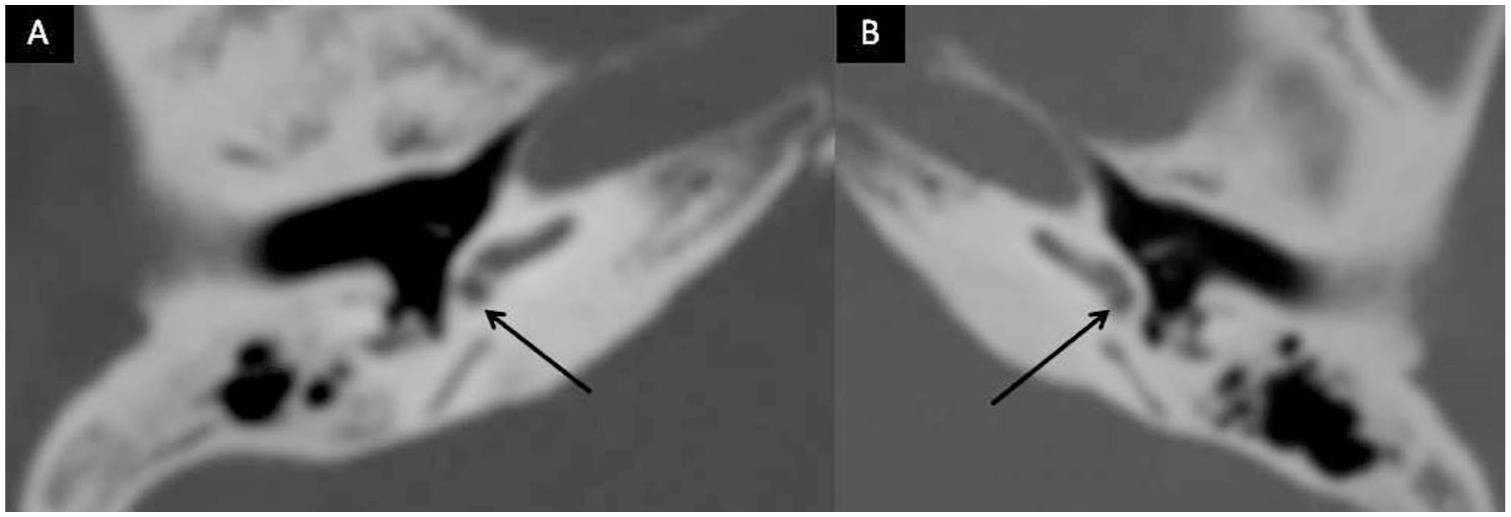
Axial high-resolution computed tomography scans of the temporal bones (A, B) show bilateral round window niches (black arrows) filled with dense soft tissue. This finding is consistent with the round window sign suggestive of a perilymphatic fistula. The adjacent middle ear and ear capsule structures appear to be preserved.
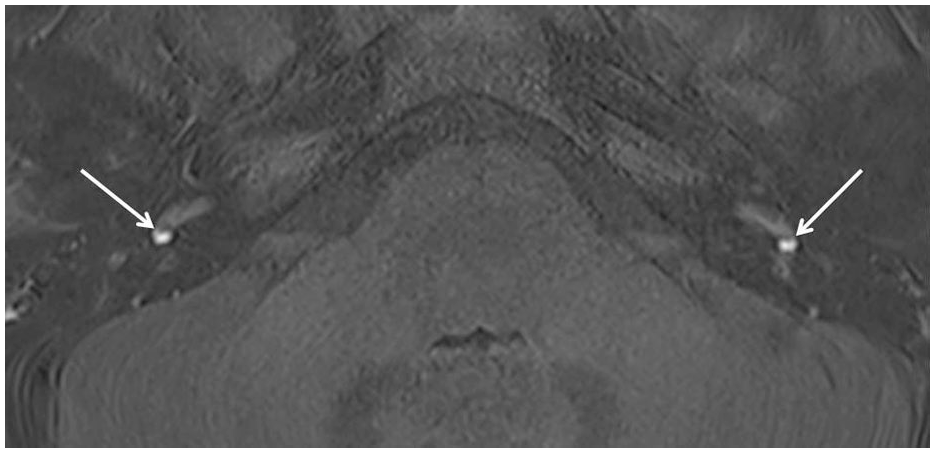
Axial 3D-FLAIR MR image acquired 4 hours after gadolinium injection shows bilateral, sharply demarcated hyperintense foci in the niches of the round windows (white arrows). These signal intensities represent the round window sign and indicate the presence of perilymphatic leakage. 3D-FLAIR, 3-dimensional fluid-attenuated inversion recovery; MR, magnetic resonance.
Conclusion
Spontaneous PLF is an uncommon but important cause of fluctuating SNHL. The absence of trauma or vestibular symptoms can lead to misdiagnosis as Menière’s disease or idiopathic sudden SNHL. Imaging has therefore become central to diagnosis. Among MRI techniques, delayed contrast-enhanced 3D-FLAIR is highly sensitive to low gadolinium concentrations within the perilymph. Delayed imaging (3-4 hours after injection) enhances contrast between perilymphatic spaces and surrounding tissues, enabling subtle detection of leakage at the round window. Dubrulle et al 1 first described the RWS as a reliable indicator of PLF, showing strong correlation with surgically confirmed cases. Subsequent studies confirmed its diagnostic value and suggested that it may replace exploratory tympanotomy in selected patients.4 -6 In our patient, the bilateral RWS and absence of other pathological findings support the diagnosis of idiopathic bilateral PLF, a presentation rarely documented in the literature. Conservative management was effective, consistent with reports that some spontaneous fistulas close under pressure-stabilizing precautions. The combination of HRCT and delayed 3D-FLAIR MRI allowed a confident diagnosis while avoiding unnecessary surgery.
Delayed contrast-enhanced 3D-FLAIR MRI is a sensitive and noninvasive imaging method for detecting perilymphatic leakage. The RWS provides a clear diagnostic clue for PLF, particularly in patients with isolated hearing symptoms and no history of trauma. Early recognition of this finding can guide conservative treatment, prevent unnecessary surgical intervention, and improve outcomes. Larger studies are warranted to validate the diagnostic accuracy of RWS and incorporate it into standardized otologic imaging protocols.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Informed written consent was obtained from the patient for their anonymized information to be published in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.