
Abstract
We report a case of cochleovestibular neurovascular compressive syndrome (CVCS)-induced drop attack treated with microvascular decompression (MVD) of the superior vestibular nerve. This report discusses the merits of surgical intervention through a review of related literature. A 58-year-old woman was referred to our clinic with a chief complaint of intermittent, strong, right-sided tinnitus lasting for a few seconds immediately prior to drop attack. Magnetic resonance imaging (MRI) showed bilateral neurovascular contact between the anterior inferior cerebellar artery (AICA) and the vestibulocochlear nerve. Based on MRI findings, history of present illness, and response to anticonvulsants, CVCS was suspected, and surgical decompression on the right side was subsequently performed. The patient became asymptomatic immediately after the surgery, and the vestibular-evoked myogenic potentials were normalized. No recurrence was reported during a 1-year follow-up period.
Introduction
Neurovascular compression of the cranial nerve has been reported to cause several clinical problems. 1 For example, neurovascular compression associated with the fifth, seventh, and ninth cranial nerves can consequently induce trigeminal neuralgia, hemifacial spasm, and glossopharyngeal neuralgia, respectively. Although medical therapies, such as anticonvulsants, have been utilized to improve these associated symptoms, microvascular decompression (MVD) has a relatively high success rate and effectiveness with less recurrence.2,3 Particularly, vestibulocochlear symptoms resulting from the eighth cranial nerve compression, referred to as cochleovestibular neurovascular compressive syndrome (CVCS), present as vertigo, tinnitus, or hearing disturbances. 4 Although the role of MVD for CVCS remains debatable, patients who are refractory to medications or have a tendency to relapse may require MVD for definitive treatment.4,5 Herein, we report the case of a patient with drop attack and tinnitus who underwent MVD of the superior vestibular branch of the eighth cranial nerve, which resulted in complete resolution.
Case Report
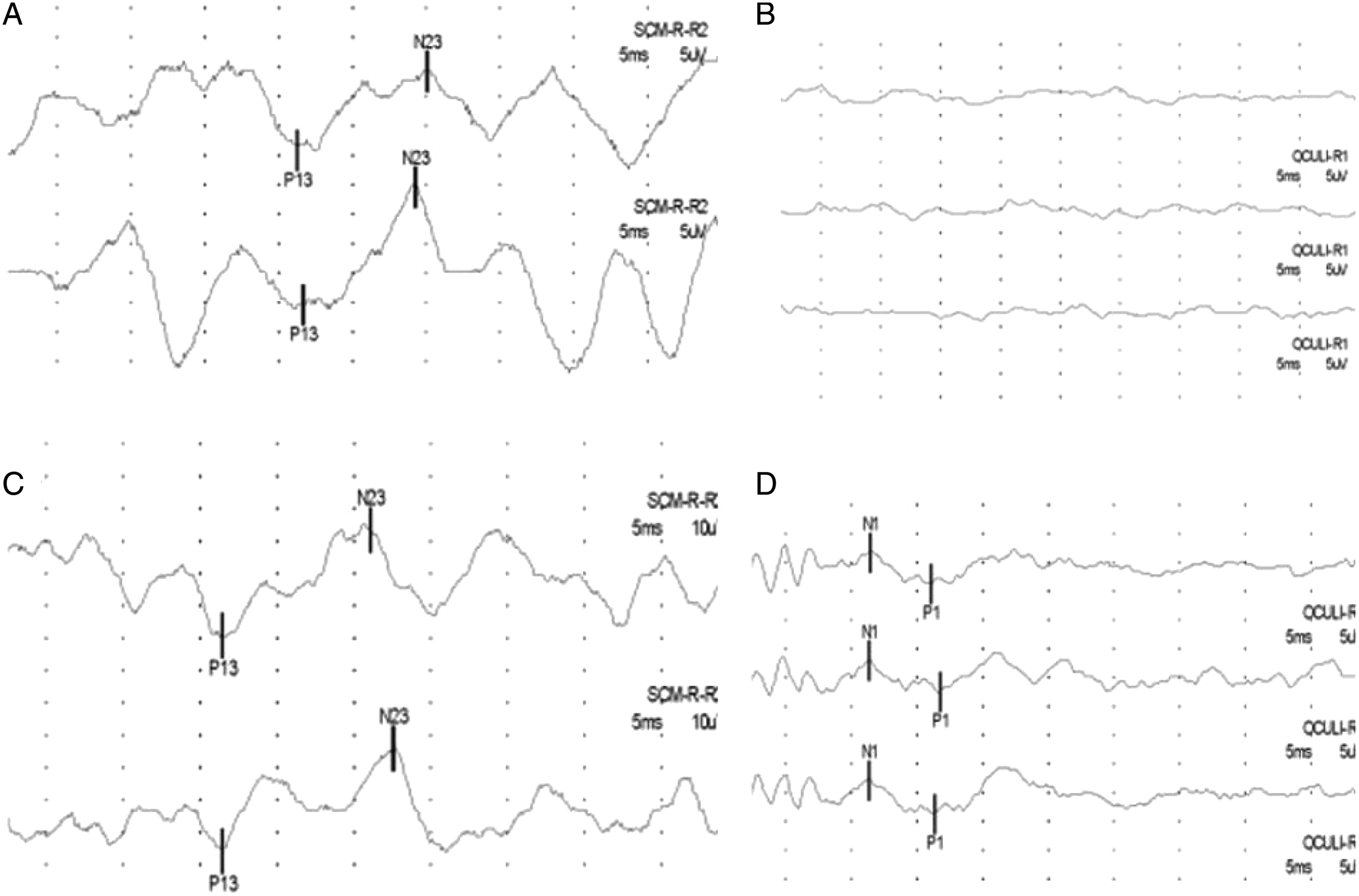
