
Abstract
Introduction:
Otosclerosis is a progressive, autosomal dominant hereditary disease of temporal bone causing tinnitus, and conductive hearing loss. Stapes surgery is safe and effective treatment with evidence suggesting tinnitus improvement corelates with hearing restoration. This systematic review evaluates evidence related to tinnitus improvement and hearing restoration following stapedectomy.
Methods:
This systematic review was prepared in accordance with the Preferred Reporting Item for Systematic Review and Meta-Analysis-P statement. The search included bibliographic databases like MEDLINE, EMBASE, the Cumulative Index of Nursing and Allied Health Literature, and Cochrane Library from inception until June 2024. The review included all studies reporting tinnitus severity and hearing outcomes post-stapes surgery. Outcome measures were tinnitus severity, hearing improvement, and timeframe of improvement. This review was registered with PROSPERO (CRD42024566593).
Result:
The initial search generated 609 studies from multiple databases, of which 22 studies involving 2233 patients were included. Due to heterogeneity in study design, patient population, and outcome measures used, pooling of data for meta-analysis was not feasible. Most of the studies were prospective in nature (77.3%), conducted in university hospitals (45.5%), and the average mean age of patients ranged from 18 to 75 years, predominantly females (60.7%). Most studies reported improvement of tinnitus severity post-stapes surgery 15.7% to 64% (median 46.3%), only fewer studies noted worsening among 2.9% to 11% patients. Hearing outcomes were consistently positive among majority of the studies, and only a small subset of patients reported no improvement or worsening. There was a moderate-to-strong relation between tinnitus improvement and air-bone gap (ABG) closure (32%), tinnitus resolution versus ABG closure (55%). More than 50% of the studies reported adherence to the Strengthening the Reporting of Observational Studies in Epidemiology quality assessment checklist.
Conclusion:
The systematic review indicates that stapes surgery improves degree of tinnitus severity and hearing outcomes and has moderate-to-strong correlation between resolution in tinnitus versus ABG closure. Most patients experienced significant improvement within 6 months.
Introduction
Otosclerosis is a progressive, autosomal dominant hereditary disease of human temporal bone clinically characterized by the presence of conductive hearing loss and intact tympanic membrane and middle ear.1,2 Tinnitus occurs in ~60% to 85% of patients with otosclerosis, manifesting variable degree of severity.3 -5 Despite extensive research, the underlying mechanisms of tinnitus remain poorly understood.6,7 However, existing theories suggest that abnormal bone remodeling, particularly the formation of highly-vascularized bone tissues in otosclerosis may contribute to pulsatile tinnitus by affecting sound transmission through altering middle ear dynamics.8,9 Further studies have suggested that tinnitus may also result from cochlear otosclerosis by disrupting the inner ear fluid dynamics that triggers the release of toxic metabolites causing tinnitus development.10,11
Stapes surgery has widely been recognized as safe and effective treatment for improving hearing outcomes in patients with otosclerosis. It has very positive outcomes in treating hearing loss of otosclerosis; however, its impact on tinnitus improvement remains inconsistent and underexplored. Anecdotal evidence suggests tinnitus tends to improve in conjunction with improved hearing outcomes following stapedectomy.12 -15 However, only a few studies have quantified the improvement of tinnitus and the prognostic factors of improvement.
A recent prospective study involving 48 patients reported significant improvement in tinnitus severity among 91% of the patients who underwent stapes surgery, with a clear positive correlation observed between hearing restoration and tinnitus reduction. Chang and Cheung in a prospective, within-subject study investigated changes in tinnitus loudness and hearing outcomes following stapedectomy. The study enrolled 26 patients, of whom 16 patients reporting severe preoperative tinnitus. Among those with sever preoperative tinnitus, 85% experienced significant improvement in tinnitus outcomes within the first 6 months with the greatest reduction observed within first 30 days. Furthermore, the study demonstrated a strong correlation between tinnitus improvement and hearing outcomes, predominantly in patients with severe preoperative tinnitus. However, the study did not explicitly measure the timeframe for observed improvements following stapes surgery. 16
Rationale
One key limitation addressed in many of these studies is the lack of a standardized approach to defining and measuring the degree of tinnitus improvement. While very few studies used validated tools such as Tinnitus Functional Index (TFI) and Visual Analogue Scales (VAS) to quantify the tinnitus severity, the majority rely on subjective patient reporting questionnaires or non-standardized scales leading to inconsistencies in quantifying the outcomes, making comparison between studies difficult. Furthermore, a precise timeframe for tinnitus improvement is poorly understood, as some studies reported improvements within 6 months, while others observed changes within the first 1 to 3 months post-stapedectomy. Although hearing restoration and tinnitus improvements co-occurred, very few studies systematically explored them independently.
Given these limitations, there may be merit in pooling and synthesizing data from different studies for more robust and reliable conclusions. Additionally, no systematic review around this topic has been conducted in the past 6 years, underscoring the need for an updated and thorough analysis. The current systematic review therefore aimed to critically appraise, synthesize, and present the available evidence related to tinnitus improvement and hearing restoration following stapedectomy.
Objectives
The systematic review aimed to critically appraise, synthesize, and present the available evidence related to tinnitus improvement following stapedectomy. The specific review questions are as follows:
What is the impact of stapedectomy on the severity of tinnitus in patients with otosclerosis?
What is the correlation between tinnitus improvement and hearing improvement following stapedectomy in patients with otosclerosis?
What is the timeframe for observed improvement in tinnitus following stapedectomy in patients with otosclerosis?
