
Abstract
Glomangiopericytoma is an uncommon tumor of the sinonasal region, originating from the pericytes that envelop capillaries, and it accounts for fewer than half a percent (0.5%) of all sinonasal tumors. This report presents the case of a 65-year-old man who experienced worsening nasal obstruction and was subsequently diagnosed with glomangiopericytoma based on histological, immunohistochemical, and radiographic findings. The patient underwent a complete excision of the tumor via an endoscopic endonasal approach. Upon follow-up after the surgical resection, the patient exhibited no signs of recurrence.
Introduction
Glomangiopericytoma is a rare type of tumor that originates from the pericytes in the sinonasal area. It accounts for less than half a percent (0.5%) of sinonasal tumors and is characterized by a prominent perivascular growth pattern with a considerably-low-malignant potential. It is also called sinonasal type hemangiopericytoma and is so called because the lesion falls between glomus tumors and capillary hemangioma. 1 The term glomangiopericytoma was introduced by Granter et al in 1998 to describe a tumor that exhibits the composite features of hemangiopericytomas. In 2005, glomangiopericytoma (GPC) was categorized by the World Health Organization as a soft tissue tumor of the nose and paranasal sinuses, characterized by borderline malignancy and a low potential for malignancy, with an overall survival rate that is considered excellent. The underlying cause of GPC is often unclear, but it may be linked to factors such as previous trauma, hypertension, pregnancy, or a history of steroid use. GPCs are frequently mistaken for other spindle cell and vascular neoplasms in the sinonasal tract, with solitary fibrous tumors being the most common misdiagnosis. This case report details an elderly male that had GPC originating from the right nasal cavity. The patient underwent successful treatment through an endoscopic endonasal resection.
Case Report
A 65-year-old male patient presented to the otorhinolaryngology, head and neck surgery outpatient clinic with a complaint of right-sided nasal obstruction. He reported a decreased quality of life due to the worsening obstruction, which had been gradually increasing in severity over the past few months.
Upon further questioning, the patient denied experiencing any other nasal symptoms and reported no history of nasal trauma, previous surgeries, or illicit drug use. Additionally, there was no family history of sinonasal tumors. His medical history included well-controlled hypertension and hyperlipidemia, for which he was on medication.
During the nasal endoscopic examination, a right-sided nasal mass was observed. The mass appeared dark red in color and extended to the posterior aspect of the inferior meatus, partially occupying the choanae without invading the inferior turbinate. The lesion was noted to be soft in consistency. Figure 1 represents the nasal mass during endoscopic examination of the right-side nasal cavity (Figure 2). Figure 3 demonstrates the histopathological examination of the nasal mass. Histology and immunohistochemistry are critical for understanding the behavior of this unusual tumor.