A 62-year-old woman with a 6-month history of tinnitus and vertigo was referred to our clinic for recurrent drop attacks. On admission, she complained of an intermittent, strong, right tinnitus lasting for a few seconds immediately prior to drop attack. Audiological assessment showed a pure tone average of 50 dBHL and 40 dBHL in the right and left ears, respectively, and her tinnitus handicap inventory (THI) score was 66, indicating a severe hearing handicap. Brain magnetic resonance imaging (MRI) was performed, which showed bilateral neurovascular contact between the anterior inferior cerebellar artery (AICA) and vestibulocochlear nerve (Figure 1). Subsequently, the cervical and ocular vestibular evoked myogenic potentials (cVEMP and oVEMP, respectively) were measured. Notably, oVEMP showed no response on the right side, whereas cVEMP showed decreased response amplitudes (Figures 2A, 2B). All other vestibular function test results were normal. Furthermore, 75 mg oxcarbazepine (Trileptal
(Left) Preoperative T2 magnetic resonance imaging (MRI) showing a complex of left VII and VIII in contact with a loop of the left anterior inferior cerebellar artery (AICA). (Right) The right side of the VII and VIII complexes also shows regions of conflict with the right AICA. Changes in vestibular-evoked myogenic potentials (VEMPs) of the right side before and after surgery. (A) Preoperative cVEMP and the amplitude range from 13.83 to 20.34 μV. (B) Preoperative oVEMP showing no response. (C) Postoperative cVEMP showing an increase in amplitude (32.52–33.36 μV) (D) Postoperative oVEMP shows the appearance of response, indicating functional recovery of the right superior vestibular nerve.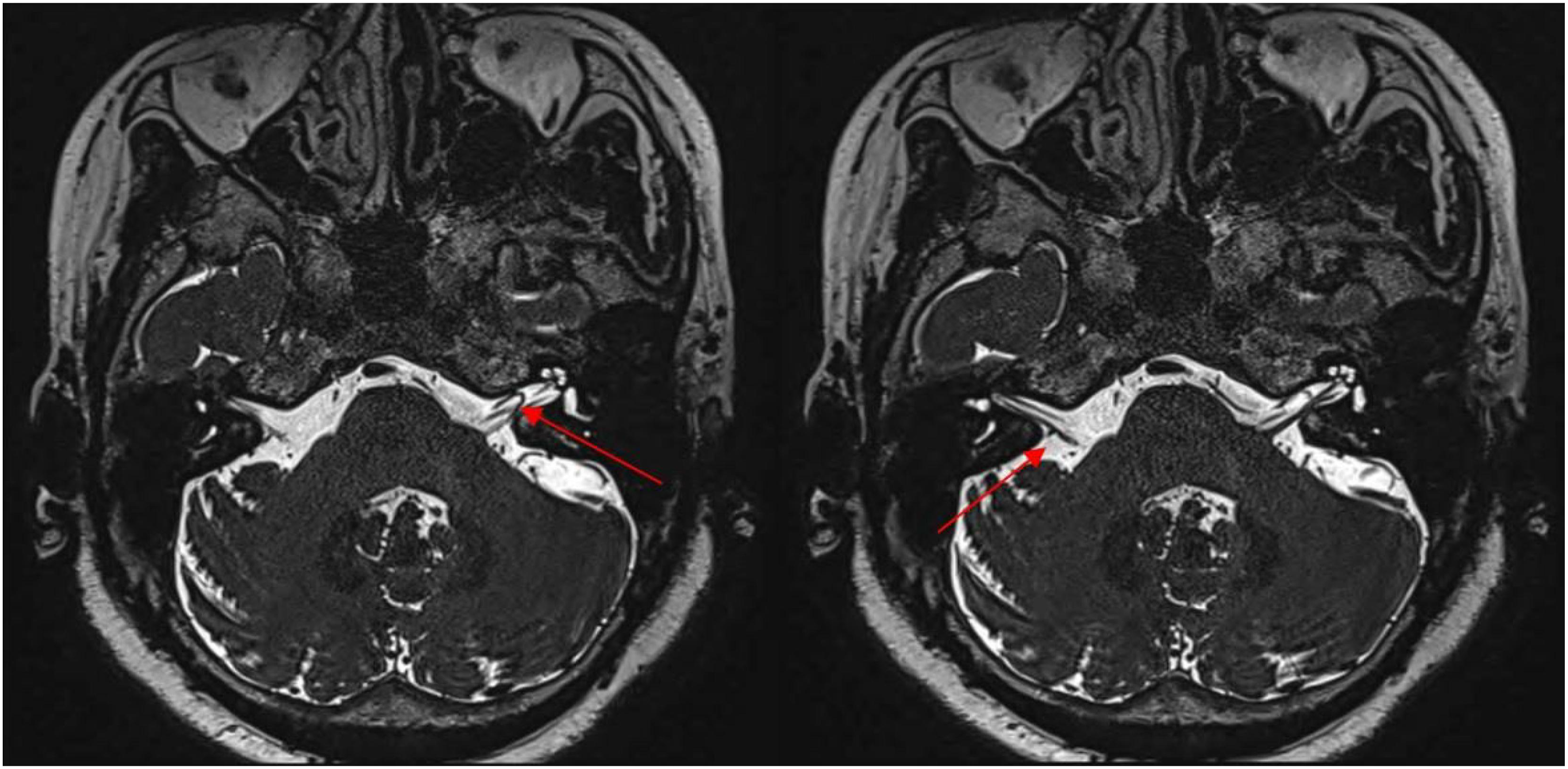
Under the guidance of intraoperative brainstem auditory evoked potentials and facial electromyography monitoring, a post-auricular, lazy-S skin incision was made, and the bone flap (approximately 3 cm in diameter) was subsequently removed using a high-speed drill. The dura was then opened using a C-shaped incision, and the arachnoid membrane was dissected gently and sharply to expose the cranial nerve VII–VIII complex. The offending vessel, AICA, was identified adjacent to the internal acoustic meatus, attaching to the superior vestibular nerve. The AICA was then carefully detached from the cranial nerve VIII (most likely the superior vestibular nerve) and re-attached to the dura tentorium using a fibrin-sealant patch to prevent compression (Figure 