Materials and Methods
The current systematic review is prepared in accordance with the Preferred Reporting Item for Systematic Review and Meta-analysis (PRISMA-P) statement. 17 RefWorks was used to manage citations and remove duplicates. 18 This protocol has been registered with PROSPERO (CRD42024566593; https://www.crd.york.ac.uk/prospero/#recordDetails)
Eligibility Criteria
The systematic review included, peer-reviewed, English-language primary research studies investigating the impact of stapes surgery on tinnitus and hearing. The search was conducted from inception up to June 2024. Furthermore, e-mail alerts were set up on Medline® to ensure that no recent papers were missed during the time of writing. The Population-Intervention-Comparator-Outcomes-Study design criteria will be used to select the studies eligible for inclusion in the review. 19
The review includes all studies reporting findings of adult patients (>18 years) diagnosed with otosclerosis and have undergone stapedectomy or stapedotomy. It will also include studies that reported outcomes related to tinnitus severity using scales such as VAS, Tinnitus Handicap Inventory (THI), and TFI. Studies reporting hearing improvement (including changes in air conduction (AC), bone conduction (BC), and air-bone gap [ABG]) will also be included in the review.
Exclusion
We excluded case reports, case series, protocols, letters, editorials, commentaries, books and book chapters, dissertations, grey literature including conference abstracts, clinical practice guidelines and systematic, scoping, or narrative reviews. Non-English language papers were also excluded from this systematic review. Studies that do not clearly report tinnitus outcomes were also excluded from this review.
Population-Intervention-Comparator-Outcomes-Study
Population
The review included all studies that examined the impact of stapes surgery on the severity of tinnitus in patients with a diagnosis of otosclerosis.
Intervention
All studies reporting stapes surgery (stapedectomy) in patients with clinical diagnosis of otosclerosis were included.
Comparator
A comprehensive search did not find any Randomized Controlled Trial (RCT), so no comparator was used in this study.
Outcome Measures
The primary outcome measures in this review are as follows:
Severity of Tinnitus: The pre- and postoperative changes in tinnitus severity were measured using VAS, THI, Tinnitus Severity Index. The review also considered the proportion of patients reporting improvement specifically in scales of complete, partial, or no improvement.
Hearing Improvement: In terms of hearing improvement or severity of hearing loss, the review assessed pre- and post-scores of pure-tone audiometry (PTA), ABG measured using AC and BC, and speech discrimination scores.
Timeframe of Improvement was measured by comparing the preoperative scores versus time to onset of improvement post-surgery at different follow-up intervals such as after 1, 3, and 6 months.
The patient-reported outcomes around the impact of tinnitus of stapes surgery on tinnitus patients with otosclerosis were measured using quality of life (QoL) questionnaires, for example, SF-36, subjective patient satisfaction surveys.
The measured effect primarily focused on improvement in tinnitus and hearing outcomes based on pre- and post-changes/scores post-stapedectomy at different time intervals.
Information Sources
Search Strategy and Electronic Sources
The literature search was performed by 2 independent researchers N.A.L. and B.T. following the PRISMA-S guidance using a search strategy peer-reviewed by H.H. Following bibliographic databases like MEDLINE, EMBASE, the Cumulative Index of Nursing and Allied Health Literature (CINAHL), and Cochrane Library via Wiley were searched from inception until June 2024. The search also included controlled vocabulary National Library of Medicine’s Medical Subject Headings, and keywords. All duplicate records between MEDLINE and CINAHL were identified through the EBSCOhost interface. A detailed search strategy is provided in the Appendix. The reference list of all included studies was reviewed for any additional publication that might meet the inclusion criteria of this study.
Data Extraction
A standardized data extraction form was developed to ensure the uniformity of data collection and capture all relevant information across all studies. The following key variables were collected: author, year of publication and country, study design, duration, etc., in terms of participant characteristics, population details, pre- and post-tinnitus severity, pre- and postoperative hearing thresholds, types of surgery, correlation between tinnitus improvement and hearing, etc. Two reviewers independently extracted the data to minimize errors and potential biases.
Data Synthesis
Due to clinical and methodological heterogeneity in study designs, data collection tools, and outcome measures, a narrative approach to data synthesis was deemed appropriate.
A descriptive summary of the findings was reported specifically around how tinnitus severity and hearing threshold changed post-stapedectomy. The study reported patient satisfaction and timeframe for improvement based on the follow-up scores. The risk of bias across the studies was discussed using Newcastle-Ottawa Scale for cohort studies. The data synthesis followed the PRISMA flow diagram for study selection process and the PRISMA checklist ensuring comprehensive reporting.
Risk of Bias and Quality Assessment of the Studies
Two reviewers independently assessed the quality, any disagreement was resolved by consensus, or a third reviewer was contacted for resolution. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist for cohort, case-control, and cross-sectional studies (combined) was used to assess the quality of papers included in this review. It consists of a 22-item checklist assessing the quality of studies as well as risk of bias, generalizability, and reliability. The studies were categorized based on adherence levels, excellent (>85), good (70%-85%), adequate (60%-70%), and below 60 were considered as poor. 20
Results
Study Screening
A comprehensive review of papers published from the inception until June 30, 2024, yielded a total of 609 records from multiple databases. After removing the duplicates, 451 unique articles were found. An additional 341 articles were excluded during the title and abstract review stage due to inappropriate study design, outcome measures, or because they were review articles, case reports, or grey literature. A further 110 full-text articles were assessed, with 19 meeting the criteria for data extraction. Additionally, 3 studies were identified through manual search, resulting in 22 studies that were found to be relevant and were included for the final analysis (see Figure 1).