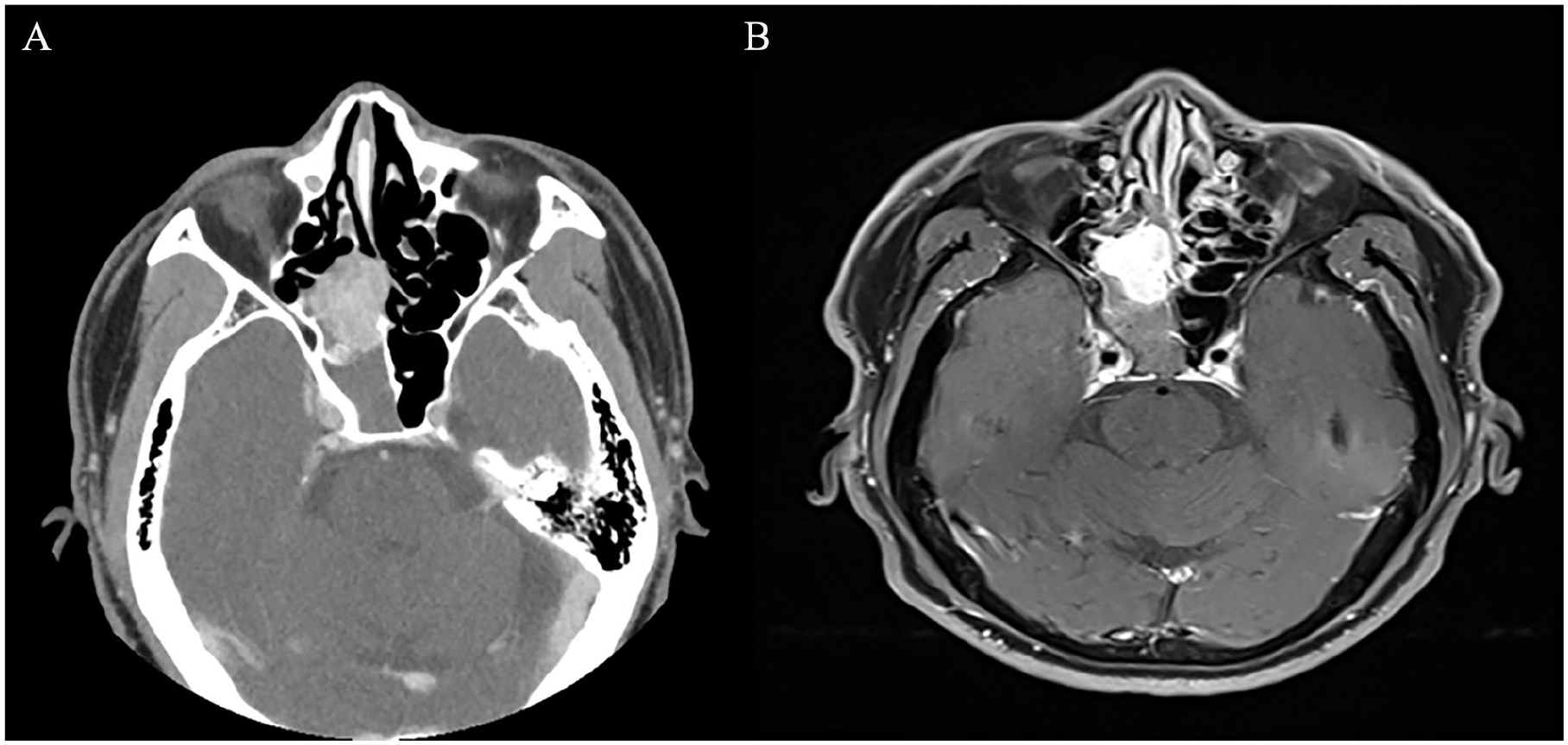
Nasal mass in the endoscopic examination of the right side of the nasal cavity. (A) CT paranasal sinuses showing right sided enhanced nasal mass. (B) T1-weighted MRI images show a homogeneously-enhancing soft tissue mass at the right ethmoid area, intraoperatively it was found to be originated from the posterior aspect of the nasal septum.
