
Abstract
Background:
To summarize the therapeutic effect of aspiration combined with magnet compression in the treatment of auricular pseudocyst and to explore a simple and effective treatment regimen for auricular pseudocyst.
Methods:
The clinical data of 45 patients with auricular pseudocysts treated in the outpatient department from March 2019 to May 2021 were retrospectively analyzed. Treatment outcomes were categorized into cure, excellence, and invalid to evaluate the therapeutic effect. The visual analog scale (VAS) was used to assess patients’ satisfaction with the treatment.
Results:
After treatment with aspiration combined with magnet compression, 31 cases (68.9%) were cured, 8 cases (17.8%) demonstrated excellence, and 6 cases were invalid. The VAS score ranged from 2 to 8 points with a mean value of 7.3 points.
Conclusions:
The treatment that aspiration combined with magnet compression shows significant advantages. It can be considered as the first choice for patients with good local skin conditions during their initial visit, especially in primary hospitals lacking surgical facilities or where access to medical care is difficult.
Keywords
Introduction
Auricular pseudocyst refers to a cystic protrusion formed by non-purulent, serous exudation within the cartilage lamella of the auricle. It is termed a pseudocyst because it lacks the characteristic epithelial structure of a true cyst wall. 1 The cystic fluid originates from the perichondrium of the anterior part of the auricle. The treatment strategy aims to eliminate the production of perichondrial cystic fluid through surgery or drugs.2,3 At present, the main treatment methods include perichondrial resection, 4 local injection of medication at the lesion site, 5 or local compression followed by puncture and aspiration.6,7 Literature reports that materials used for compression include plaster, silicone sheets, and iodoform gauze strips. In our department, we commonly use magnets. Long-term clinical treatment has found that magnet compression has the advantages of simple operation, low cost, and good therapeutic effect. This paper reports the clinical characteristics and treatment outcomes of 45 patients with auricular pseudocysts treated with puncture and aspiration combined with magnet compression.
Patients and Methods
General Data
We retrospectively analyzed the clinical data of 62 patients with auricular pseudocysts treated in the Department of Otolaryngology of Xijing Hospital from March 2019 to May 2021. Among these, 45 cases had complete clinical data (with a loss to follow-up rate of 27.4%). Inclusion criteria are as follows: (1) diagnosed with auricular pseudocyst, (2) treatment-naive patients receiving puncture and aspiration combined with magnet compression therapy, and (3) complete baseline/follow-up data. Exclusion criteria are as follows: (1) concurrent infection, (2) prior auricular interventions, and (3) combined with auricular malignancy or uncontrolled systemic disease. This study was approved by the Medical Ethics Committee of the First Affiliated Hospital of the Air Force Medical University (no KY20222123-C-1). Informed consent was obtained from the patients enrolled in the study.
