
Abstract
Objective:
To evaluate the clinical use of pentoxifylline and tocopherol (PENTO), with or without clodronate (PENTOCLO), in the treatment and prevention of osteoradionecrosis (ORN) and medication-related osteonecrosis of the jaw (MRONJ).
Methods:
A literature review was conducted using PubMed from database inception to May 2025. Studies were included if they evaluated PENTO or PENTOCLO for the treatment or prevention of ORN or MRONJ. Only human studies with full-text availability were included. Data extracted included patient population, intervention details, duration, co-interventions, outcomes, and adverse events.
Results:
Twenty-two studies met inclusion criteria, comprising randomized trials, prospective cohorts, and retrospective case series. In ORN treatment, PENTO/PENTOCLO achieved complete healing in 54% to 100% of patients, with improved symptoms and reduced need for surgery. The addition of clodronate (PENTOCLO) showed mixed results, with 1 large cohort suggesting no additional benefit over PENTO alone. PENTO prophylaxis before dental extractions in irradiated patients resulted in low ORN incidence (0%-5%). In MRONJ, PENTO improved pain, radiographic healing, and mucosal coverage; the only RCT showed significantly-lower relapse rates after surgery with adjunctive PENTO. Across all studies, adverse effects were minimal.
Conclusion:
PENTO is an effective and well-tolerated therapy for ORN and MRONJ, with emerging evidence supporting its use in prevention protocols. While PENTOCLO may benefit select ORN cases, further trials are needed to define optimal regimens. PENTO offers a noninvasive, accessible alternative to surgery and hyperbaric oxygen therapy.
Keywords
Introduction
Radiation therapy (RT) is a mainstay of treatment for head and neck cancer. Osteoradionecrosis (ORN) is a morbid complication of RT, which occurs in the mandible of around 2% of patients with head and neck cancer. 1 ORN can occur in other areas along the skull base including the maxilla, temporal bone, and sphenoid.2,3 ORN of the mandible is most common, likely due to the vulnerability of the blood supply and its frequent inclusion in the radiation field.1,4 ORN may occur spontaneously or more commonly secondary to postradiation injury or trauma. 1 The incidence of ORN after dental extraction in an irradiated patient is between 2% and 18%. 5
Our understanding of the pathophysiology of radiation damage has been evolving. Initially, the fibrosis and atrophy was thought to be driven by relative tissue hypoxia.4,6 Today, the theory of radiation-induced fibroatrophy (RIF) focuses on the role of reactive oxygen species in fibroblast signaling and proliferation. 6 There are 3 described phases of RIF: the pre-fibrotic phase marked by inflammatory destruction of endothelial cell barriers, the constitutive organized phase of fibroblast proliferation, and the late fibroatrophic phase resulting in progressive sclerosis. 6
Conservative treatment of ORN focuses on lifestyle factors such as oral hygiene and cessation of tobacco and alcohol use. 7 Antimicrobials and corticosteroids are used to decrease the risk of osteomyelitis of necrotic bone.7,8 To promote wound healing and limit hypoxic injury, hyperbaric oxygen therapy (HBOT) has been used as an adjunct treatment of ORN.7,9 However, further studies have failed to demonstrate significantly-improved outcomes. 10 Surgical management of ORN ranges from sequestrectomy to major reconstructive procedures. 5
The most promising medical treatment regimen in recent years is known as the pentoxifylline + tocopherol + clodronate (PENTOCLO) protocol. This triple therapy was initially trialed for the treatment of ORN in 2002. 11 Pentoxifylline (PTX) is a derivative of methylxanthine, which decreases inflammatory response, inhibits fibroblast proliferation, increases red blood cell flexibility, and vasodilates. 6 Tocopherol or vitamin E is an antioxidant, which scavenges free radicals and inhibits TGF-β1. 6 Clodronate is a non-aminobisphosphonate, which inhibits osteoclast activity at a lower potency than other bisphosphonates and simultaneously increases osteoblast activity. Clodronate has a reduced risk of medication-related osteonecrosis of the jaw (MRONJ) as compared to other bisphosphonates. These unique properties may contribute to bone protection at the doses used for treatment of ORN.12,32
Materials and Methods
A comprehensive literature search was performed in PubMed from database inception through May 1, 2025, by 2 reviewers individually. The search query used combined terms for ORN, MRONJ, and the interventions of interest, including PTX, tocopherol, vitamin E, and clodronate. After an initial search, relevant articles were included or excluded by screening titles and abstracts. Citation searching was also performed on the articles initially found.