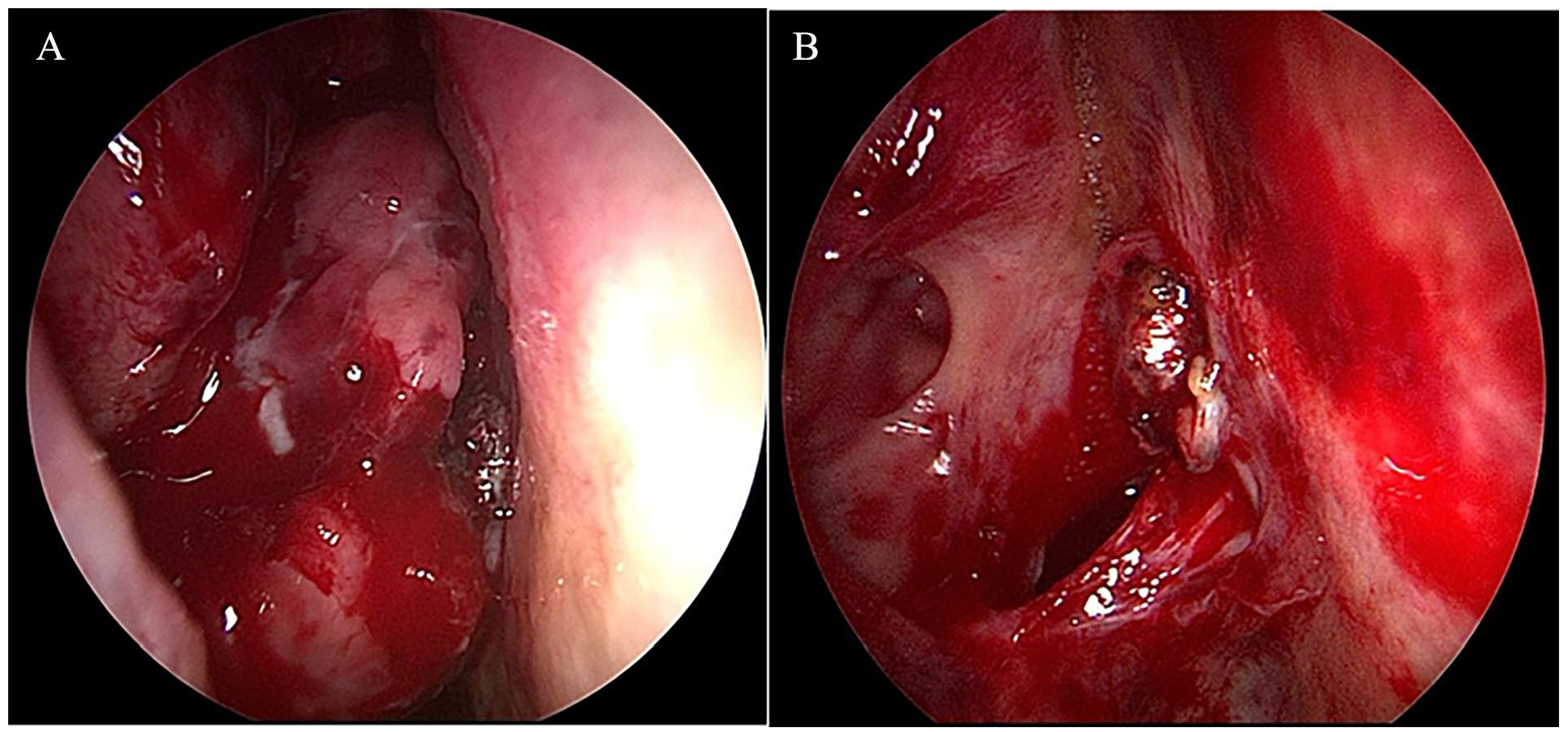
(A) Endoscopic examination of the right-sided nasal cavity with findings of mass located between right middle turbinate lateraly, spetum medially, and right inferior turbinate inferiorly. (B) Endoscopic view after a complete resection of the mass achieved.
