
Abstract
Background:
Tinnitus is the most common auditory disorder and can profoundly affect quality of life. It can contribute to various types of headaches, including chronic and recurrent forms. Dizziness is also among the most common complaints in medicine, affecting 15% to 35% of the general population at some point in their lives. Experiencing headache and dizziness simultaneously is often alarming, yet this combination can result from multiple causes ranging from dehydration to anxiety. This study aimed to examine the impact of tinnitus and dizziness on chronic and recurrent headaches among adults residing in Zahedan, southeastern Iran.
Methods and Materials:
This study utilized baseline data from the Zahedan Adult Cohort Study. Participants were enrolled according to the cohort’s inclusion criteria, while individuals with severe physical or mental disabilities or those unable to complete the questionnaire were excluded. Data were analyzed using descriptive statistics (frequency, mean, standard deviation, percentage) and logistic regression in SPSS 22. A significance level of P < .05 was applied. Logistic regression models were applied to assess associations between tinnitus, dizziness, and headache types, adjusting for potential confounders.
Results:
The participants had a mean age of 50.44 ± 9.18 years. The mean age at onset of chronic headache was 37.43 ± 11.90 years. The prevalence of chronic and recurrent headaches was 5.2% and 36.2%, respectively. Women had a significantly higher likelihood of developing chronic headaches compared with men (odds ratio [OR] = 3.2, 95% confidence interval [CI]: 2.5-4.0). Recurrent headaches were more prevalent in women (OR = 2.5, 95% CI: 2.3-2.7). Additionally, hypertension, head trauma, and epilepsy were associated with increased risks of both chronic and recurrent headaches.
Conclusion:
Chronic and recurrent headaches were influenced by demographic factors, socio-economic status, and medical conditions such as hypertension, and head trauma. Importantly, both tinnitus and dizziness significantly increased the odds of these headaches. Social determinants, neurological comorbidities, and vestibular dysfunction appear to play key roles. These findings underscore the need for integrated otolaryngological and neurological care.
Introduction
Tinnitus is a common condition characterized by the perception of ringing or other sounds in the ears or head without any external source, which affects ~10% of the population.1,2 While some individuals may adapt or ignore it, many face significant negative impacts on their quality of life 3 due to related issues like hyperacusis, 1 hearing loss, 4 depression,1,5 and headaches. 6 Tinnitus also places a substantial economic burden on the healthcare system, exceeding $15 billion annually in the United States. 7
Headache is a common sensation of pain or discomfort in the head or facial region, and it includes various subtypes such as migraine, tension-type headache (TTH), and cluster headache. It can also be classified as primary or secondary, with primary headaches being the most frequent and affecting about 3 billion people annually. 8 Headaches are the leading cause of neurological consultations, 9 affecting an estimated 66% of the general population across their lifespan. 10 Accordingly, the co-occurrence of headaches in patients with tinnitus is not unexpected. Although the precise prevalence of headaches among individuals with tinnitus remains unclear, both conditions can share overlapping symptoms, such as pain or discomfort, and in some cases, one can even trigger or worsen the other.
Chronic headache is defined as a headache that occurs on at least 15 days/month for a period of 3 months or more, and represents a major cause of pain and disability in affected individuals. 11 Many patients with idiopathic tinnitus also report headaches.12,13 The recurrent nature of both conditions suggests their frequent co-occurrence. 14 Most population-based studies have primarily investigated migraine as a risk factor in adults and have consistently demonstrated a strong bidirectional relationship between tinnitus and headache. 15
Substantial evidence suggests that certain forms of idiopathic headache and tinnitus share common pathophysiological mechanisms. Imaging findings from both animal and human studies have demonstrated a close relationship between tinnitus and abnormal activity in central auditory pathways secondary to hearing loss.16,17 Furthermore, significant evidence indicates that alterations in thalamocortical activity play a key role in the pathogenesis of both tinnitus and headaches.18 -20
Recent animal studies suggest that the trigeminal nerve, located at the level of the dorsal cochlear nucleus, can directly influence the activity of central auditory pathways. 21 Aberrant activity in the trigeminal system, involving both peripheral and central components, contributes to the development of primary and secondary headaches, including migraine. 22 This highlights the critical role of the trigeminal system in the pathophysiology of both idiopathic headache syndromes and tinnitus.
Dizziness is a common clinical complaint, with one-third of American adults seeking medical advice for it at some point in their lives. While many cases are attributable to benign causes, serious conditions like stroke or increased intracranial pressure may also present with dizziness. Therefore, a step-by-step diagnostic approach is crucial to differentiating among potential etiologies.23,24 Patients are typically asked to describe their symptoms, as dizziness presents an erroneous perception of movement, often accompanied by blurred or darkened vision. This contrasts with true vertigo, which involves a distinct spinning sensation. Both dizziness and vertigo can be disabling, often remaining unexplained in 40% to 80% of patients, yet exerting a substantial impact on social and personal functioning and disrupting daily activities. 24
In some conditions, such as vestibular migraine, tinnitus, dizziness, and headache may co-occur. Vestibular migraine is considered the second most common cause of concurrent dizziness and headache, affecting ~3% of the adult population. 25
Understanding the relationship between tinnitus, dizziness, and headaches is crucial for accurate diagnosis and effective treatment, as these symptoms may arise from a variety of causes. Research in this area can facilitate more precise diagnoses, enhance quality of life for affected adults, and help identify risk factors that may inform preventive strategies. Accordingly, this study aimed to investigate the association of tinnitus and dizziness with chronic and recurrent headaches in adults participating in the Zahedan Adult Cohort Study in southeastern Iran.