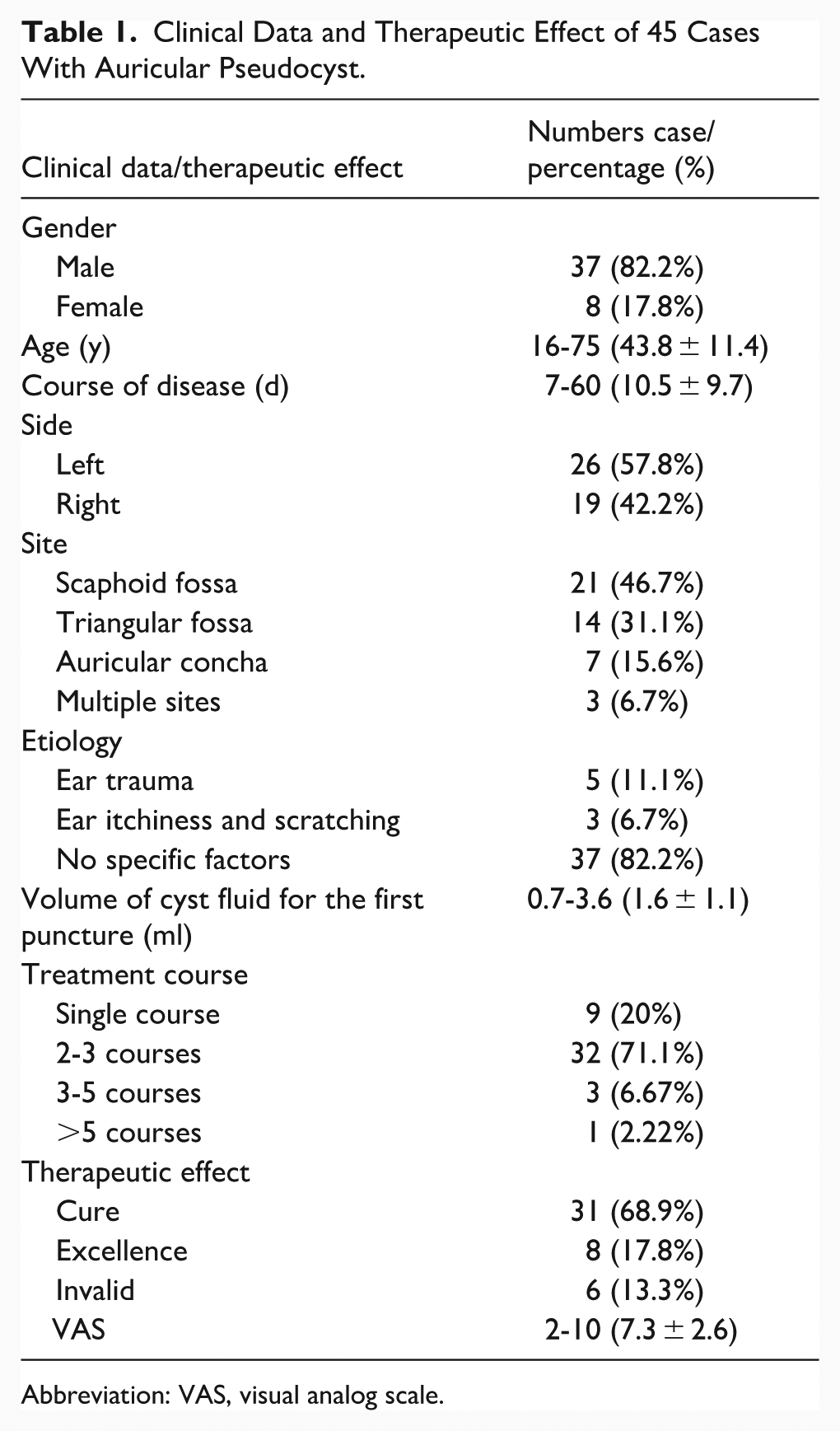
There were 37 males (82.2%) and 8 females (17.8%), with an age range of 16 to 75 years and an average age of 43.8 years. The course of the disease ranged from 7 to 60 days, with an average of 10.5 ± 9.7 days. Forty-five patients had unilateral auricular pseudocyst, with 26 cases (57.8%) on the left ear and 19 cases (42.2%) on the right ear. The lesions were mainly distributed in the scaphoid fossa in 21 cases (46.7%), the triangular fossa in 14 cases (31.1%), and the concha cavity in 7 cases (15.6%), with 3 cases (6.7%) involving the above 3 regions. The etiology was unknown in 37 cases (82.2%), trauma in 5 cases (11.1%), and repeated ear rubbing in 3 cases (6.7%).
Treatment Methods
The patient was seated upright. After routine disinfection, a puncture was performed at the lowest point of the cyst to aspirate the cystic fluid. After routine disinfection, a puncture was performed at the lowest point of the cyst to aspirate the cystic fluid. The cyst wall was simultaneously compressed with fingers to expel as much fluid as possible. After the aspiration procedure, sustained manual compression was applied for 15 minutes. After the cyst had completely disappeared, a thin, flat magnet of appropriate size and thickness was selected and placed on the front and back of the auricle where the cyst was (a double layer of small gauze was placed under the magnet to prevent pressure sores) to achieve local compression. The magnet used was a common, round, and flat piece, with no specific requirements for the manufacturer. The diameters of the magnets ranged from 0.7 to 1.5 cm, the thicknesses ranged from 0.1 to 0.15 cm, and the weights ranged from 0.3 to 1.5 g, selected flexibly according to the size of the cyst and the thickness of the auricle. After magnet compression, the patient was observed for another 15 minutes to make sure that there was no obvious re-expansion of the cyst, obvious pain, discomfort, or poor blood circulation of the auricle happened to the patient. If there was no obvious re-expansion of the cyst, obvious pain, discomfort, or poor blood circulation of the auricle, and the patient could tolerate the pain, the magnet was fixed with a thin layer of gauze and tape to prevent falling off. The patients had to return to our outpatient clinic for re-examine after 48 hours. If obvious pain in the auricle or noticeable cyanosis of the skin compared to the contralateral ear occurred within 48 hours, the patient was advised to remove the compressing magnet and go to see a doctor immediately. The specific operations can be seen in Figure 1. The magnet was removed when the cyst had completely resolved at follow-up. If there was still a residual cyst, the same method was applied again.
