
Abstract
Introduction:
Primary tracheal tumors are rare, with an estimated incidence of 1/million individuals. Tracheal schwannomas are exceptionally uncommon, and no consensus exists regarding optimal management. Reported treatment options include open surgical resection (OSR) and endoscopic (ES) approaches.
Objective:
To provide a narrative synthesis of reported cases of tracheal schwannoma, summarizing patient demographics, tumor characteristics, management strategies, outcomes, and recurrence.
Materials and Methods:
A narrative review was conducted through a comprehensive literature search across PubMed, Google Scholar, EMBASE, Scopus, Web of Knowledge, and Ovid. Data on baseline characteristics and outcomes were extracted from eligible studies. Findings were summarized descriptively using counts, percentages, means, and ranges. No inferential statistical analyses or meta-analytic synthesis were performed.
Results:
Forty-two studies reporting 48 patients were included. Twenty-seven patients underwent ES management, and 21 underwent OSR. Patients reported in the ES group were generally older, while sex distribution appeared broadly similar across the 2 treatment approaches. ES cases often involved smaller, intraluminal tumors, whereas open resection was more frequently applied to larger or extratracheal lesions. Across both approaches, over 90% of patients experienced symptom resolution, and recurrence was rarely reported. Follow-up durations varied widely, with many studies lacking long-term data.
Conclusions:
Both ES and OSR have been reported as effective treatment options for primary tracheal schwannoma. The choice of approach should be individualized based on tumor size, morphology, extension, and patient comorbidity. Given the narrative design and reliance on case reports and small series, these findings should be interpreted with caution, and further studies are needed to establish standardized management strategies.
Introduction
Primary tracheal schwannomas are exceedingly rare, accounting for <0.5% of all tracheal tumors.1,2 Because of their rarity, most knowledge comes from isolated case reports and small case series, and there is no consensus on optimal management.3,4 Treatment approaches vary from minimally invasive endoscopic (ES) procedures to open surgical resection (OSR),3,5-7 but guidance on patient selection and expected outcomes remains limited.3,4
Symptoms may be absent in early disease because the airway can tolerate up to 50% narrowing before clinical manifestations appear. It is typically only when the tumor exceeds 50% of the tracheal space that patients can begin to present nonspecific symptoms such as shortness of breath, dry cough, or, in more severe cases, difficulty breathing during inhalation. 8 The tissue’s definitive diagnosis of schwannoma is made by immuno-histochemical analysis, as the confirmation of the diagnosis of schwannoma is demonstrated by the presence of diffuse positivity for S-100 protein and vimentin. 9
There is no consensus on the optimal management of tracheal schwannomas due to the rarity of these tumors. Common treatment options include surgery and interventional bronchoscopic therapy. 1
Given the rarity of this entity and the lack of standardized treatment guidelines, a structured synthesis of the literature is important to inform clinical decision-making, highlight knowledge gaps, and guide future research. This review aims to provide a narrative overview of reported cases of tracheal schwannoma, focusing on patient demographics, tumor characteristics, management strategies, outcomes, and recurrence.
Materials and Methods
Data Collection Procedures and Tools
Access to the full-text manuscript of the studies selected needed permission, which was solved by university electronic library membership and/or individual valid access to specific journal sites.
This review was conducted following the Scale for the Assessment of Narrative Review Articles guidelines for narrative reviews. 10 The importance of the topic was justified by the rarity of tracheal schwannomas and the absence of consensus regarding optimal management. The aim was to provide a structured overview of published experiences with ES and OSR of tracheal schwannomas.
Literature Search
A comprehensive search was performed using PubMed, Google Scholar, EMBASE, Scopus, Web of Knowledge, and Ovid. The search terms included “tracheal schwannoma,” “primary tracheal tumor,” “bronchotracheal schwannoma,” and “endoscopic resection.” The search was limited to English-language publications from 1950 to 2025. References from relevant articles were also manually screened to identify additional eligible studies.