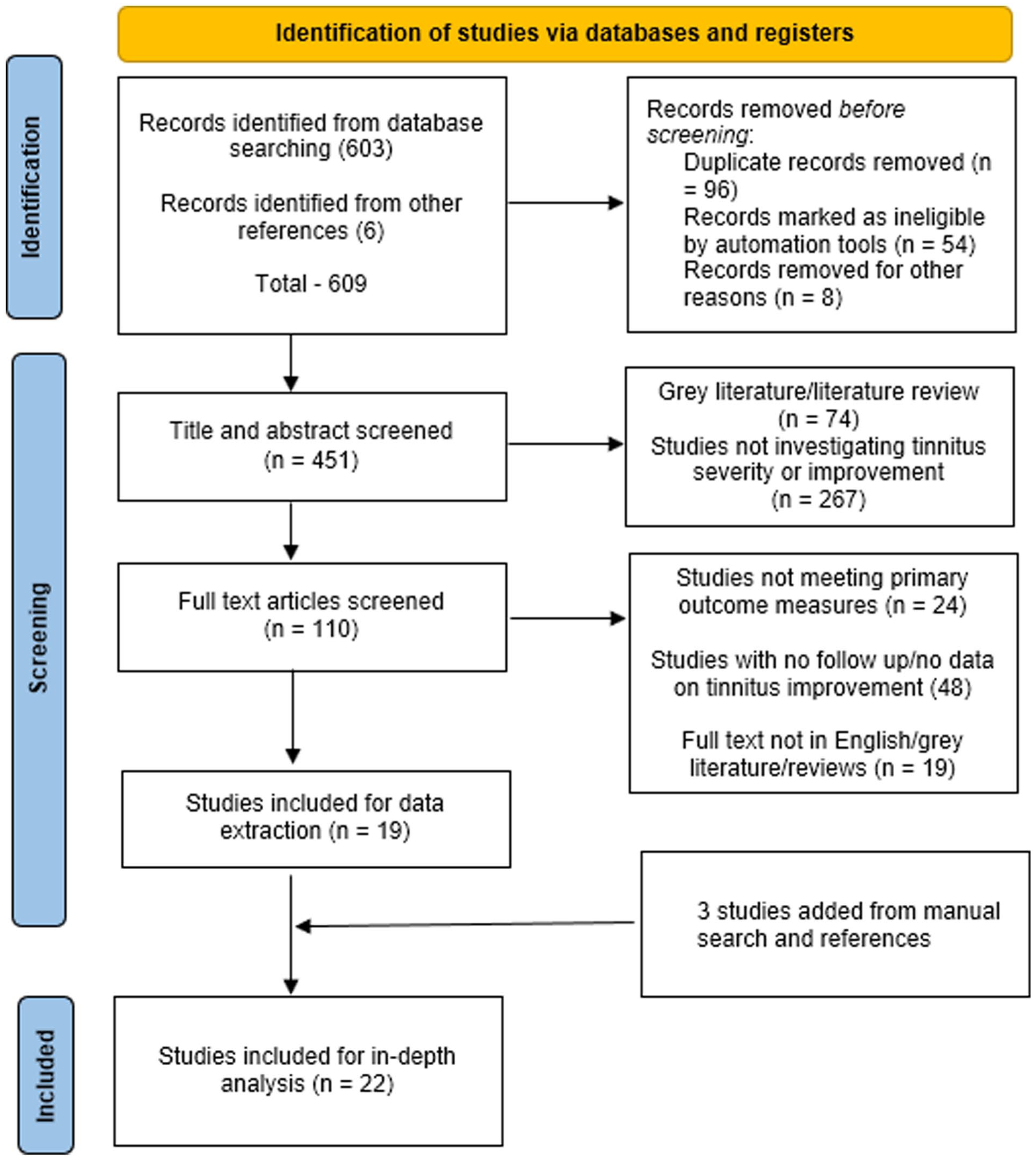
PRISMA flowchart describing systematic review search and study selection.
Demographic Characteristics
Most of the studies originated from Poland 4 (18.2%), followed by United States and Brazil, both representing 3 (13.6%). Other countries represented include France, Germany, Italy, Turkey, Belgium, China, Jordan, Iran, and Finland, each contributing 1 to 2 studies. Most of the studies (17; 77.3%) were prospective in nature while 5 (22.7%) studies followed a retrospective study design. In terms of study setting, most studies (10; 45.45%) were conducted in university hospitals, while 8 studies (36.36%) took place in tertiary referral centers, 3 (14.45%) studies were carried out in clinical settings in hospital or private clinic, while 1 study did not mention the setting used. The studies were conducted between 1996 and 2023, with the majority being carried out within the last decade. The sample size of tinnitus patients who underwent stapes surgery ranged from as low as 13 patients to as high as 643 patients. The average mean age of patients ranged from 18 to 75 years, with 60.7% of patients being female in comparison with males 39.3%. Patients were followed up for a minimum of 1 month post-surgery to a maximum of 55 months.
Outcome Measures and Tools Used
The outcome measures used in the studies included focused primarily on assessing tinnitus severity, hearing thresholds, and QoL. Several tools were used to assess the tinnitus and hearing outcomes. While TFI, VAS, and THI were used to evaluate the impact and intensity of tinnitus, PTA including AC, BC, and ABG were used to measure the change in hearing thresholds. Moreover, to assess patient QoL and overall satisfaction post-surgery, tools such as the Glasgow Benefit Inventory (GBI) and Clinical Global Impression-Severity (CGI-S) were used. PTA and TFI were used together in 6 studies. PTA and VAS were combined in 3 studies, while PTA and THI were used together in 2 studies. While more comprehensive assessment incorporating PTA, TFI, and the GBI was reported in 2 studies, 9 studies used tools such as PTA, VAS, THI, and others like Questionnaire for Tinnitus (QTN) or CGI-S independently to measure the tinnitus severity and hearing outcomes.
Quality Assessment of the Included Studies
Risk of bias and quality assessment was conducted using the STROBE checklist. The studies revealed variance in adherence across different studies, and the results section demonstrated greater variability in reporting. While very few studies reported data on patient flow, main findings, and subgroups, several studies lacked information around participant recruitment and outcome data. The majority of the studies (18/82%) were categorized as “good” or “adequately” adherent to the reporting guidelines as well as quality, and 4 (18%) studies were “excellent” in terms of quality and reporting. No study scored below 60% (poor), indicating overall reasonable study quality.
Tinnitus Improvement and Severity Posttreatment
Twenty-two studies assessed tinnitus improvement following stapes surgery. Almost all the studies reported improvements in tinnitus severity in patients at different stages. The percentage of patients experiencing total remission of tinnitus symptoms ranged from 15.7% to maximum of 64% with a median of 46.3%, while the percentage of patients reporting partial improvement ranged from 16% to 75% across different studies. While no change in tinnitus severity ranged from 2.9% to 11%, only fewer studies reported worsening of tinnitus severity post-stapedectomy, and the percentage of patients ranged from 2.9% to 11%. In terms of postoperative scores, studies used standardized tools to evaluate the tinnitus improvement, wherein scores ranged from slight to severe.