Materials and Methods
This cross-sectional investigation used baseline information from the Zahedan Cohort Study in southeastern Iran, as part of the Prospective Epidemiological Research Initiatives in Iran (PERSIAN). The research included 10 016 participants aged between 35 and 70 years, with recruitment and data collection conducted in Zahedan from October 2015 to January 2019. The study’s rationale, aims, and methodology have been detailed in previous publications. 26
Ethical Considerations
Ethical considerations and participant confidentiality were strictly upheld throughout the research process. All the participants gave informed written consent before their involvement and were informed of their right to withdraw from the study at any time. The study was approved by the Ethics Committee of Zahedan University of Medical Sciences (IR.ZAUMS.REC.1403.139).
Eligibility Criteria
The criteria for eligibility to participate in the study included being an Iranian citizen, aged between 35 and 70 at the time of the baseline assessment, having resided in Zahedan for at least 9 months for local residents, and having maintained residency for a minimum of 1 year if migrating from other areas. Data collection began after obtaining informed written consent. Participants who did not meet the inclusion criteria or who had serious physical or mental health problems that affected their ability to complete questionnaires or attend visits to the cohort center were excluded from the study.
Participants were selected randomly from the Zahedan population through a multi-stage sampling method. The city was divided into 3 zones based on socio-economic status, and a central health center was chosen in each zone. Participants were randomly selected from the population blocks of the health centers. The study comprised a total of 10 016 participants.
Measurements
The questionnaires used in this study were previously validated within the PERSIAN Cohort Study, 27 covering areas such as general information, socio-economic status, and medical history. Socio-economic status (SES) for each participant was determined based on data about infrastructure facilities (eg, drinking water source, sanitation), housing features (eg, number of rooms, type of home ownership), ownership of durable assets (eg, dishwasher, car, television), and education level. Participants were then classified into 5 SES quintiles, from the lowest (first) to the highest (fifth).
All participants were interviewed by an expert physician familiar with the local dialects and languages. Participants provided self-reported responses to the following questions: Have you ever experienced dizziness (a sensation of disorientation or light-headedness) that significantly interfered with your daily activities? Have you ever suffered from tinnitus (a sound in the ear or head without an external stimulus) that lasted longer than 1 week? Have you ever experienced a history of chronic and recurrent headaches? Have you ever suffered a head injury that resulted in any period of unconsciousness, however brief? Have you ever had recurrent headache attacks that lasted at least 4 hours each (occurring at least twice)? Have you experienced chronic headaches lasting 15 days or more per month?
Statistical Analysis
Data were summarized as frequencies and percentages. Logistic regression analysis (both simple and multiple models) was used to examine the relationships of demographic characteristics, comorbidities, tinnitus, and dizziness with chronic and recurrent headache. Logistic regression served as a modeling procedure to estimate the odds of binary outcomes while adjusting for potential confounding variables. The associations were expressed as odds ratios (ORs) with 95% confidence intervals (CIs). Both overall model fit and the statistical significance of individual predictors were assessed, with a P < .05 regarded as statistically significant.
Results
A total of 10 016 adults participated in this study, with a mean age of 50.44 ± 9.18 years. The majority of the participants were female (60.9%) and married (88.3%). Approximately half of the participants identified as Sistani ethnicity, and 21.8% were classified as illiterate. Employment rates were recorded at 57.8% among males and 11.4% among females. The prevalence rates for hypertension, epilepsy, and a history of head trauma were 25.8%, 1.5%, and 6.6%, respectively. Chronic headache was reported by 5.2% of participants, of whom 91.8% were under treatment. The mean age for the onset of chronic headache was 37.43 ± 11.90 years.
Chronic headache was more likely to occur in women (OR = 3.2, 95% CI: 2.5-4.0; P < .001), individuals aged 41 to 50 years compared to those over 60 years (OR = 1.8, 95% CI: 1.3-2.4; P < .001), participants of Baluch (OR = 2.1, 95% CI: 1.5-2.8; P < .001), or Sistani (OR = 1.8, 95% CI: 1.4-2.5; P < .001) compared to Fars ethnicity. Additionally, individuals with very poor socio-economic status were more likely to report chronic headache compared to those with very good status (OR = 1.3, P = .049). The likelihood of chronic headache was also higher among participants with hypertension (OR = 1.3, 95% CI: 1.1-1.6; P = .002), epilepsy (OR = 3.8, 95% CI: 2.4-5.9; P < .001), and a history of head trauma (OR = 1.6, 95% CI: 1.2-2.2; P = .001). Conversely, employment was associated with a 50% reduction in the odds of chronic headache (P < .001; Table 1).