Eligibility Criteria
Eligible studies included case reports, case series, and clinical studies reporting the management of primary tracheal schwannoma with either ES or OSR approaches. Articles without patient-level data or outcome information were excluded. Cadaver or animal studies, expert opinion pieces, and reports with unclear or incomplete descriptions were also excluded.
Study Selection and Data Extraction
After removing duplicates, titles and abstracts were screened to identify potentially relevant studies. Full-text review was performed to confirm eligibility. Data were independently extracted, including patient demographics, tumor characteristics, surgical approach, functional outcomes, follow-up duration, and recurrence.
Data Synthesis
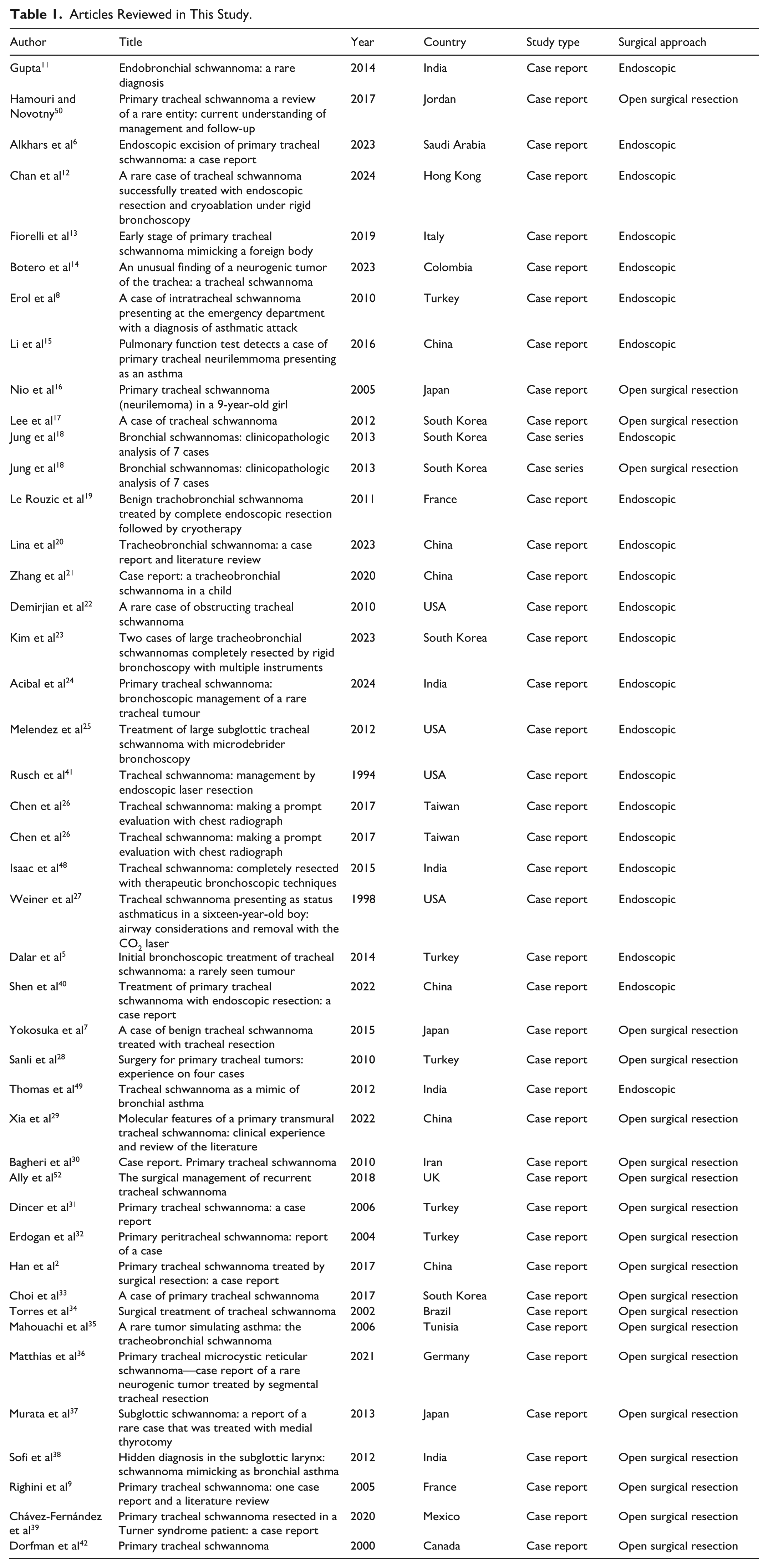
Findings were summarized descriptively using counts, percentages, means, ranges, and standard deviations where available. No formal statistical comparisons, heterogeneity assessments, or meta-analytic synthesis were performed due to the rarity of the disease, small sample sizes, and heterogeneity across studies. The author independently extracted data from each study and assessed the outcome and the reporting of the variable outcome data. These studies revealed that both management strategies (ES and OSR) showed an excellent outcome. The articles reviewed in the present study are presented in Table 1.