3). Thereafter, the dura mater was closed using a watertight seal. (Left) The 30˚ endoscopic view shows that the region of conflict between the anterior inferior cerebellar artery (AICA) (black arrowhead) and cranial nerve VII–VIII complex (superior vestibular nerve most likely, black arrow) is found near the entry site of internal acoustic canal. (Right) TACHOSIL® (black arrow) is applied between the offending vessel and dura tentorium to prevent compression.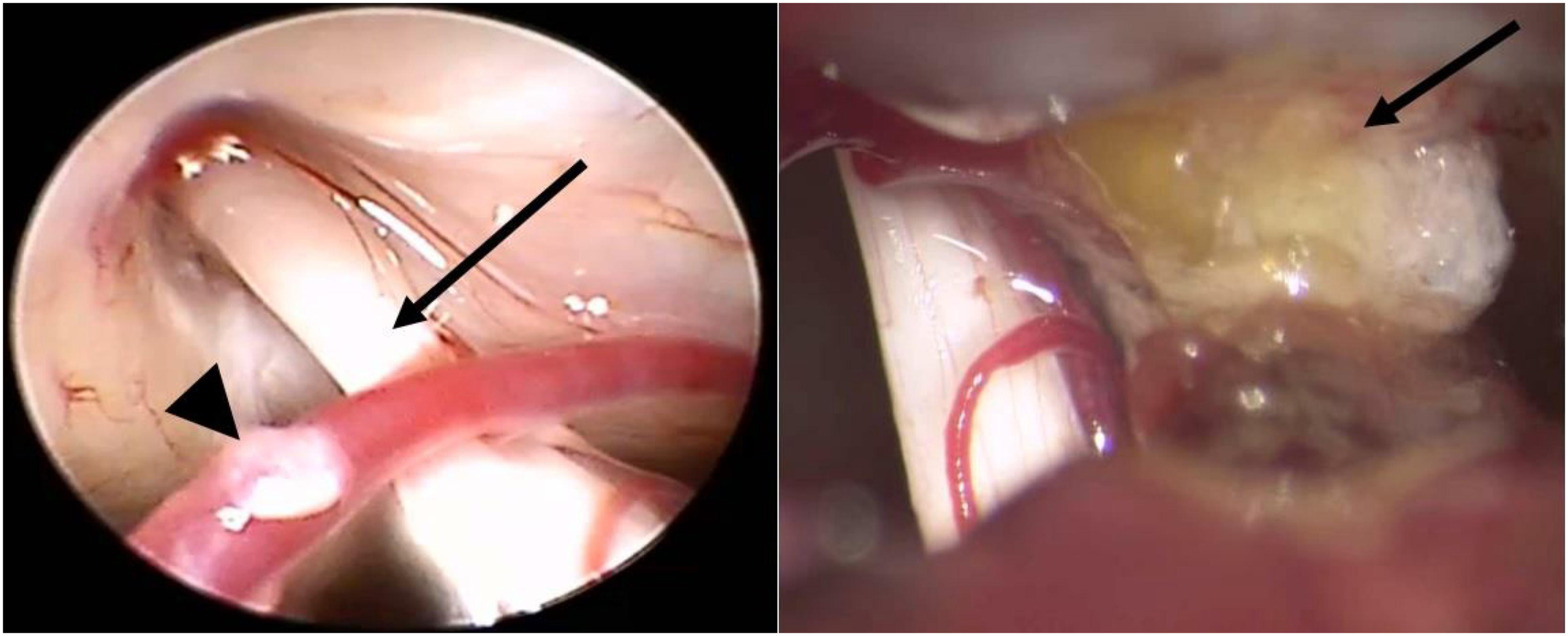
Postoperatively, the patient reported immediate symptomatic relief, and no postoperative complications were observed. The postoperative audiogram showed no significant differences in hearing thresholds relative to the preoperative audiogram. Moreover, the postoperative THI score was 0, indicating complete symptom relief. Notably, VEMPs at 6 months postoperatively showed significant changes, including the appearance of responses to oVEMP and increased response amplitudes on cVEMP (Figures 2C, 2D). On a 1-year follow-up, the patient reported no related symptoms or recurrence.
Discussion
In 2007, Ridder et al proposed diagnostic criteria for CVCS as follows: (1) unilateral paroxysmal tinnitus; (2) co-existence of ipsilateral symptoms (hemifacial spasms, otalgia, vertiginous spells, and hearing loss at tinnitus frequency); (3) positive MRI findings indicative of vascular contact; and (4) positive auditory brain response potential. 6 In this case, the patient complained of unilateral paroxysmal tinnitus with frequent onset of drop attack. Moreover, the patient’s MRI findings showed vascular compression on both sides of the eighth cranial nerve, fulfilling most of the proposed criteria, implicating CVCS as the most likely cause for the patient’s chief complaints. In such cases wherein abnormal imaging findings are detected in a patient who is refractory to medication, surgical exploration of the affected site is recommended. 4 In this report, we successfully identified the region of contact, which allowed us to detach the offending vessel from the nerve, adding further evidence to previous findings that symptoms are dramatically resolved immediately after decompression surgery. Furthermore, it implies that MVD is an effective treatment option for CVCS symptoms.