ORs of Chronic Headache According to Demographic Factors and Medical Conditions.
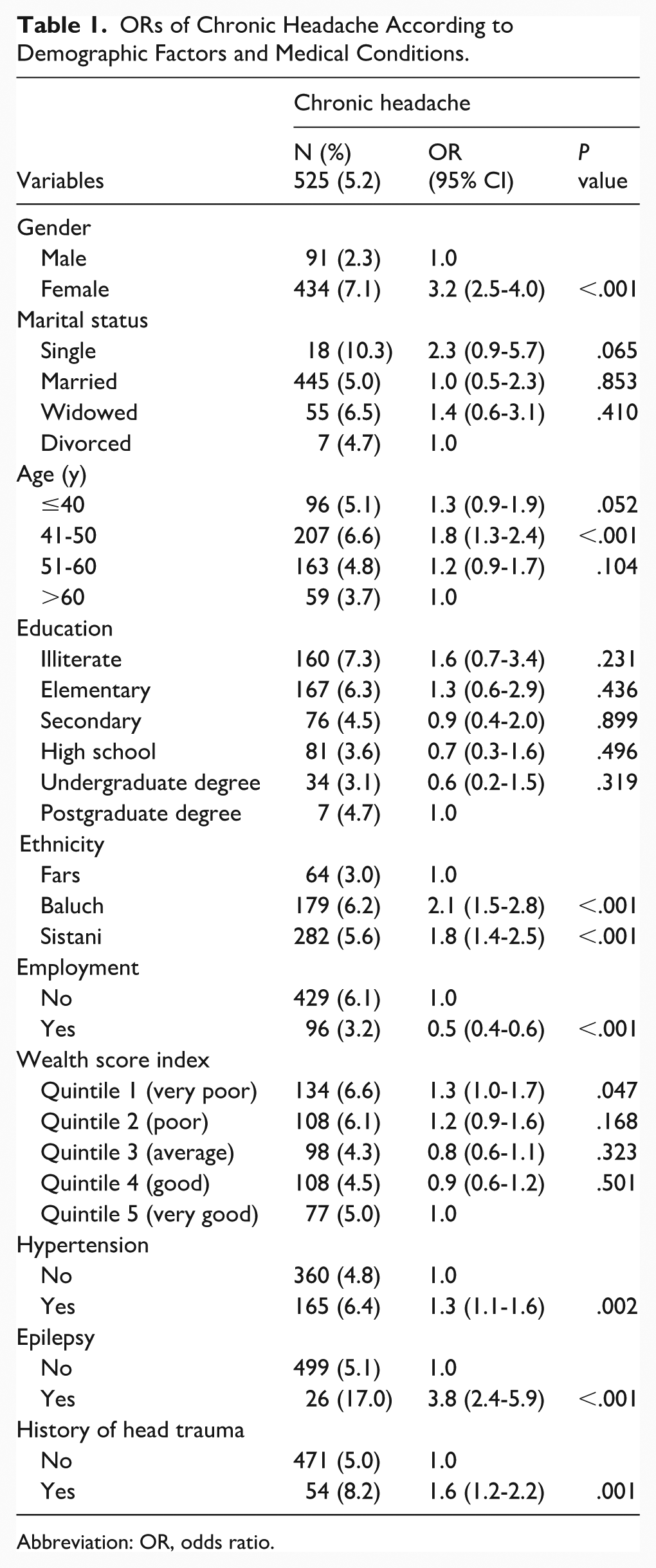
Abbreviation: OR, odds ratio.
The odds of chronic headache were 2.1 times higher in individuals with tinnitus (P < .001), even after adjusting for confounding factors. Similarly, the odds were 3.4 times higher in those with dizziness (P < .001; Table 2).
Crude and Adjusted ORs of Chronic Headache in People With Tinnitus and Dizziness.
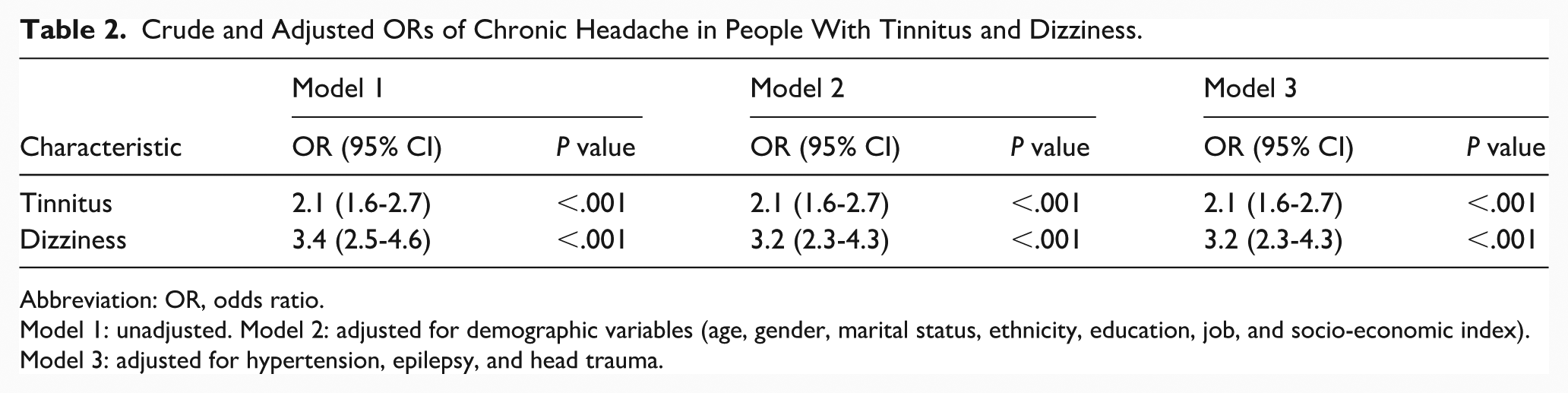
Abbreviation: OR, odds ratio.