We limited results to human studies including clinical trials, cohort and case-control studies, case series, case reports, and retrospective studies. We excluded animal or in vitro studies, editorials/commentaries, systematic reviews, and meeting abstracts without full-text data. No language restrictions were applied initially, but studies needed to have full-text available in English.
Data were extracted by both reviewers using a standardized form capturing: study design, population (including indication: ORN vs ORN prophylaxis vs MRONJ, site of jaw involved, radiation dose, or antiresorptive therapy details), intervention details (dosing and schedule of PENTOCLO, duration of therapy, co-interventions (such as antibiotics, HBOT, or surgery), outcome measures, key quantitative results, and authors’ notable comments. We summarized the data in tables (Tables 1–5).
Treatment of RIF Without Bone Involvement.
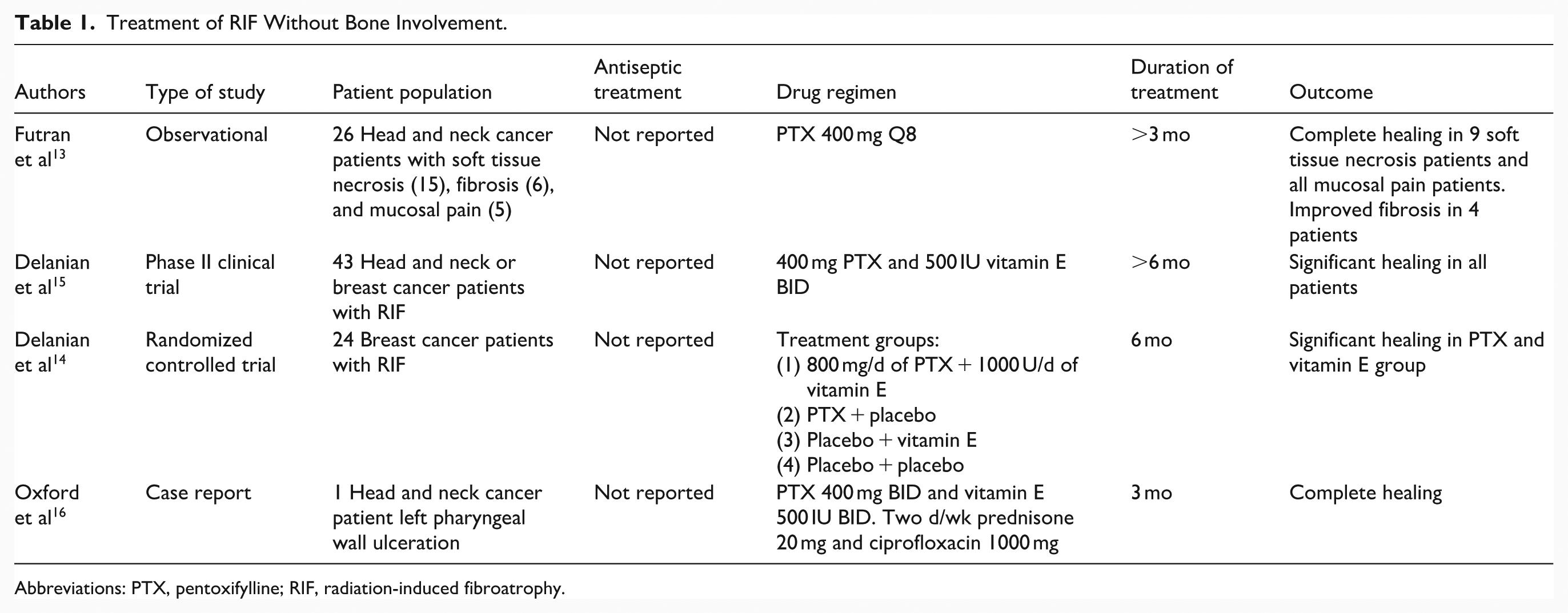
Abbreviations: PTX, pentoxifylline; RIF, radiation-induced fibroatrophy.