Articles Reviewed in This Study.
Types of Outcome Measures
Reported outcomes included symptom resolution, airway patency, surgical success, recurrence, and follow-up duration, as described in the included studies.
In this narrative review, no formal meta-analytic synthesis, heterogeneity assessment, or subgroup analyses were performed; therefore, the findings should be interpreted with caution, given the small number of available studies and the descriptive nature of the review.
Statistical Analysis
Data extracted from the included studies were summarized descriptively. Counts, percentages, ranges, and means with standard deviations were reported where possible. Given the heterogeneity and small number of cases, no formal statistical comparisons or meta-analytic synthesis were performed.
Results
Study Selection and Characteristics
A total of 42 studies reporting 48 patients with tracheal schwannoma were included. Twenty-seven patients underwent ES group treatment, while 21 underwent OSR group. The reviewed articles and their characteristics are summarized in Table 1.
Demographics
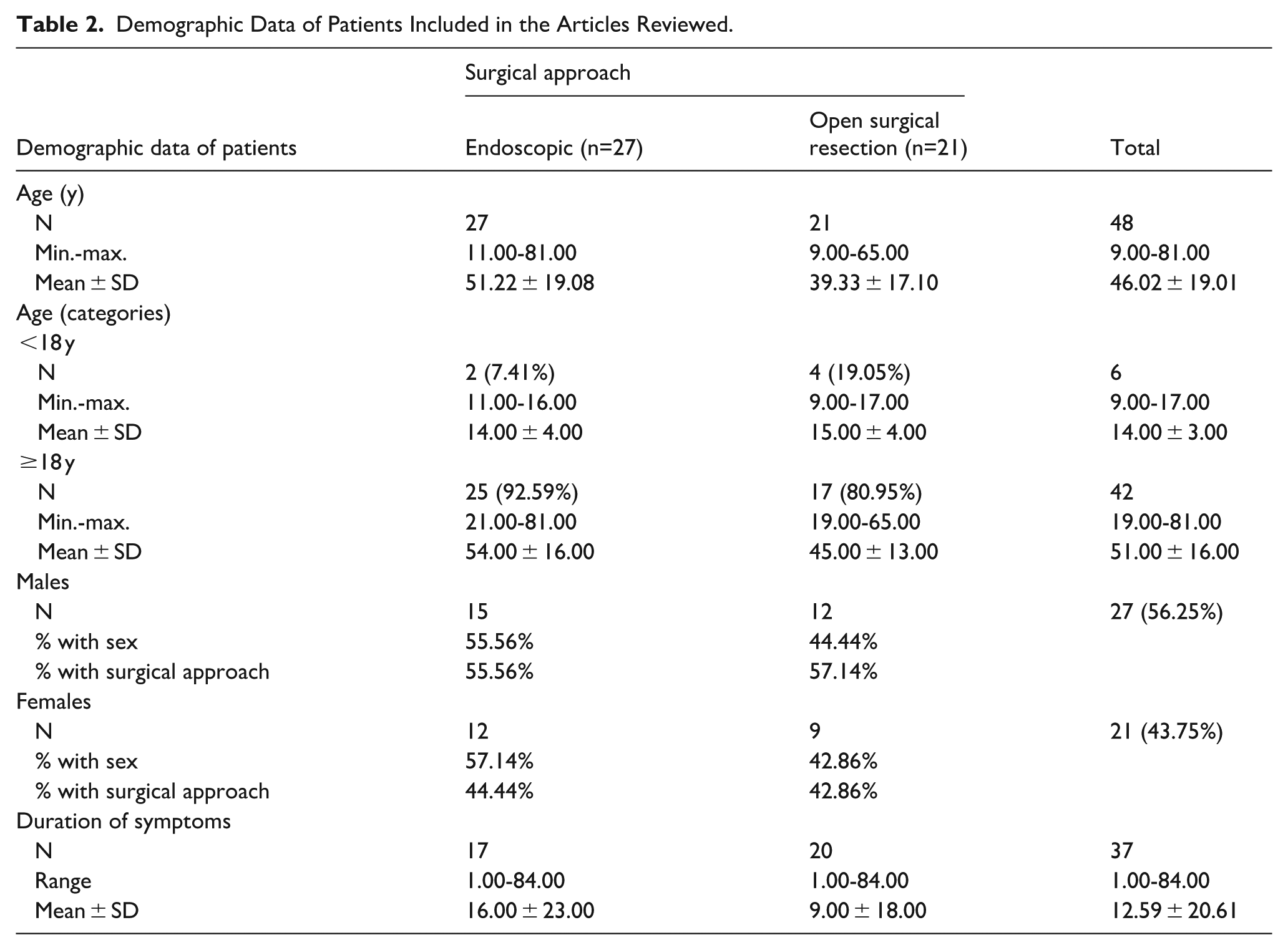
Patients managed endoscopically tended to be older (mean age ~51 years, range 11-81 years) compared with those undergoing open resection (mean age ~39 years, range 9-65 years). The majority of patients in both groups were adults (≥18 years). Sex distribution was similar, with a slight predominance of males overall (56%). Duration of symptoms before diagnosis varied widely, ranging from 1 to 96 months, with mean durations of ~22 months in the ES group and 19 months in the OSR group (Table 2).
Demographic Data of Patients Included in the Articles Reviewed.
Tumor Location and Characteristics