Model 1: unadjusted. Model 2: adjusted for demographic variables (age, gender, marital status, ethnicity, education, job, and socio-economic index). Model 3: adjusted for hypertension, epilepsy, and head trauma.
The prevalence of recurrent headache was 36.2%. Recurrent headache was more likely in women (OR = 2.5, 95% CI: 2.3-2.7; P < .001), people aged up to 50 years compared to those older than 60 years (OR = 1.6, 95% CI: 1.4-1.9; P < .001), illiterate individuals compared to those with postgraduate degree (OR = 1.4, 95% CI: 1.0-2.0; P = .047), Baluch (OR = 1.8, 95% CI: 1.6-2.0; P < .001) and Sistani (OR = 1.2, P < .001) compared to Fars ethnicity, and people with very poor (OR = 1.2, P = .002) and poor (OR = 1.1, P = .016) compared to those with satisfactory socio-economic status. Furthermore, it was more likely in people with hypertension (OR = 1.2, 95% CI: 1.1-1.3; P < .001), epilepsy (OR = 2.5, 95% CI: 1.8-3.5; P < .001), and blow to the head (OR = 1.7, 95% CI: 1.4-2.0; P < .001). However, the odds of recurrent headache decreased 40% in employed individuals (P < .001; Table 3).
OR of Recurrent Headaches According to Demographic Factors and Medical Conditions.
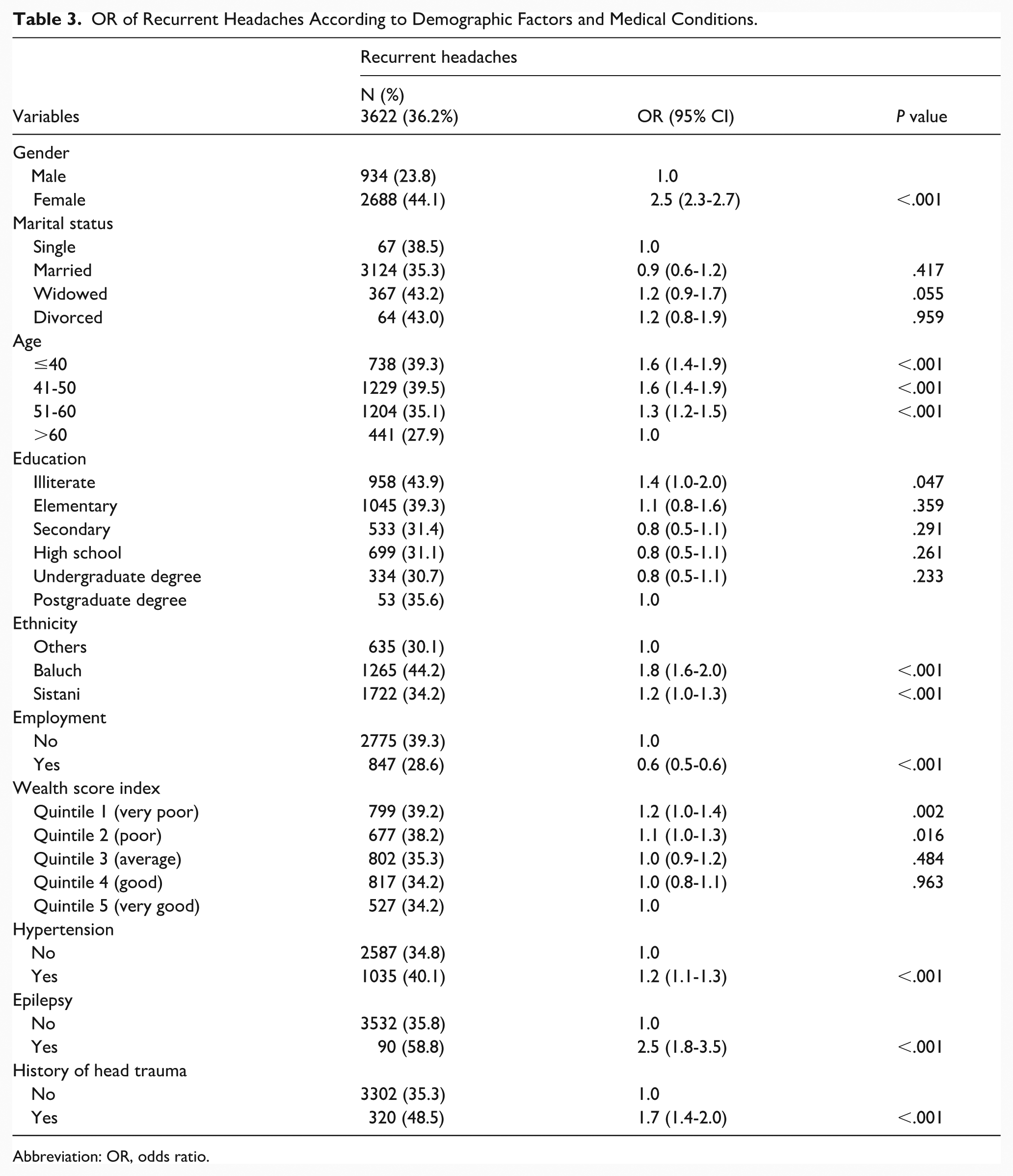
Abbreviation: OR, odds ratio.