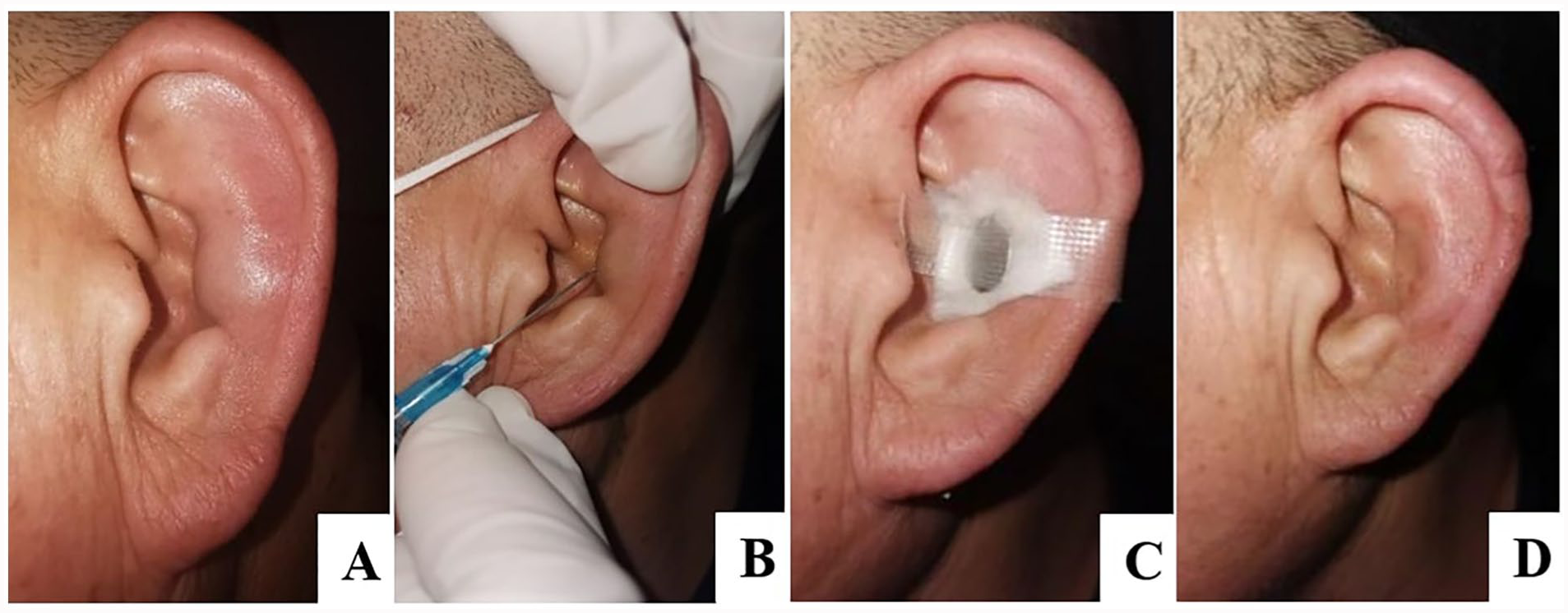
(A) Clinical presentation of the left auricular pseudocyst. (B) Aseptic puncture and aspiration of cystic fluid. (C) Magnet pressurization. (D) Post-treatment appearance at 48 hours.
Evaluation of Therapeutic Effects
Therapeutic effects were evaluated after 6 months of follow-up, which was classified into 3 groups based on the previous literature: cure, excellence, and invalid.1,8 Cure: the cyst completely disappears, and there was no difference with the contralateral side in shape, skin, and thickness. Excellence: the auricle having a shape similar to the contralateral side, but with local thickening at the original cyst site and pigmentation of the skin. Invalid: the cyst has not disappeared or has recurred during the treatment period. The visual analog scale (VAS) was used to assess patient satisfaction with treatment outcomes, with scores ranging from 0 to 10, where higher scores indicate greater satisfaction.
Results
Among the 45 patients treated with cyst puncture and aspiration combined with magnet compression, 31 cases (68.9%) were cured, 8 cases (17.8%) demonstrated excellence, and 6 cases (13.3%) were invalid. The volume of cyst fluid aspirated during the first puncture ranged from ~0.7 to 3.6 ml. Nine patients (20.0%) were cured after a single treatment course within 48 hours. Thirty-two patients (71.1%) demonstrated cure or excellence following 2 to 3 treatment courses. These cases predominantly involved lesions located in the scaphoid fossa or triangular fossa. Three elderly male patients (6.7%) necessitated 3 to 5 treatment courses for cure or excellence, with lesions extending across multiple sites of the auricular cartilage. A patient who had been treated more than 5 times but still failed was subsequently treated with surgery. During the 6-month follow-up after treatment, 6 cases recurred, with 5 cases recurring within 2 weeks after treatment and 1 case recurring 4 months after treatment. The VAS scores after treatment ranged from 2 to 10, with an average of 7.3 points (Table 1).