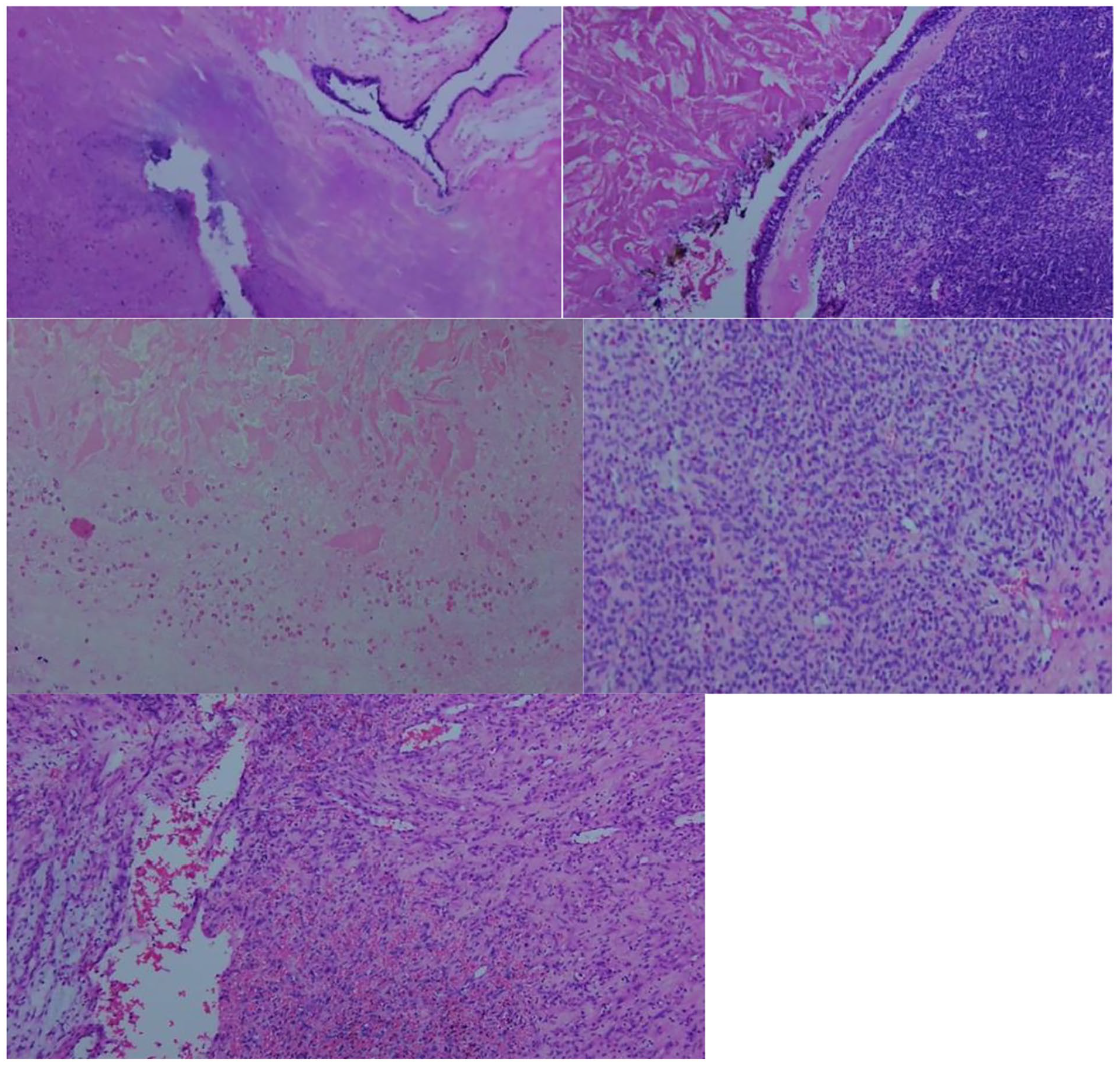
Histopathological examinations of the nasal mass. Photomicrographs of the tumor specimen. Revealed numerous thin-walled, branching staghorn vessels surrounded by oval- to spindle-shaped cells. positive cyclin D1 and B-catenin.
On complete physical examination, the left-sided nasal cavity, the ears, the throat, the head, the neck, and cranial nerves were found to be unremarkable. The patient underwent a comprehensive radiological evaluation, which included both computed tomography (CT) and magnetic resonance imaging (MRI) scans with contrast enhancement. The CT scan revealed a well-defined, contrast-enhancing mass situated within the right nasal cavity. Following a thorough preoperative assessment, the patient was scheduled for surgical excision of the tumor using an endoscopic endonasal approach.