The odds of recurrent headache were 2.2 times higher in people with tinnitus (P < .001), even after adjusting for confounding factors. Similarly, it was 1.9 times higher in individuals with dizziness (P < .001; Table 4).
Crude and Adjusted ORs of Recurrent Headaches in People With Tinnitus and Dizziness.
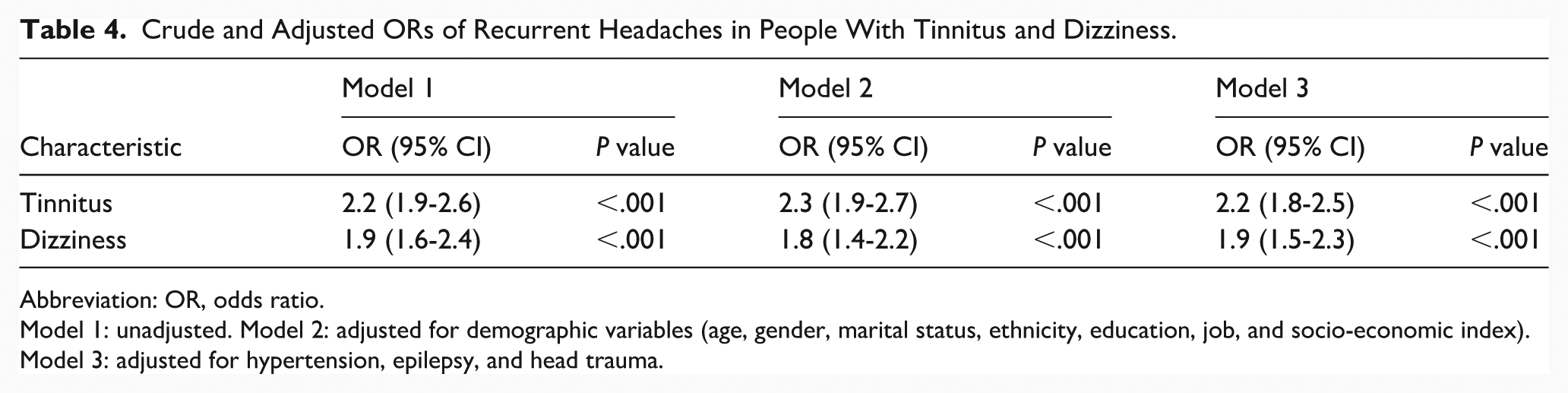
Abbreviation: OR, odds ratio.
Model 1: unadjusted. Model 2: adjusted for demographic variables (age, gender, marital status, ethnicity, education, job, and socio-economic index). Model 3: adjusted for hypertension, epilepsy, and head trauma.
Discussion
This study investigated the association of tinnitus and dizziness with chronic and recurrent headaches in adults aged 35 to 70 in Zahedan, southeastern Iran. The results indicated that tinnitus and dizziness significantly increased the likelihood of developing chronic and recurrent headaches. This relationship remained robust even after adjusting for confounding variables, suggesting a bidirectional association between these auditory/vestibular symptoms and various headache types.
The study reported a recurrent headache and chronic headache prevalence of ~36.2% and 5.2%, respectively. The likelihood of recurrent headache was more in women, younger participants, and those with a history of hypertension and epilepsy. Women and employed individuals as well as participants with a poor socio-economic status, hypertension, head trauma, and epilepsy were more likely to have chronic headache.