In the ES group, tumors were distributed across multiple tracheal levels, including proximal, carina, intermediate, distal trachea, and both main bronchi. In the OSR group, tumors were more commonly located in the upper and lower segments of the trachea. The maximum diameter of tumors ranged from 2 to 40 mm. Mean tumor size was slightly larger in the OSR group (~23 mm) compared to the ES group (~19 mm). Distances to the carina and vocal cords, when reported, showed wide variability across cases (Table 3).
Tumor Location and Characteristics in the Studied Articles Reviewed.
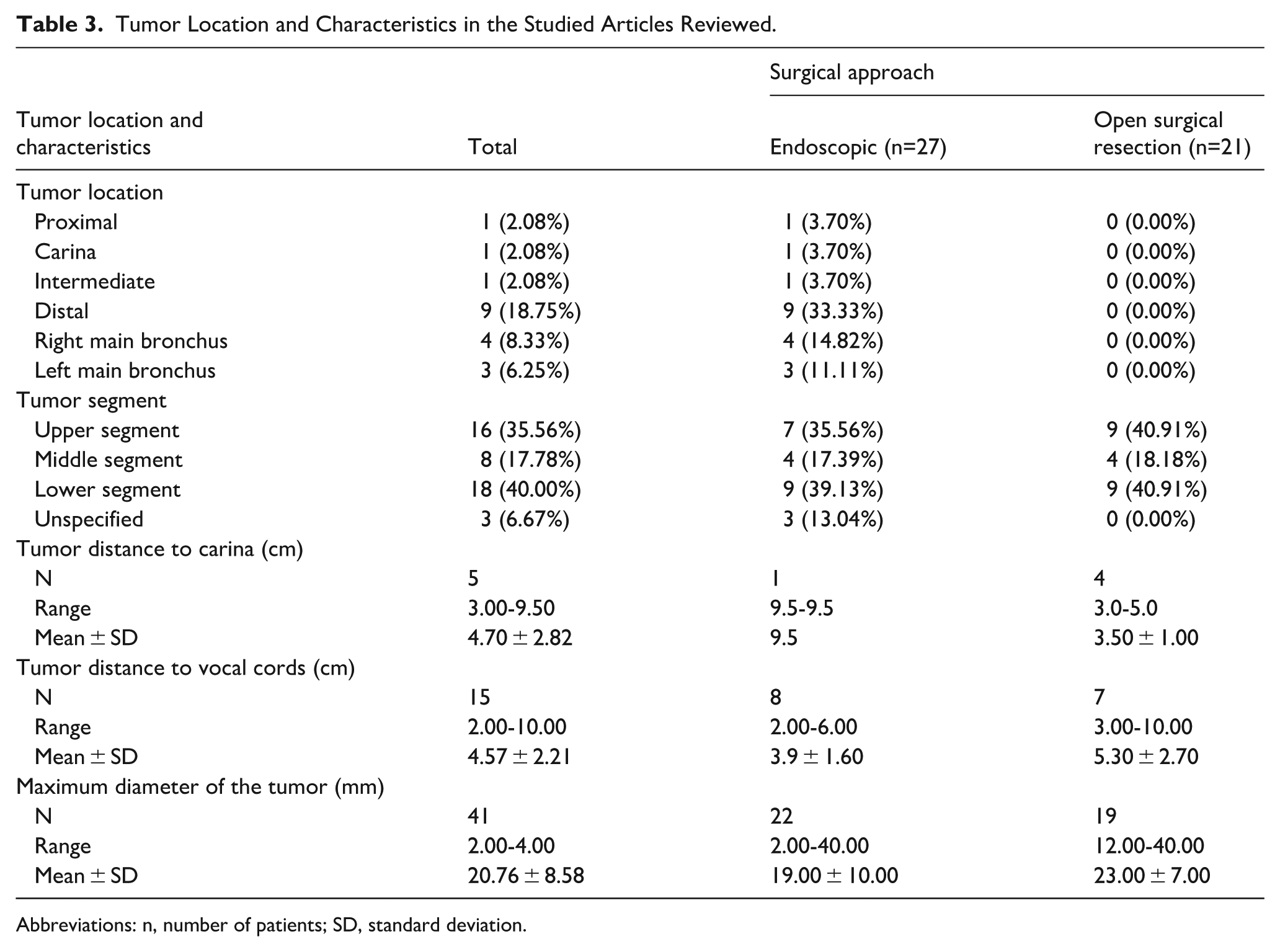
Abbreviations: n, number of patients; SD, standard deviation.
Follow-Up
Follow-up duration ranged from 1 to 96 months, with an overall mean of ~21 months across studies. Approximately 29% of cases did not specify follow-up length, and 6% had short-term follow-up only. ES cases generally reported follow-up up to 66 months, while OSR cases were reported up to 96 months (Table 4).
Reported Follow-Up in the Studied Articles Included.