Hearing Improvement
In terms of hearing improvement, all 22 studies reported significant improvements in hearing, particularly in ABG reduction, measured by PTA. Hearing outcomes were consistently positive across studies, with no cases of hearing deterioration reported in most patients. ABG Closure of more than 10 dB was achieved in 70% to 94% of cases. Significant hearing improvement was reported in majority of the studies, with ABG scores ranging from 20.7 to 36.6 dB preoperatively, 4 to 12 dB postoperative, respectively, and mean hearing improvement ranged from 18.6 to 25.4 dB. Only a very small subset of studies mentioned minimal cases where hearing did not improve, but these instances were rare. However, 1 study did not explicitly state the hearing improvement, though it still indicated positive outcomes regarding tinnitus relief.
Correlation Between Tinnitus and Hearing Improvement Post-Stapedectomy
Several studies measured the tinnitus improvement and hearing restoration post-stapedectomy using key indicators such as PTA and ABG closure. While several studies have reported strong correlation between tinnitus improvement and ABG closure (hearing improvement), studies reported patients with ABG closure ≤10 dB had 50% to 70.7% tinnitus improvement (37, 5, and 13). However, Dziendziel et al reported weak correlation between ABG closure and tinnitus improvement, that is, only 37% experienced complete tinnitus resolution despite good hearing restoration. In relation to PTA, hearing gain of more than 20 dB improvement in PTA showed direct improvement in tinnitus. 24
Timeframe of Observed Improvement
Most studies reported significant hearing improvement in the early period (first 3 months postoperatively), particularly in ABG reduction, with outcomes remaining stable over the following months. Eighty-five percent of patients with severe preoperative tinnitus showed improvement within the first 30 days. A similar trend was observed in tinnitus outcomes, where some studies noted stable symptom improvement over time. However, most papers indicated that a significant proportion of patients experienced no further changes in tinnitus outcomes during the follow-up period. These findings suggest that while hearing improvement is a reliable and stable outcome, tinnitus relief tends to plateau in the subsequent months.
Discussion
Statement of Key Findings
The current systematic review reported the impact of stapedectomy on tinnitus and hearing improvement in patients with otosclerosis. The studies included were primarily conducted in university hospitals and tertiary referral centers, which demonstrated that stapedectomy leads to significant improvements in hearing, particularly in ABG reduction, with most patients experiencing either complete or partial hearing recovery. Tinnitus severity also showed notable improvement, with complete remission reported in 15.7% to 64% of patients and partial relief in 16% to 75%. Only a small percentage (2.9%-11%) experienced worsening tinnitus postoperatively.
Various standardized tools, including PTA, TFI, VAS, and THI, were used to assess tinnitus severity and hearing thresholds. Risk of bias and quality assessment using the STROBE checklist indicated that most studies were of good-to-excellent quality, although some lacked detailed reporting on patient recruitment and outcome measures. The timeframe analysis suggested that while hearing improvement remains stable over time, tinnitus relief plateaus after an initial period of improvement. These findings reinforce the effectiveness of stapedectomy in addressing both hearing loss and tinnitus in otosclerosis patients, with hearing improvement being a more consistent and stable outcome than tinnitus relief. The variability in results across studies may be partially explained by varying population characteristics and different surgical techniques and the heterogenous nature of tinnitus.
Interpretation of Key Findings
Despite noticeable increase in studies focusing on tinnitus severity and hearing outcomes post-stapedectomy in patients with otosclerosis, majority of studies originate from Europe and North America; however, little is known about tinnitus severity in Middle East and Africa. This systematic review therefore highlights a clear gap in understanding tinnitus severity and managing its complications in diverse population across the globe. Limited research in tinnitus severity could be due to under reporting due to cultural factors, poor research priority, insufficient funding, or lack of specialized academic health care centers. Furthermore, no systematic review has been conducted on this topic in the last 5 years.
While all previous studies have reported significant improvement in tinnitus severity post-stapedectomy in patients with otosclerosis, their effectiveness and degree of improvement varied across the studies.21 -26 For example, Dziendziel et al reported that significant reduction in tinnitus severity post-stapedotomy in 55% of patients, with 37% achieving complete remission. 15 However, in a similar study Sobrinho et al observed 91% of patients reporting either a reduction or total remission of tinnitus following stapes surgery, this is much higher success rate than the previous study. 5 These discrepancies may be attributed to differences in study design, patient selection, follow-up duration, and evaluation methods.
The correlation between tinnitus improvement and hearing restoration following stapedectomy was the key focus of this study. The findings suggest that studies that reported greater closure of ABG (≤10 dB) demonstrated better tinnitus improvement with most of the patients achieving complete resolution of symptoms. This reinforces the hypothesis that middle ear mechanics plays pivotal role in tinnitus improvement. While majority of studies showed a positive correlation between tinnitus improvement and hearing restoration, few studies also reported moderate tinnitus improvement without proportional improvement in hearing outcomes,27 -32 attributed mostly due to cochlear function, central auditory plasticity, and preexisting sensorineural hearing loss. Further studies have reported that patients with partial hearing loss had lower chance of tinnitus improvement even after a successful surgery.33 -36 Therefore, experts recommend a thorough examination before the surgery to identify patients who would benefit from tinnitus relief post-stapedectomy.
The timeframe for tinnitus improvement post-stapedectomy varied across the studies, with most of the studies indicating early relief before 3 months.24,36 -38 For example, Chang and Cheung reported that 85% of the patients with severe form of preoperative tinnitus experienced significant improvement in their symptoms within first 30 days and further improvement in the next 3 months, respectively. A further study noted 97% of the patients reported tinnitus improvement within first 6 months post-stapedectomy. 39 These findings are promising, which suggest tinnitus improvement typically occurs within first 6 months post-surgery. While the long-term follow-up data demonstrated a steady improvement in hearing symptoms, tinnitus severity did not show any improvement after 12 months. This is an important finding and warrants adjunctive tinnitus management strategies for nonresponders beyond 12 months period.