During the surgery, it was observed that the mass was located at the posterior aspect of the nasal septum. The tumor extended medially, reaching the superior and middle turbinates, also to the inferior meatus. The mass occupied the right choanae with no contact to the inferior turbinates.
The mass was carefully debulked initially to determine the anatomical landmarks, then followed by complete resection with consideration of safe margins. The surgery was conducted smoothly with no intraoperative issues, as well as no postoperative sequelae or complications. The patient was discharged with a good status. The final histopathological examination showed the following: spindle cell tumor, with the presence of mitoses, cellularity, with no necrosis or abscess, and the presence of staghorn-like vessel. Immunohistochemistry showed the following: positive cyclin D1 and B-catenin. Upon follow-up in the clinic, patient reported an excellent improvement in the right-sided nasal obstruction and endoscopic examination showed no evidence of recurrence.
Discussion
Hemangiopericytoma was first described by Stout and Murray 2 as a soft tissue tumor marked by vascular proliferation, including branching vessels and perivascular hyalinization, despite its considerable morphological variability. In 1976, Compagno and Hyams 3 further refined this classification by identifying lesions within the nasal cavity as intranasal hemangiopericytoma tumors.
Over time, these tumors have come to be recognized as a distinct entity within the spectrum of sinonasal tumors, now commonly referred to as GPC. This terminology distinguishes them from the classic soft-tissue hemangiopericytoma, which represents a separate pathological condition. GPC is now understood to be a unique tumor type within the sinonasal tract, characterized by its specific histological features and clinical behavior. GPC is considered a rare sinonasal tumor. The gross presentation of these kinds of lesions is generally insufficient. It can be firm, soft, fleshy, and/or friable, or it can have hemorrhaging and/or fluid-filled patches. The average size of a sinonasal lesion is usually around 3.1 cm. 3
The age of patients in the literature ranges from the second decade of life to 86 years. The majority of cases documented in the literature indicate that it is a female-predominant condition. 4 In line with this, we present the case of a 65-year-old male patient who experienced nasal obstruction on the right side. Most commonly, patients report symptoms such as nosebleeds, which occur in 78% of cases. This is often followed by nasal obstruction, reported in 52% of cases, and headaches, which are seen in 17% of patients. Other symptoms may also be present but are less common. These tumors form in the nasal epithelium of the nasal cavity. The symptomatology of advanced-stage tumors may differ, and the patient may appear with vision abnormalities, chronic sinus disease, or cheek paresthesia. 5 In our case, the patient presented with the right-sided nasal obstruction.
Previous trauma, high blood pressure, extended use of corticosteroids, being pregnant, and hormonal imbalances are all risk factors that may play a role in the etiology. 6 In our patient, no such risk factors were identified. CT and MRI were both utilized to assess the tumor’s characteristics and evaluate its effect on the surrounding structures. These imaging techniques provided detailed insights into the tumor’s size, location, and potential impact on adjacent tissues and organs, allowing for a comprehensive understanding of its nature and the extent of its involvement. Patients are usually assessed endoscopically first due to their symptoms. CT and MRI allow for an additional precise evaluation of tumor features and extension. CT scans typically reveal a soft-tissue tumor with significant enhancement following contrast injection. For larger tumors, angiography is often performed to thoroughly assess the tumor’s blood supply. This imaging technique helps in mapping out the vascular network feeding the tumor and also facilitates preoperative embolization, a procedure that can reduce blood flow to the tumor, minimizing potential bleeding during surgery and aiding in a safer and more controlled surgical removal. In our case, the decision was not to do preoperative embolization, since the lesion originating from medial aspect of nasal cavity. The vascular supply to the GPC is best visualized via digital subtraction angiography, which is then utilized to plan a preoperative embolization. Transarterial embolization is used to prevent significant surgical bleeding. 7
Histological examination is important in diagnosing GPC. Hematoxylin and eosin staining is typically used to evaluate the tumor, revealing a well-delineated, yet unencapsulated, subepithelial mass. This mass is situated beneath the normal respiratory epithelium and is distinguished by a widespread proliferation of densely-packed cells, which are typically organized in short, bundled arrangements known as fascicles. In some instances, the tumor may exhibit additional structural patterns, including storiform (swirled), whorled (spiral-like), or palisaded (fence-like) formations. These cell arrangements are interspersed with numerous thin-walled blood vessels that often take on a characteristic staghorn shape, contributing to the tumor’s unique histological appearance.