These results align with the study by Logo (2020) in Sweden, which examined the relationship between headache and tinnitus in 2539 individuals. The authors concluded a strong correlation between the severity of tinnitus and headache, with the association strengthening as tinnitus severity increased. The Swedish study also indicated a gender effect, with women experiencing headaches having more likelihood of tinnitus than men. This may be due to the greater prevalence of headache disorders, Tempromandibular Joint (TMJ) issues, and stress among women, factors that can contribute to both tinnitus and headaches. 28
Nowaczewska et al in Poland investigated the prevalence of different headache types in 286 patients with tinnitus. The study, conducted between February 2019 and May 2020, used the Tinnitus Handicap Inventory (THI) to measure tinnitus severity and the Visual Analog Scale to assess tinnitus loudness. Participants provided information on tinnitus location (ears or head), laterality (bilateral or unilateral), and severity. Headache diagnoses were based on the International Classification of Headache Disorders, third edition (ICHD-3). 11 The study found that 141 (49%) of the patients with tinnitus experienced headaches.
Younger age and female gender were associated with a higher likelihood of developing headaches. Additionally, individuals with bilateral tinnitus showed a higher prevalence of headaches. Among the patients with tinnitus who reported headaches, 42 experienced migraines and 94 reported tension headaches. 29
Langguth et al investigated the relationship between tinnitus and headache in individuals aged 18 to 90 at the Tinnitus Center of the University of Regensburg in Germany (2003-2011). Tinnitus severity was assessed using the Tinnitus Questionnaire, and headache classification followed the ICHD-2 criteria. The authors concluded that while tinnitus and headache may not occur concurrently, they are interrelated through shared pathophysiological mechanisms, such as migraine or trigeminal neuralgia, which can predispose individuals to both conditions. 30
Guichard et al investigated the relationship between tinnitus and headache in adults. Using data from a cohort-based population of French-speaking university students and higher education centers, 5729 participants completed self-report questionnaires. The results indicated that of the participants, 3246 had no headache history, 838 had non-migraine headaches, 1645 had migraines (744 with aura), and 331 reported tinnitus. Multivariate analysis, classifying participants into groups based on headache status (no headache, with headache, migraine without aura, migraine with aura), revealed an increased risk of tinnitus in individuals with migraine headaches. Notably, a strong association was found between migraine with aura and tinnitus compared to migraine without aura. Overall, migraine was estimated to account for 43% of tinnitus cases in this study population. This figure rose to 52% for individuals experiencing migraine with aura. No significant differences were found in this association between men and women. 31
Research on the relationship between tinnitus and headache in cohort-based populations is scarce, and the association of tinnitus and dizziness with headache has been particularly understudied.6,32 Existing studies have largely focused on hypothetical analyses to identify factors related to tinnitus in the ear6,32 or have reported tinnitus symptoms in patients with headache. However, results from the National Health and Nutrition Examination Survey (NHANES) indicated a substantial overlap, with 44.6% of individuals with tinnitus also experiencing migraines. Furthermore, multivariate logistic regression analysis from NHANES suggested that patients with tinnitus in the ears have a higher likelihood of suffering from migraines. 8
Tinnitus and headache, both are associated with specific changes in the activities of the thalamocortical system, which overlap with each other. One of the major reasons for dizziness, along with factors such as Meniere’s disease, vestibular neuritis, and head trauma, is the presence of vestibular migraine, which is usually accompanied by migraine headaches. Diagnostic guidelines for vestibular migraine emphasize the simultaneous occurrence of headache and dizziness symptoms, including imbalance.
All kinds of vascular malformations can produce headache and tinnitus. Both are more prominent in arteriovenous malformations (AVMs) and arteriovenous fistula. The headaches in individuals with AVMs often fulfill criteria for migraine with aura. The tinnitus often occurs episodically. Both tinnitus and headaches are more common in individuals with vascular abnormalities located to the posterior fossa, and the tinnitus may be a relevant symptom in lesions near the VIII nerve. 25
This study revealed a significant association between tinnitus and chronic headaches, with individuals experiencing tinnitus being 2.1 times more likely to report them. Similarly, dizziness was associated with a 3/2 increase in the likelihood of chronic headache. These associations remained even after adjusting for confounding factors and highlighted the nature of the relationship between these conditions. This relationship may stem from shared neural pathways, vestibular disorders, or common triggers like stress and sleep disturbances. SES and employment also significantly influenced headache prevalence. Very poor economic status increased the likelihood of both chronic and recurrent headaches, while employment significantly reduced headache prevalence, potentially due to better access to resources, healthcare, and structured routines. These findings emphasize the significant role of social determinants in health outcomes, and the need for targeted interventions to address these inequalities. Additionally, this study revealed that individuals with a history of epilepsy had an increased risk of developing chronic and recurrent headaches, with ORs of 3.8 and 2.5, respectively. This aligns with research by Ottman et al, who studied 1948 patients with epilepsy and found that patients with epilepsy had twice the risk of migraine headaches compared to those without epilepsy. 33
Mutlu in Turkey investigated the relationship between epilepsy and headache in 420 individuals between January and June 2016. He concluded a significantly higher prevalence of headaches in patients with epilepsy. 34 The results suggested that the increased activity in central nervous system following seizures or attacks in patients with epilepsy contributes to a higher occurrence of various types of headaches.