In terms of quality assessment of the studies, the overall quality of studies included in this review was assessed using the STROBE checklist, and majority of the studies were rated as moderate-to-high quality, with no studies demonstrating poor quality. While few studies demonstrated methodological flaws, for example, inconsistent use of tinnitus assessment tools/scales, inconsistent follow-up data post-surgery and poor sample sizes might have contributed to variability in results. Furthermore, lack of standardized criteria or definition to report the tinnitus improvement across the studies further warrants better framework and tools for reporting the tinnitus outcomes.
There were several key limitations that must be acknowledged, most notably the heterogeneity in study designs, sample size, and outcome measures, which restricted the viability for data aggregation; consequently, a meta-analysis could not be performed. Owing to inconsistent use of tinnitus assessment tools, there is a lack of a standardized approach in defining and measuring the degree of tinnitus improvement and severity. Additionally, there is a lack of long-time follow-up for the included studies, potentially overlooking the long-term effect of stapes surgery on tinnitus and hearing outcomes. Despite these limitations, the current systematic review offers a comprehensive search strategy ensures a wide coverage of relevant literature from multiple databases and the review was prepared in adherence to the PRISMA-P guidelines. The studies were screened and synthesized independently by 2 independent researchers to minimize bias and ensure reliability of the finding. The review included a substantial number of papers involving a large patient population providing greater generalizability of the data. Furthermore, studies were assessed using the STROBE checklist for quality.
Future Research
Further research should focus on consistent use of validated scales such as TFI, VAS, THI rather than using self-reported measures. Studies should carefully assess the tinnitus outcomes for long term, that is, more than 1 year to confirm whether improvements are sustained. Future research should focus on multicentered RCTs to provide more robust data.
Conclusion
This systematic review demonstrates that stapedectomy effectively improves tinnitus severity and hearing outcomes in patients with otosclerosis, particularly those with complete ABG closure. While majority of the patients experienced significant relief of symptoms within first 3 to 6 months post-surgery, tinnitus improvement beyond 12 months is uncommon. Given these findings, it is imperative to conduct a detailed preoperative clinical evaluation to better predict postsurgical tinnitus outcomes. Future research should aim to standardize tinnitus assessment tools, longer follow-up, and identify predictive factors to guide clinical decision-making (Tables 1–5).
Tinnitus Assessment Scales and Degree of Improvement.
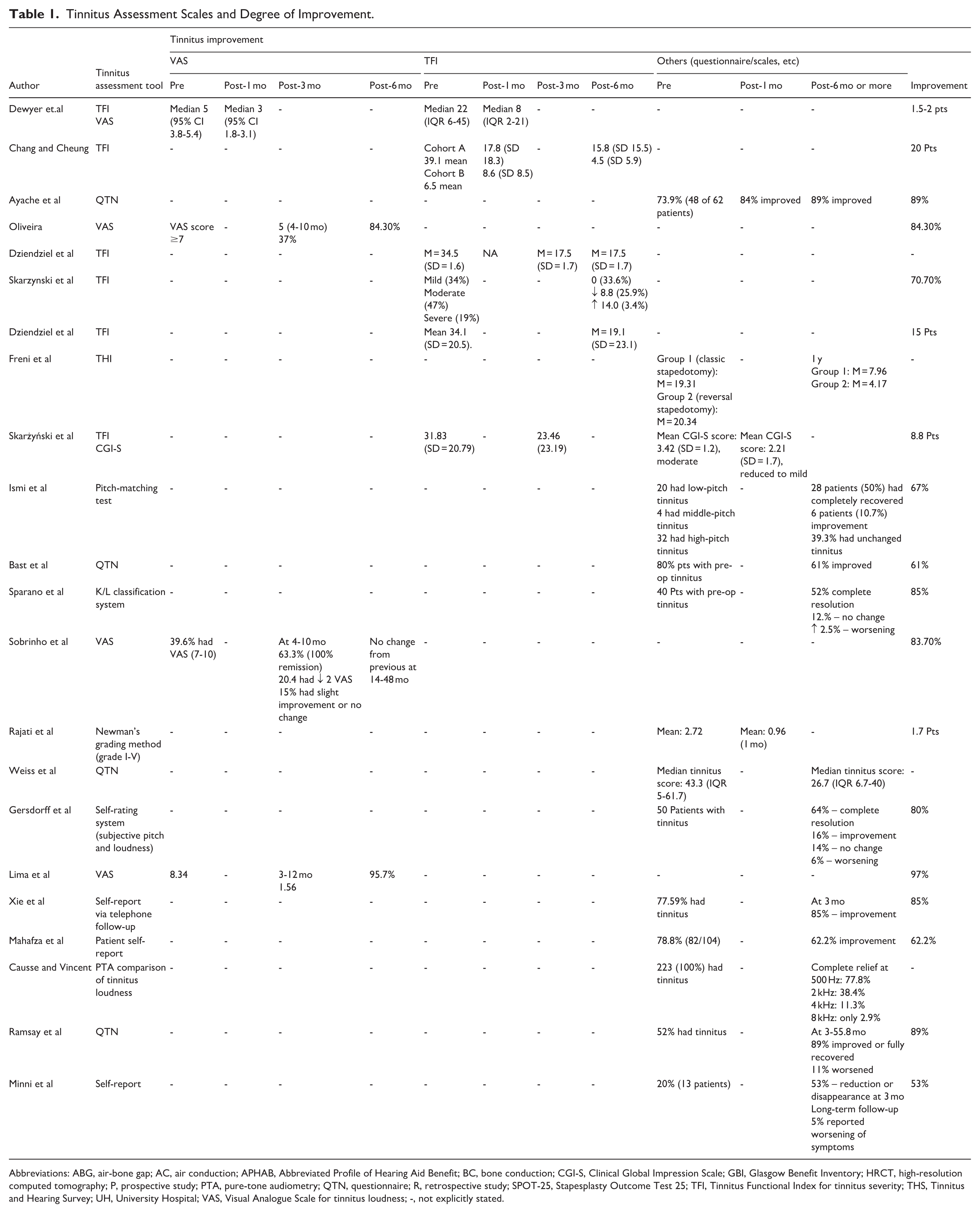
Abbreviations: ABG, air-bone gap; AC, air conduction; APHAB, Abbreviated Profile of Hearing Aid Benefit; BC, bone conduction; CGI-S, Clinical Global Impression Scale; GBI, Glasgow Benefit Inventory; HRCT, high-resolution computed tomography; P, prospective study; PTA, pure-tone audiometry; QTN, questionnaire; R, retrospective study; SPOT-25, Stapesplasty Outcome Test 25; TFI, Tinnitus Functional Index for tinnitus severity; THS, Tinnitus and Hearing Survey; UH, University Hospital; VAS, Visual Analogue Scale for tinnitus loudness; -, not explicitly stated.