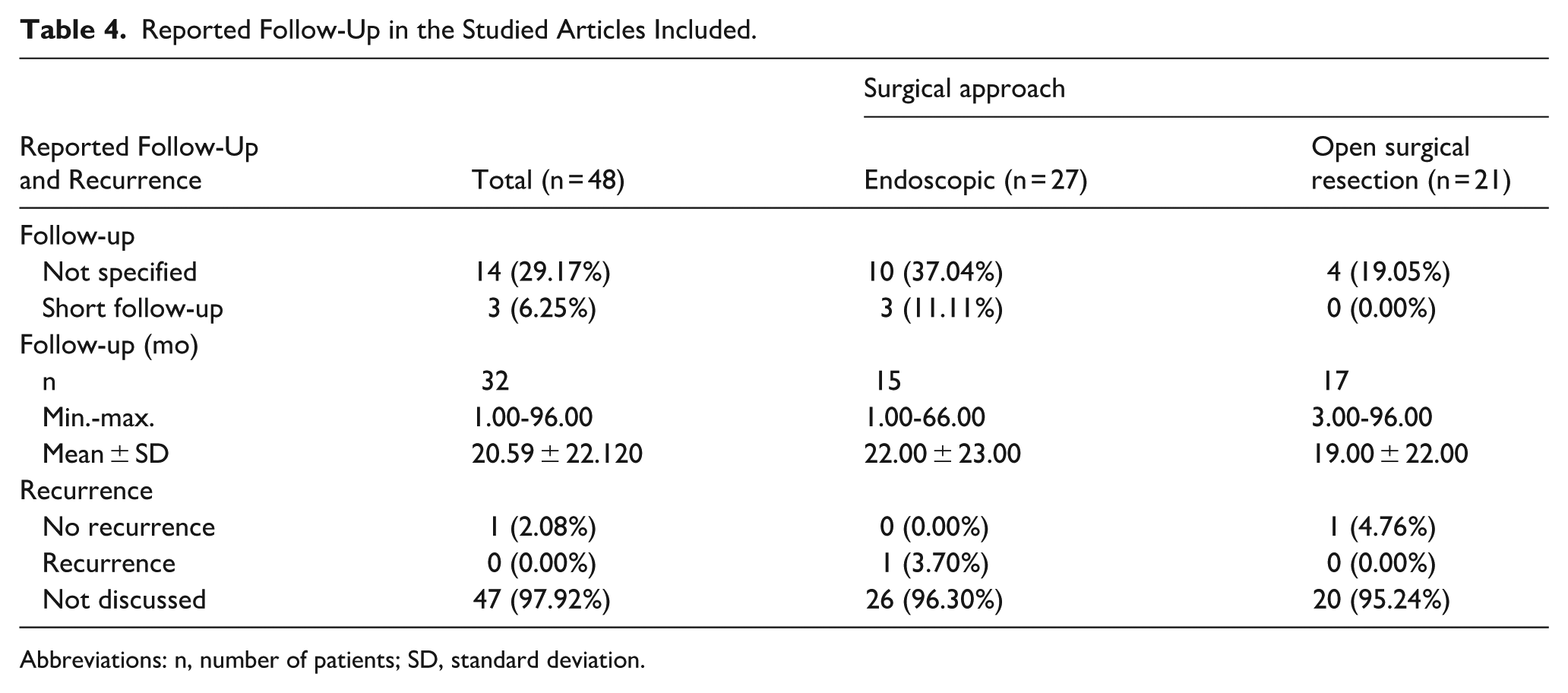
Abbreviations: n, number of patients; SD, standard deviation.
Functional Outcomes
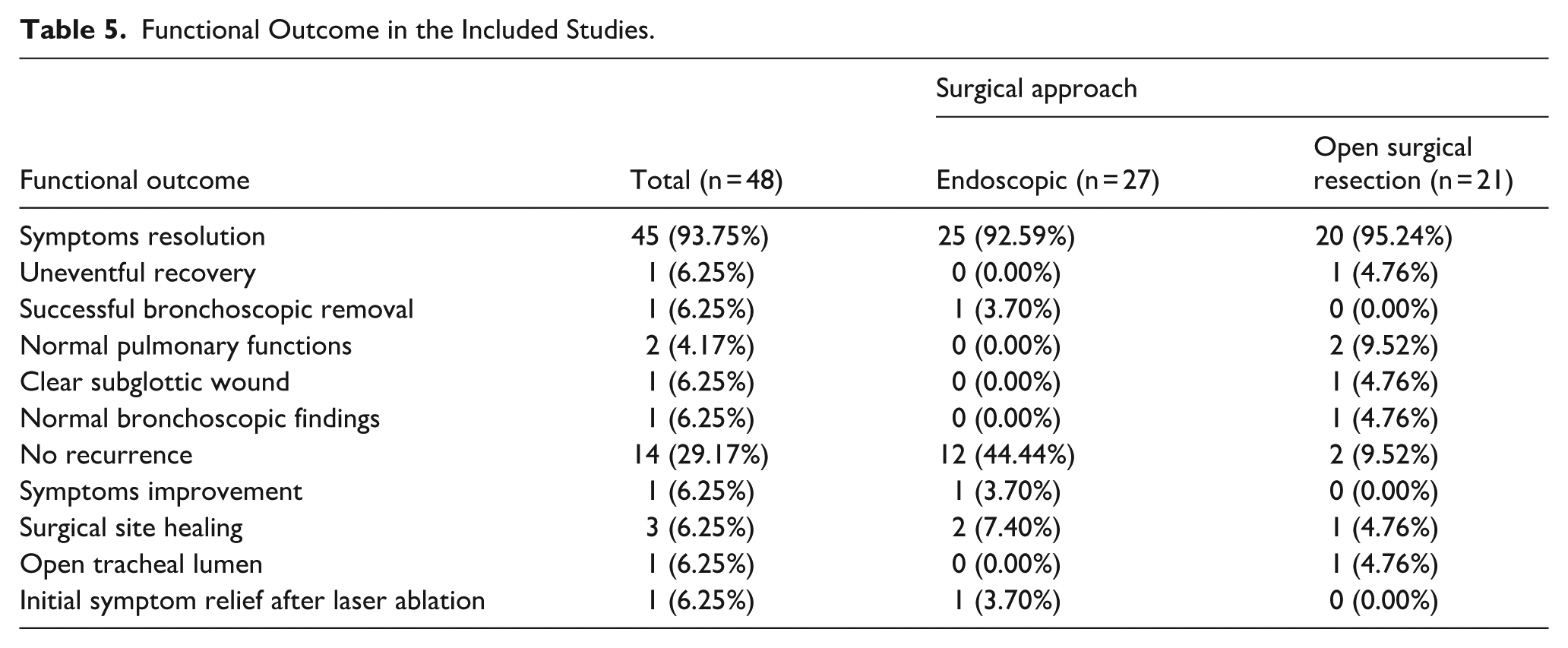
Symptom resolution was reported in the vast majority of cases (over 90%) in both groups. ES cases often documented improvement in airway patency, healing at the surgical site, and absence of recurrence during the available follow-up period. OSR cases similarly demonstrated high rates of symptom relief, with occasional documentation of normal pulmonary function and clear bronchoscopic findings. Recurrence was rarely reported, although follow-up was limited in many studies. A variety of adjuvant ES therapies were described, including cryotherapy, diode laser coagulation, and argon plasma coagulation, each used in isolated cases. Reported complications were minimal and generally self-limited (Table 5).
Functional Outcome in the Included Studies.
Procedures
In the OSR group, surgical techniques included segmental tracheal resections with anastomosis, wedge resections, circumferential resections with reconstruction, posterolateral thoracotomy, and anterior cervical approaches. Some procedures involved partial cricoid or cartilage resection with flap reconstruction. In the ES group, reported techniques included rigid bronchoscopy, Nd:YAG laser, electrocautery snaring, argon plasma coagulation, cryotherapy, and microdebrider bronchoscopy, among others.