Clinical Data and Therapeutic Effect of 45 Cases With Auricular Pseudocyst.
Abbreviation: VAS, visual analog scale.
Discussion
Auricular pseudocyst occurs predominantly in males aged 20 to 50 years, with unilateral involvement observed more frequently, while bilateral involvement is relatively rarely reported in the literature. 9 The lesion is often located on the anterior part of the auricle, such as the concha and triangular fossa. Clinically, it usually presents as a painless swelling, but a small number of patients may experience pain and redness. 10 The etiology of auricular pseudocyst is mostly unknown. It is currently believed that local trauma to the auricle, congenital embryonic developmental abnormalities, and immune factors may lead to local microcirculatory disturbances, resulting in increased reactive exudate between the cartilages.11,12 This exudate accumulates in the tissues and eventually forms a cystic lesion. Men often exercise, wear helmets, and fight, which may be the reasons why men are more susceptible to this condition. 2 The 45 patients retrospectively analyzed in this study generally conformed to the aforementioned clinical characteristics, as evidenced by unilateral auricular involvement observed in all cases and no significant lateralization of incidence between ears. There were 3 male patients over 60 years old. After asking them about their sleeping habits carefully, it was found that they preferred to sleep on the same side, which may reduce the flexibility of the auricles. Repeated compression leads to increased local exudate.
Treatments for auricular pseudocyst mainly include surgical and non-surgical treatment procedures. Surgery is effective and has a low recurrence rate, but cartilage and newly formed cartilage need to be resected in the operation, which can cause serious local inflammatory reactions, and patients suffer postoperative pain. Postoperative complications such as auricular perichondritis and auricular deformity may occur, especially in patients with a tendency to form keloids, who have a higher risk of keloid formation in the auricle. Furthermore, there is no significant difference in recurrence prevention between surgery and conservative treatment. Postoperative measures such as compression dressing and drainage are still required.13,14 Some studies have compared the treatment satisfaction between surgical and nonsurgical patients and found that surgical patients had lower satisfaction. 1 Therefore, clinicians tend to choose nonsurgical treatment for patients who visit for the first time, have high compliance, and have small cyst volumes.
Nonsurgical treatment has the advantages of being simple, economical, and having a low incidence of auricular infection and deformity. Simple aspiration of cyst fluid alone is inevitably prone to recurrence. Therefore, local compression after aspiration is crucial. Plaster was commonly used for fixation in the early days, but it has the disadvantages of being heavy and making it difficult to observe local blood circulation. Some studies report that oral silicone mold has been used to achieve precise compression, but this material is relatively expensive. 3 In addition to avoiding the shortcomings of the above materials, the pulsed electromagnetic field of magnetic stones can significantly increase collagen fibers, thereby promoting wound healing.15,16 With various diameters and thicknesses, magnetic stones can be flexibly selected according to the size and location of the cyst to cover the cyst area as completely as possible. If local pain or skin color changes occur due to poor blood circulation during treatment, doctors can detect it in time, and the magnetic stones can be removed or replaced with thinner ones. Even if the magnetic stone falls off, the patient can reposition it in time. In our study, all 45 patients included were treated for the first time, with little cyst fluid aspirated. Therefore, the VAS score after treatment was higher than the VAS score (4.3) reported by Yu et al 1 for patients treated with gauze and bandage compression. We find that the effect of magnetic compression is closely related to the location of the lesion and the local skin condition. This therapeutic method has obvious advantages for patients with lesions in thin skin and single sub-regions, who can be cured after 1 to 2 treatments. On the contrary, this treatment method has poor therapeutic effects for patients with thick local skin, multiple sub-regions, and much initial cyst fluid, so patients need to be treated several times. In addition, the treatment effect in young and middle-aged patients is significantly better than that in elderly patients.
Conclusion
In conclusion, magnetic compression treatment for the auricular pseudocyst has obvious advantages and can be considered the first choice for patients who visit for the first time and have good local skin conditions, especially in primary hospitals without surgical conditions or where medical care is difficult. This study supplements and expands the clinical experience of the treatment that aspiration combined with magnetic compression in the treatment of auricular pseudocyst. However, the limitation of our study is that it is a retrospective, single-center study with a relatively limited treatment method and no comparison with multiple treatment options.
Footnotes
Acknowledgements
The authors acknowledge the patient for his cooperation.
Ethical Considerations
All procedures in this study were conducted in accordance with the Medical Ethics Committee of the First Affiliated Hospital of the Air Force Medical University (no KY20222123-C-1) approved protocols.
Consent for Publication
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Author Contributions
Yubin Lai and Xingchen He contributed equally with shared co-first authorship. All authors have read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Innovation team of Shaanxi Province (no 2023-CX-TD-70).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data included in this study are available upon request by contacting the corresponding authors.