Degree of Improvement.
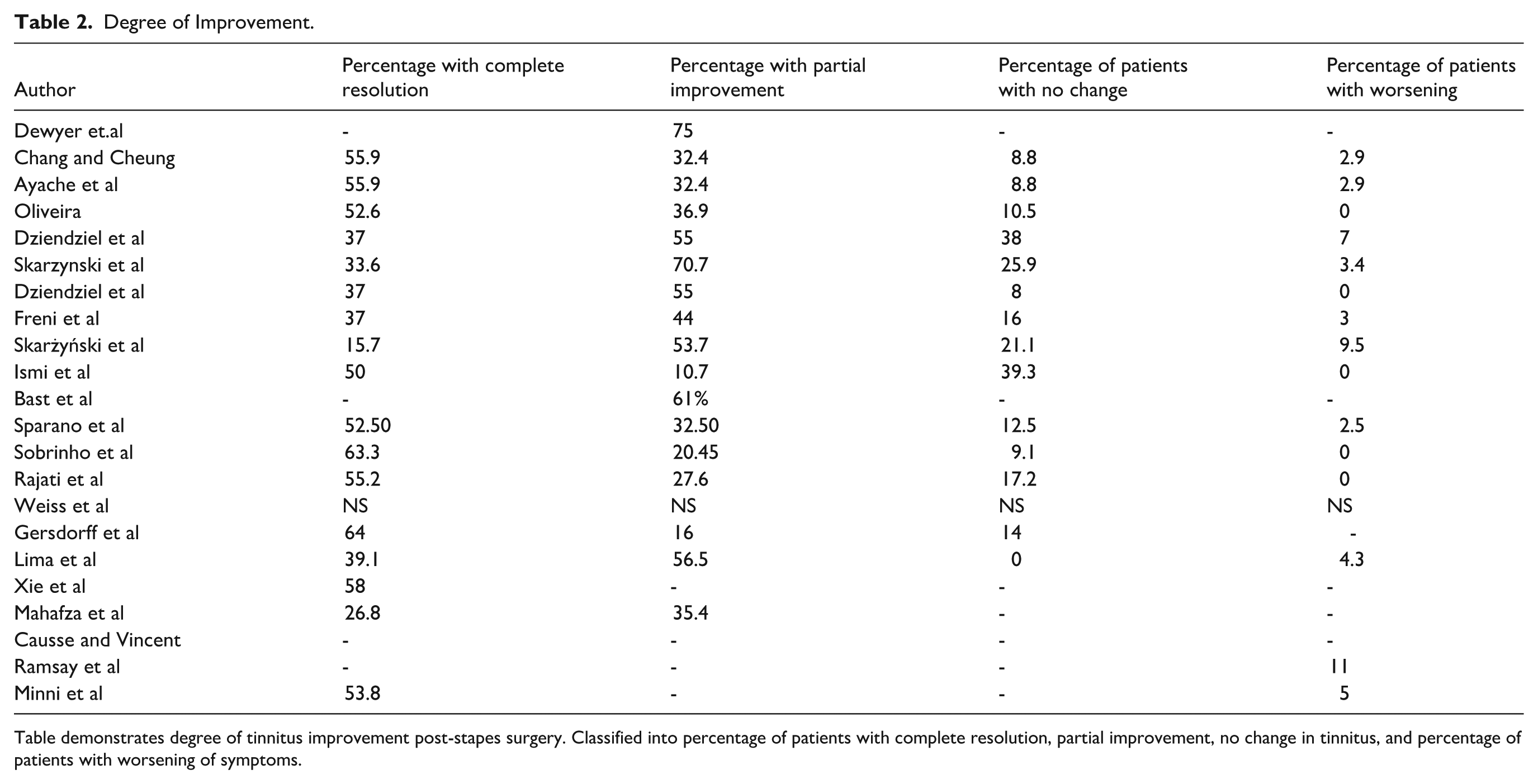
Table demonstrates degree of tinnitus improvement post-stapes surgery. Classified into percentage of patients with complete resolution, partial improvement, no change in tinnitus, and percentage of patients with worsening of symptoms.
Hearing Improvement and Different Tools Used.