This study also found that hypertension in participants was associated with an increased risk of chronic and recurrent headaches. This aligns with a study by Stewart on 200 individuals with severe hypertension, which associated hypertension to severe headaches primarily driven by anxiety and stress. 35
Kiechl et al investigated the prevalence of primary headaches (migraine and tension-type) and cranial neuralgias in individuals aged 55 to 94 in Bruneck, Italy. Beginning with a baseline assessment in 1990 and continuing with 5 year follow-ups, the study included 574 men and women who underwent neurological and laboratory examinations, including a standardized headache interview. Their study revealed a combined prevalence of 51.7% for all primary headaches and 1.6% for cranial neuralgias. TTHs (40.9%) and migraine (19.3%) were the most common headache types. The 1 year prevalence of primary headaches was notably high (40.5%) in this age group, indicating a significant impact on health-related quality of life. The study provided crucial insights into the lifetime prevalence of primary headaches and cranial neuralgias in the general population. It also offered the first reliable data on primary headache prevalence based on the second edition of the ICHD-2. Interviews, conducted according to ICHD-1 criteria, gathered detailed information including pain location (unilateral or bilateral), quality, intensity, sensitivity to light, duration, and number of attacks. Participants reported headache frequency per day, week, month, or year. The study revealed that migraine lifetime prevalence was 28.5% in women and 8.7% in men, yielding a female-to-male ratio of 3.3:1. Migraine occurred in 28.4% of women aged 40 or older, and in 5.7% of women aged 60 or older.
This study found that the lifetime prevalence of TTH was 46.3% in women and 34.7% in men, with a sex ratio of 1.3:1. Episodic TTH occurred with similar frequency in both sexes, while chronic TTH was present in 2.8% of the study population. 36
In a 2004 study by Buse et al, data from the “Migraine Prevalence and Prevention Study in the United States” were analyzed. The study reported gender-specific prevalence estimates for migraine and other severe headache types, both overall and within different population groups. A total of 162 756 individuals aged 12 years and older participated in the 2004 survey, with a response rate of 64.9%. Among these respondents, 28 261 (17.4%) reported experiencing a “severe headache” in the past year—23.5% of women and 10.6% of men. Additionally, 11.8% of participants met the ICHD criteria for migraine—17.3% of women and 5.7% of men. The study’s results indicated significant gender differences in the prevalence of migraine and severe headaches, with both migraine and TTHs being more common in women than in men, consistent with our findings. 37
Studies consistently show a significant relationship between gender and headache occurrence, particularly migraines. Women are more susceptible to headaches than men due to biological factors (eg, hormonal fluctuations), psychological factors (eg, anxiety), and social factors (eg, daily life stressors). Understanding these differences is crucial for healthcare providers to offer more targeted and effective treatments. Future research should explore the precise roles of genetic, hormonal, and behavioral factors in these gender differences.
A 2001 cross-sectional study by Winter et al investigated the relationship between SES and different types of headaches, including migraine and non-migraine headaches. The study involved 36 858 female health professionals. 38
SES was determined using an index based on annual household income and education level. Headache information, specifically on migraine, migraine with aura, and non-migraine headaches, was gathered through highly reliable self-reports. The researchers used multivariate logistic regression models to analyze the association between SES and headache types. The study found that 12 140 (32.9%) of the women reported a history of some type of headache. Specifically, 6801 (18.4%) had a history of migraine, and 5339 (14.5%) experienced non-migraine headaches. Women with low SES showed a higher risk for all types of headaches:
Non-Migraine Headache: Adjusted OR = 1.22 (95% CI: 1.10-1.36).
Any Type of Migraine: Adjusted OR = 1.40 (95% CI: 1.28-1.54).
Migraine With Aura: Adjusted OR = 1.44 (95% CI: 1.23-1.69).
Migraine Without Aura: Adjusted OR = 1.38 (95% CI: 1.21-1.58).
Furthermore, among women actively suffering from migraines, low SES was associated with an increased likelihood of experiencing weekly or more frequent attacks (OR = 1.77, 95% CI: 1.26-2.49).
Winter et al found that low SES correlated with a higher prevalence of all headache types and increased migraine attack frequency. 39 These findings align with our own study’s conclusions. 38
Additionally, our study observed that younger individuals experienced all headache types more frequently than older individuals did. This aligns with a 2018 cross-sectional study by Torres-Ferrus et al in Spain, which investigated headache, comorbidity, and lifestyle in 1619 adolescents aged 12 to 20. Their research, conducted via anonymous questionnaire (14), reported a 30.5% prevalence of recurrent headaches, with 11.3% exhibiting migraine features. Notably, 32.9% experienced weekly or more frequent attacks, and 44.1% reported headache-related disability (Ped MIDAS scale). Headaches were more common in girls (35.1%) than boys (25.5%). The Spanish study also identified significant associations between headaches and poorer sleep hygiene, less physical activity, skipping breakfast, smoking, frequent caffeine consumption, chronic pain disorders, mental health problems, and allergies. 40
A study by Nieswand et al, conducted between March 2015 and March 2016, investigated headache frequency among German schoolchildren across different age groups. The research took place in 14 public schools in Dresden, Saxony, Germany, adhering to the principles of the Declaration of Helsinki. 39
Among the participating schools were seven 4 year primary schools, three 8 year secondary schools (with educational achievement of university entrance level II certificates), and four 6 year secondary schools (achieving secondary school level I certificates). Schools within a radius of 10 km around our medical school were selected. In doing so, they spanned a wide area of the city including areas with diverse socio-economic backgrounds. The questionnaire was distributed to 1969 elementary schoolchildren, 2060 students of 8 year secondary schools and 1390 students of 6 year education in secondary schools. In total, 5419 questionnaires were distributed to pupils from 7 to 19 years of age. All completed questionnaires were included in the analysis.