The neoplastic cells within GPC are relatively uniform in size and shape, typically ranging from oval to spindle-shaped. These histological features are key to differentiating GPC from other similar neoplasms. In our case, the diagnosis of GPC was confirmed through meticulous histopathological examination, which identified these characteristic features.
The limited number of recorded cases of GPC, makes it challenging to understand the treatment and prognosis of these lesions and hence is based on the existing literature about GPCs. The sinonasal form of hemiangiopericytoma is thought to comprise a wide range of neoplasms, including GPCs. The gold standard for treatment is usually recognized to be surgical resection with tumor-free margins. The treatment of choice is unquestionably-wide field total excision. Endoscopic surgery is preferable over external surgery since it provides greater benefits. The overview is improved, and the tumor entry and extension may be assessed more precisely. Furthermore, blood loss is avoided, the risk of causing damage to the lacrimal tissues is reduced, and the normal physiology of the nose is preserved. Septal deviation, highly-vascular tumors, and orbital extension are all factors that may exclude endoscopic surgery. 8 Radiotherapy plus chemotherapy may be indicated in cases with an unresectable primary tumor or metastatic disease. In addition, to treat local diseases, adjuvant radiation may be utilized in conjunction with surgery. 9
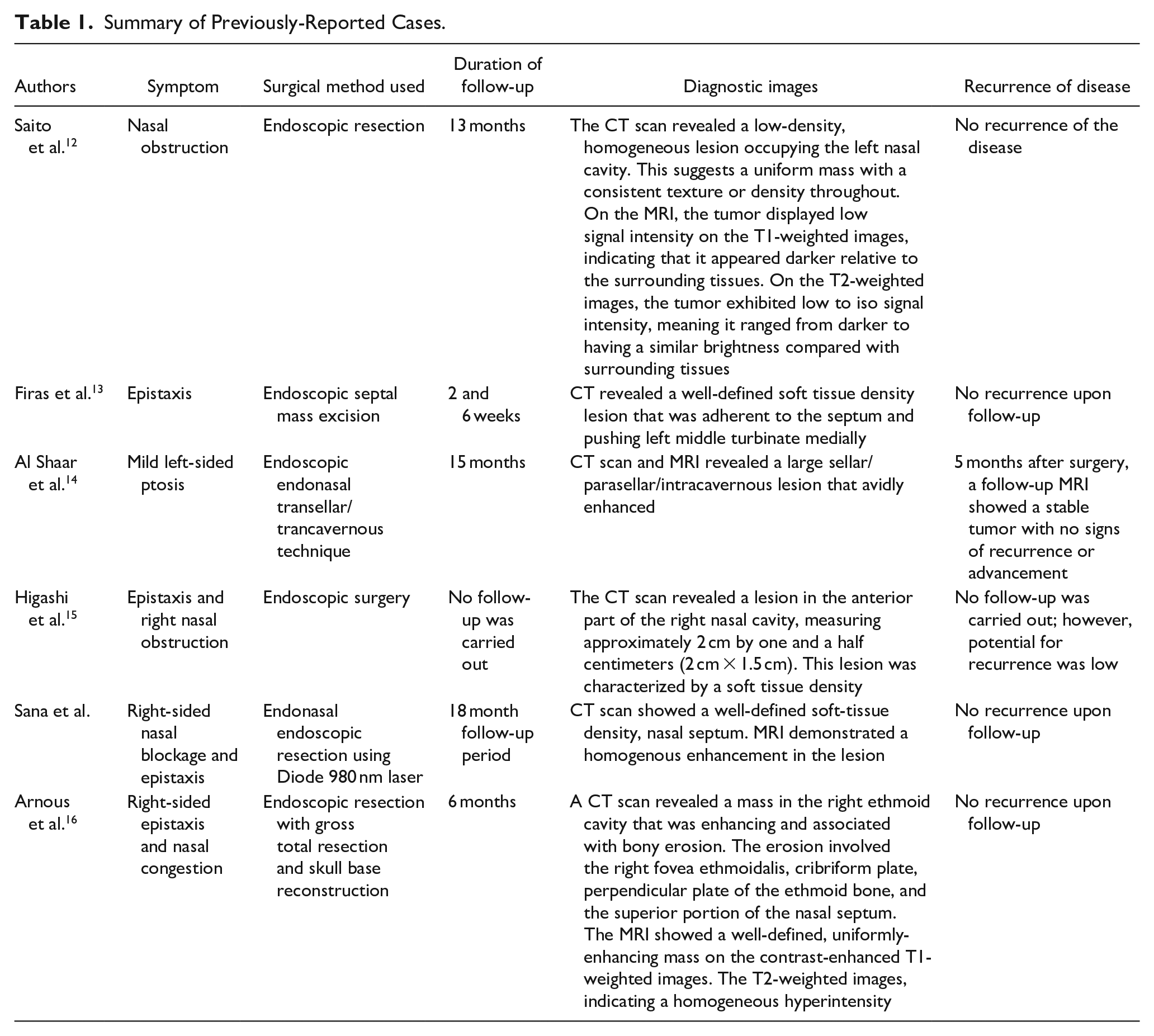
Endoscopic resection is not ruled out when the tumor is highly vascular, as long as preoperative embolization is attempted. The advantages of this approach include less intraoperative bleeding and greater visualization of the tumor. By lowering the circulatory blood supply to the tumor, preoperative embolization of afferent vessels can aid in surgical excision. Several authors have advocated for preoperative angioembolisation in the presence of large, extensive, and vascular tumors. 10 Endoscopic nasal resection enabled us to completely remove the tumor. 11 Table 1 summarizes the previous findings on the symptoms of patients, method of surgical treatment, duration of their follow-up, diagnostic images they used, and recurrence of disease.