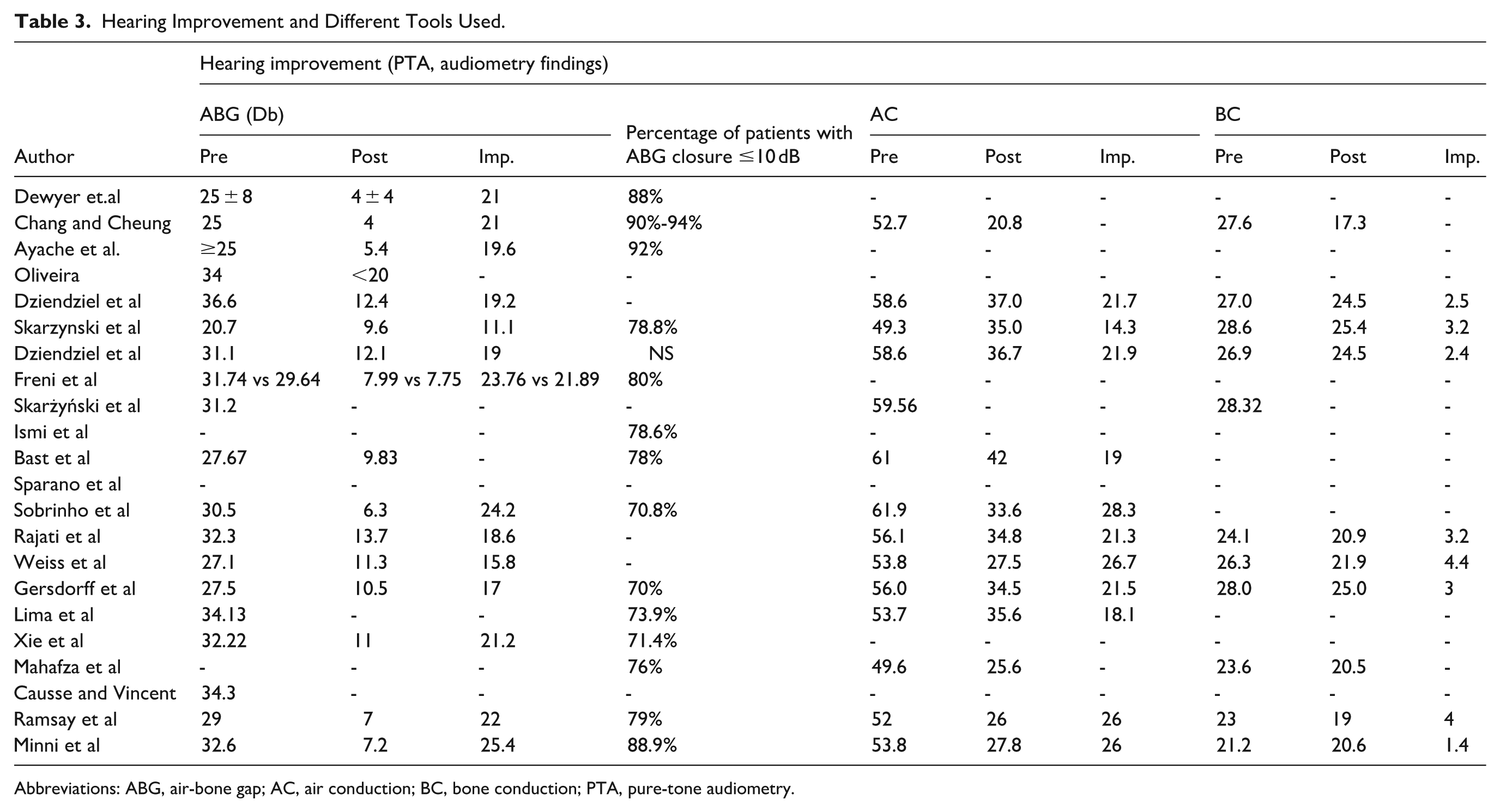
Abbreviations: ABG, air-bone gap; AC, air conduction; BC, bone conduction; PTA, pure-tone audiometry.
Correlation Between Tinnitus and Hearing Improvement (Strength of Correlation).
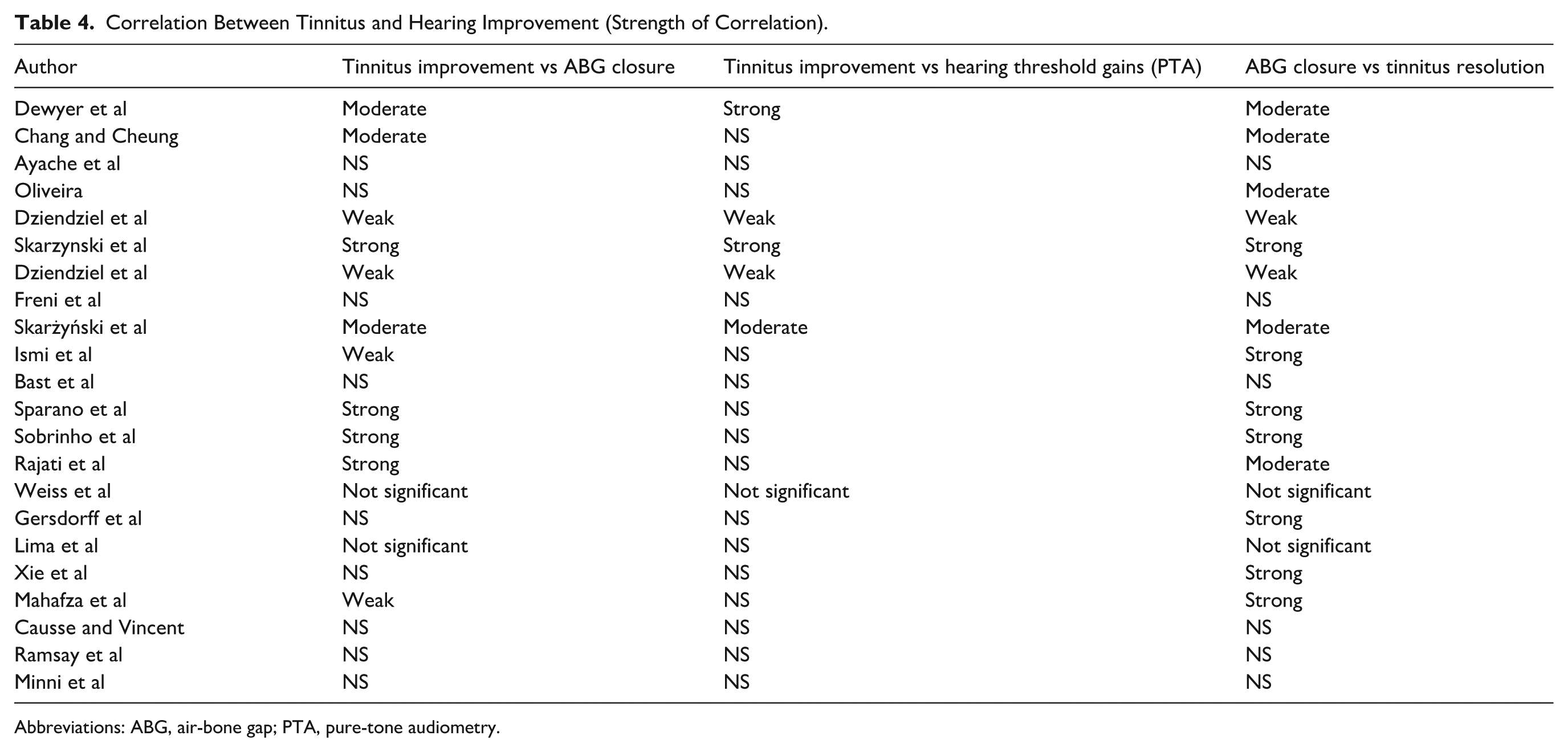
Abbreviations: ABG, air-bone gap; PTA, pure-tone audiometry.