Students were given 1 week to complete the questionnaires, which were accompanied by a letter explaining the study’s purpose. A total of 2706 questionnaires were returned, representing a response rate of 49%. Response rates varied by school type: 63.7% for primary schoolchildren (1254 students), 43.5% for 8 year-old secondary school students (896 students), and 40.0% for 6 year-old secondary school students (556 students). The gender distribution was nearly equal, with 1362 girls (50.3%) and 1344 boys (49.7%), a ratio maintained across all school types. All completed questionnaires were included in the statistical analysis. Of the 2706 participants, 31.9% reported no headaches. However, more than two-thirds (68.1%) experienced headaches regularly: 36.6% reported headaches once a month, and 31.5% reported headaches at least twice a month. Among those experiencing headaches at least 2 days a month, the frequency distribution was as follows:
Fifty-five point five percent had headaches between 2 and fewer than 5 days a month.
Twenty-seven percent had headaches between 5 and fewer than 10 days a month.
Ten point five percent had headaches between 10 and fewer than 15 days a month.
Seven percent had headaches more than 15 days a month.
These findings generally support the notion that adolescents and young people exhibit a significantly higher prevalence of headaches compared to older individuals. This could be attributed to various pressures and problems such as academic demands, occupational stress, emotional issues, sleep disturbances, irregular sleep patterns, and extensive social media use. 39
The association of tinnitus and dizziness with chronic and recurrent headaches remains unclear. However, given the higher prevalence of chronic and recurrent headaches in patients with tinnitus and dizziness, we can infer that these individuals may exhibit increased central nervous system sensitivity, predisposing them to developing these types of headaches.41,42
Strengths and Limitations
This study used a large sample size (10 016 participants) and a validated questionnaire to gather data on tinnitus, dizziness, and headaches. Logistic regression models were employed to mitigate the influence of confounding variables. Another advantage of this study was the inclusion of a large sample size with high ethnic diversity, which enhances the generalizability of the data. However, limitations included the reliance on self-reported information, indicating the need for more valid and comprehensive tools for headache assessment. 43 Additionally, the study did not explore detailed dimensions of tinnitus and dizziness, such as intensity, frequency, and temporal variations. Another limitation of this test is the lack of audiological assessments, which should be given greater attention in future research.
Conclusion
This study revealed significant associations between tinnitus, dizziness, and headache disorders in adults in Zahedan, southeastern Iran. Demographic factors, SES, and health conditions such as hypertension, epilepsy, and head trauma influenced chronic and recurrent headaches. The strong association between tinnitus/dizziness and the increased likelihood of both chronic and recurrent headaches highlights the need for integrated management strategies. Addressing socio-economic inequalities and raising public awareness are essential steps in preventing and treating these conditions.
Future research should explore the underlying mechanisms related to these conditions to develop comprehensive interventions targeting both clinical and social determinants, in order to enhance patient care, improve quality of life, and reduce the overall burden on healthcare systems.
Footnotes
Acknowledgements
We would like to express our sincere appreciation and gratitude to Dr Amir Hossein Ghazizadeh Hashemi for his cooperation in the implementation of this project.
Ethical Considerations
This study received ethical approval from the Ethics Committee of Zahedan University of Medical Sciences (approval number: IR.ZAUMS.REC.1403.139).
Author Contributions
Conceptualization: Ali Reza Salar, Fariba Shahraki-Sanavi, and Mahmood Rezvani Amin. Data curation: Mahmood Rezvani Amin, Fariba Shahraki-Sanavi, and Zahra Sarhadi. Formal analysis: Mahdi Mohammadi and Alireza Ansari Moghaddam. Investigation: Mahmood Rezvani Amin, Mehdi Rezvani Amin, and Alireza Ansari Moghaddam. Methodology: Alireza Ansari Moghaddam, Ali Reza Salar, Fariba Shahraki-Sanavi, and Mehdi Rezvani Amin. Project administration: Alireza Ansari Moghaddam. Supervision: Alireza Ansari Moghaddam. Visualization: Alireza Ansari Moghaddam, Ali Reza Salar, Mehdi Rezvani Amin, and Zahra Sarhadi. Writing—original draft: Mahmood Rezvani Amin, Fariba Shahraki-Sanavi, and Mehdi Rezvani Amin. Writing—review & editing: Mahmood Rezvani Amin, Fariba Shahraki-Sanavi, Ali Reza Salar, Mehdi Rezvani Amin, and Alireza Ansari Moghaddam.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data will be available upon reasonable request from the corresponding author.