Discussion
Published reports suggest that the management of primary tracheal schwannoma is influenced by patient condition, tumor size, morphology, and the presence of extratracheal extension.3,4 Across the literature, ES treatment has most often been described in small (<2 cm), pedunculated, intraluminal tumors, particularly in patients with limited cardiopulmonary reserve.3,5,40,41 These cases generally reported favorable outcomes when complete excision with safe margins could be achieved.5,40,41
Conversely, OSR has more frequently been applied in tumors with a broad base or extratracheal extension, where ES techniques were considered insufficient to ensure complete removal.3,7,42,43 Surgical resection was commonly associated with durable outcomes, although these procedures are more invasive and carry greater perioperative risk.44-47 Despite this, open surgery has historically been the definitive approach for airway tumors, and several series emphasize its role in ensuring radical resection and long-term disease control.42,44-47
ES techniques reported in the literature include rigid bronchoscopy, Nd:YAG and CO2 laser, electrocautery snaring, argon plasma coagulation, cryotherapy, and microdebrider bronchoscopy.40,41,48,49 The appeal of these methods lies in their minimally invasive nature, shorter hospital stays, and the ability to preserve airway anatomy. However, concerns remain regarding incomplete resection, especially in sessile or transmural lesions, where tumor recurrence has been documented.41,50-52 Some authors have suggested that adjuvant therapies such as cryotherapy or Argon Plasma coagulation (APC) at the resection base may help reduce recurrence risk, though evidence is limited to isolated reports.40,41
Follow-up data across studies are heterogeneous, ranging from a few months to more than 8 years.9,50 In nearly one-third of cases, follow-up was not specified, which complicates interpretation of long-term outcomes. Reported recurrences after ES treatment highlight the need for careful surveillance, including repeat bronchoscopy and imaging. In contrast, recurrence after OSR was rarely documented, though the numbers remain too small to draw definitive conclusions. These observations suggest that while ES resection may provide symptom relief and disease control in selected patients, it should be accompanied by structured, long-term follow-up protocols.41,50-52
Overall, both ES and OSR have been reported as effective approaches for tracheal schwannoma.3,5,7,40 The choice of strategy appears to depend largely on tumor characteristics and patient comorbidity rather than a universally superior technique. Importantly, most available evidence is derived from case reports and small series, which limits the generalizability of findings. This underscores the rarity of the disease and the absence of standardized management algorithms. Future research should focus on establishing multi-institutional registries, applying uniform reporting standards, and comparing outcomes prospectively to better define the role of different treatment modalities.
Limitations
This review has several limitations. First, tracheal schwannomas are exceedingly rare, and the available literature is limited almost entirely to case reports and small case series. As such, the strength of the conclusions is inherently restricted by small sample sizes and heterogeneity across reports. Second, although data were summarized descriptively, no formal risk of bias assessment, certainty-of-evidence grading, or meta-analytic synthesis was performed. Therefore, observed differences between ES and OSR approaches should be regarded as descriptive trends rather than statistically validated findings. Third, many studies lacked long-term follow-up, making it difficult to assess recurrence rates and the durability of treatment outcomes fully. Finally, reporting standards varied widely, with incomplete information on patient demographics, tumor characteristics, and follow-up in several studies.
Despite these limitations, the review provides a consolidated overview of published experiences and highlights patterns that may guide clinical decision-making. Further prospective studies and larger pooled analyses are needed to establish evidence-based management strategies for this rare tumor.
Conclusion
Primary tracheal schwannomas are exceedingly rare, and the evidence base is limited to case reports and small series. Both ES and OSR have been reported as effective approaches, with the choice of management depending largely on tumor characteristics and patient comorbidity. ES procedures offer less invasive alternatives and preserve airway anatomy but require careful surveillance because of the risk of recurrence. OSR, while more invasive, has been associated with durable outcomes and low recurrence rates.
Given the limited number of reported cases and the absence of standardized guidelines, these findings should be interpreted with caution. Future progress will require collaborative, multi-institutional efforts with standardized reporting of patient characteristics, treatment strategies, and long-term outcomes. Until such data are available, management decisions should remain individualized and guided by multidisciplinary discussion.
Recommendations
Both ES and OSR have been reported as effective strategies for the management of primary tracheal schwannoma. ES approaches provide the benefit of being minimally invasive and preserving airway anatomy, though concerns remain regarding the completeness of resection and the potential for recurrence, particularly in sessile or transmural tumors. OSR, on the other hand, is associated with durable outcomes but carries higher operative risk and morbidity.
Given these considerations, long-term follow-up should be emphasized in all patients, as recurrence may occur years after the initial treatment. Surveillance strategies often include repeat bronchoscopy and imaging, although there is no standardized protocol for the frequency or duration of follow-up.
Future progress will likely depend on collaborative efforts, including the development of multi-institutional registries and standardized reporting of patient characteristics, operative details, and outcomes. Such initiatives could eventually support consensus guidelines and evidence-based recommendations for optimal management and surveillance.
Until more robust data are available, management decisions should remain individualized, with careful consideration of tumor morphology, size, extension, and patient comorbidities. Multidisciplinary discussion involving thoracic surgeons, interventional pulmonologists, and anesthesiologists is encouraged to optimize treatment planning in complex cases.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.