To the best of our knowledge, this is the first report to present MVD as a definitive treatment for drop attacks secondary to CVCS. Although CVCS is mainly known to cause vertigo, tinnitus, and hearing disturbances, this report suggests the possibility of contact between the AICA and cranial nerve VIII when a patient complains of recurrent drop attacks with concomitant tinnitus. A widely accepted mechanism of drop attack is the sudden stimulation of the otolith organs, affecting the vestibulospinal pathways, consequently resulting in falls. 7 In this case, we hypothesize that the offending vessels induced mechanical stimuli to the vestibular nerve, resulting in the patient’s recurrent drop attacks. More importantly, since drop attacks are often associated with Meniere’s disease and delayed endolymphatic hydrops, other possible diagnoses must be ruled out first. Furthermore, if the patient is refractory to medications, MRI should be recommended to determine if the region of contact is cited, with consideration to the possibility of CVCS-induced drop attacks.
However, it should be noted that careful consideration is important before deciding on surgical treatment. Although the MR findings of our patient demonstrated contact between the AICA and cranial nerve VIII, relying solely on imaging for clinical decision-making is not recommended. In a previous analysis of patients with vascular contact of the cranial nerve VIII on MRI, approximately 21.4% were asymptomatic, whereas only 25% were symptomatic. 8 Therefore, vestibular function tests (in our case, cVEMPs and oVEMPs) and specific symptoms that correlate with CVCS, such as response to anticonvulsants, should be considered actively. In addition, Moller et al reported that 14 of 129 patients who underwent successful MVD had recurrence after one year. 9 Therefore, long-term follow-up is required to detect recurrence and determine the success of MVD.
Conclusion
This case report depicts the successful management of CVCS with MVD of the eighth cranial nerve. During long-term follow-up, the patient remained stable without recurrence of symptoms. Since the results of MVD of the eighth cranial nerve vary among studies, careful examination and exclusion of other causes of CVCS are important for definite diagnosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the National Research Foundation of Korea (NRF).