Quality assessment using the STROBE checklist.
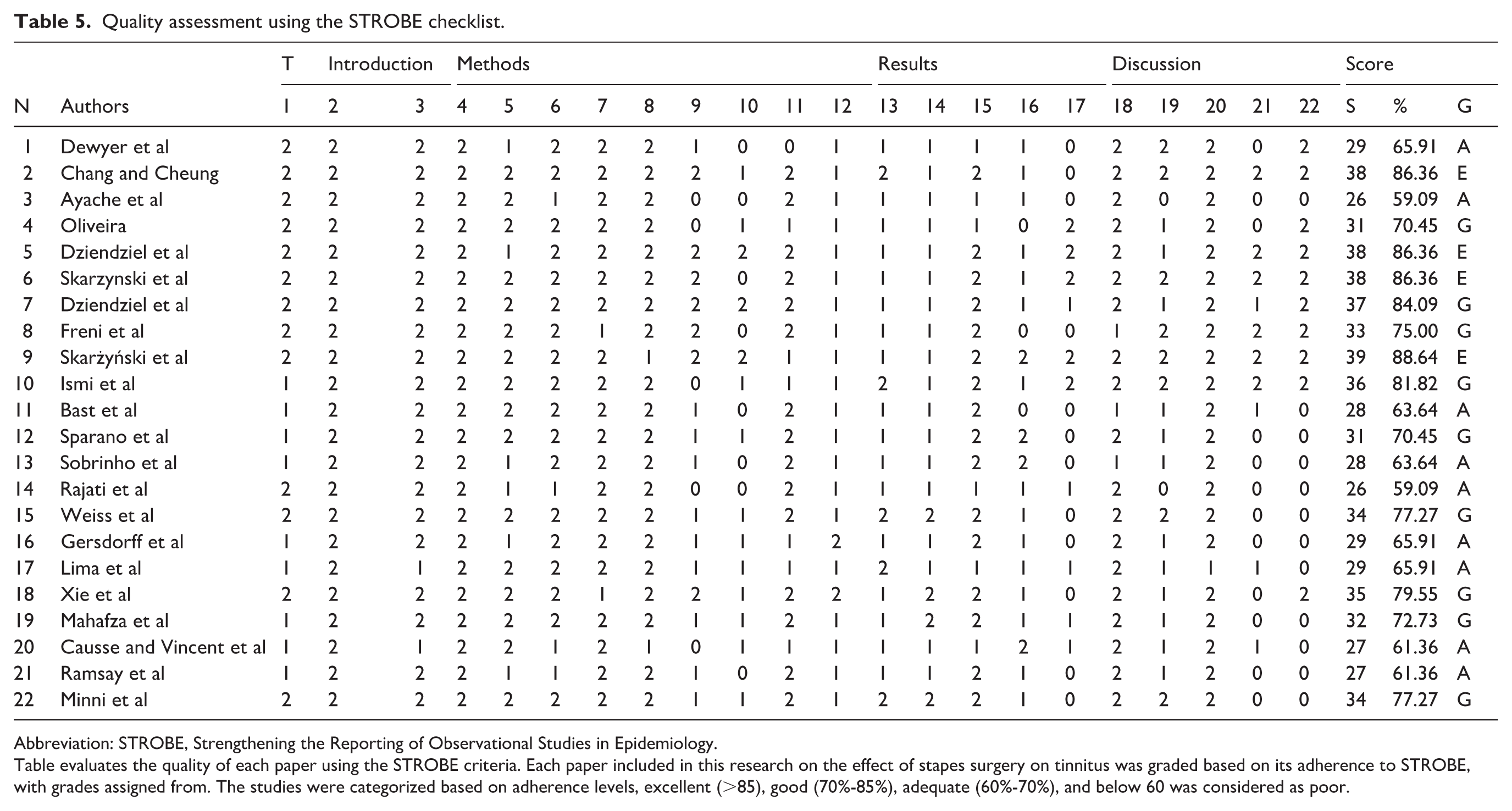
Abbreviation: STROBE, Strengthening the Reporting of Observational Studies in Epidemiology.
Table evaluates the quality of each paper using the STROBE criteria. Each paper included in this research on the effect of stapes surgery on tinnitus was graded based on its adherence to STROBE, with grades assigned from. The studies were categorized based on adherence levels, excellent (>85), good (70%-85%), adequate (60%-70%), and below 60 was considered as poor.
Footnotes
Appendix: Search Strategy (Medline and CINAHL)
(“Otosclerosis” [Mesh] OR otosclerosis) AND (“Stapes Surgery” [Mesh] OR “Stapedectomy” [Mesh] OR stapedectomy OR stapedotom* OR “stapes surgery”) AND (“Tinnitus” [Mesh] OR tinnitus OR “tinnitus severity” OR “tinnitus improvement” OR “tinnitus outcome” OR “Tinnitus Handicap Inventory” OR “THI” OR “TFI” OR “Visual Analog Scale” OR “VAS”) OR (“Hearing Loss” [Mesh] OR “Hearing Tests” [Mesh] OR hearing OR “hearing improvement” OR “hearing outcomes” OR “pure tone audiometry” OR PTA OR “air bone gap” OR “ABG”).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.