Summary of Previously-Reported Cases.
Patients with GPC generally have a favorable prognosis, with a high overall survival rate, and metastasis is rare. The recurrence rate for this tumor is approximately 10%. Achieving complete surgical resection of the tumor is critical for improving disease-free survival. In cases where total resection is not feasible, adjuvant therapies such as radiotherapy or chemotherapy may be utilized to prolong disease-free survival. In the case series by Schauwecker et al., 17 the duration of follow-up was from 11 months to 10 years for 6 cases with no evidence of recurrence.
GPC is characterized by a low malignant potential and a low likelihood of recurrence. In our case, during follow-up, the patient showed no signs of recurrence, underscoring the effectiveness of the treatment approach.
Conclusion
GPC is a rare sinonasal tumor. Endoscopy, CT, and MRI are used in the diagnostic algorithm to characterize lesions and determine their extent. The backbone of treatment is surgical resection, which can be performed endoscopically, externally, or combined approach. A long-term follow-up of all cases with GPC is required for optimal clinical care and early-recurrence detection.
Footnotes
Authors Contributions
Feras Alkholaiwi: Study design and conception, writing of the draft, and approval of the final manuscript. Ji Yun Choi: review of the draft and approval of the final manuscript.
Data Availability
Data were included in the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent and Ethical Approval
Written informed consent was obtained from the patient for their anonymized information to be published in this case. Institutional review board approval of our hospital was obtained for this study.