Treatment of Osteoradionecrosis.
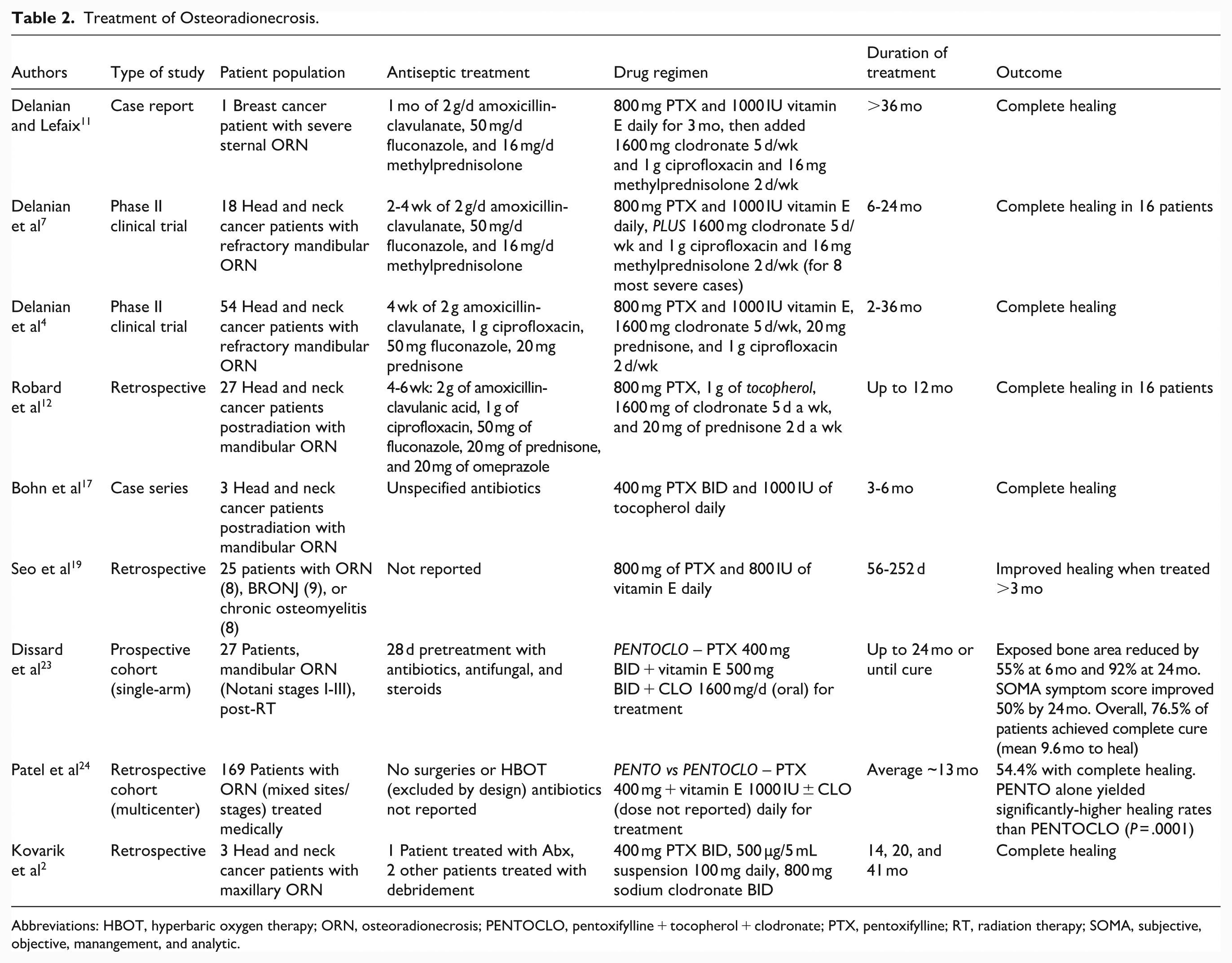
Abbreviations: HBOT, hyperbaric oxygen therapy; ORN, osteoradionecrosis; PENTOCLO, pentoxifylline + tocopherol + clodronate; PTX, pentoxifylline; RT, radiation therapy; SOMA, subjective, objective, manangement, and analytic.
Treatment of MRONJ.
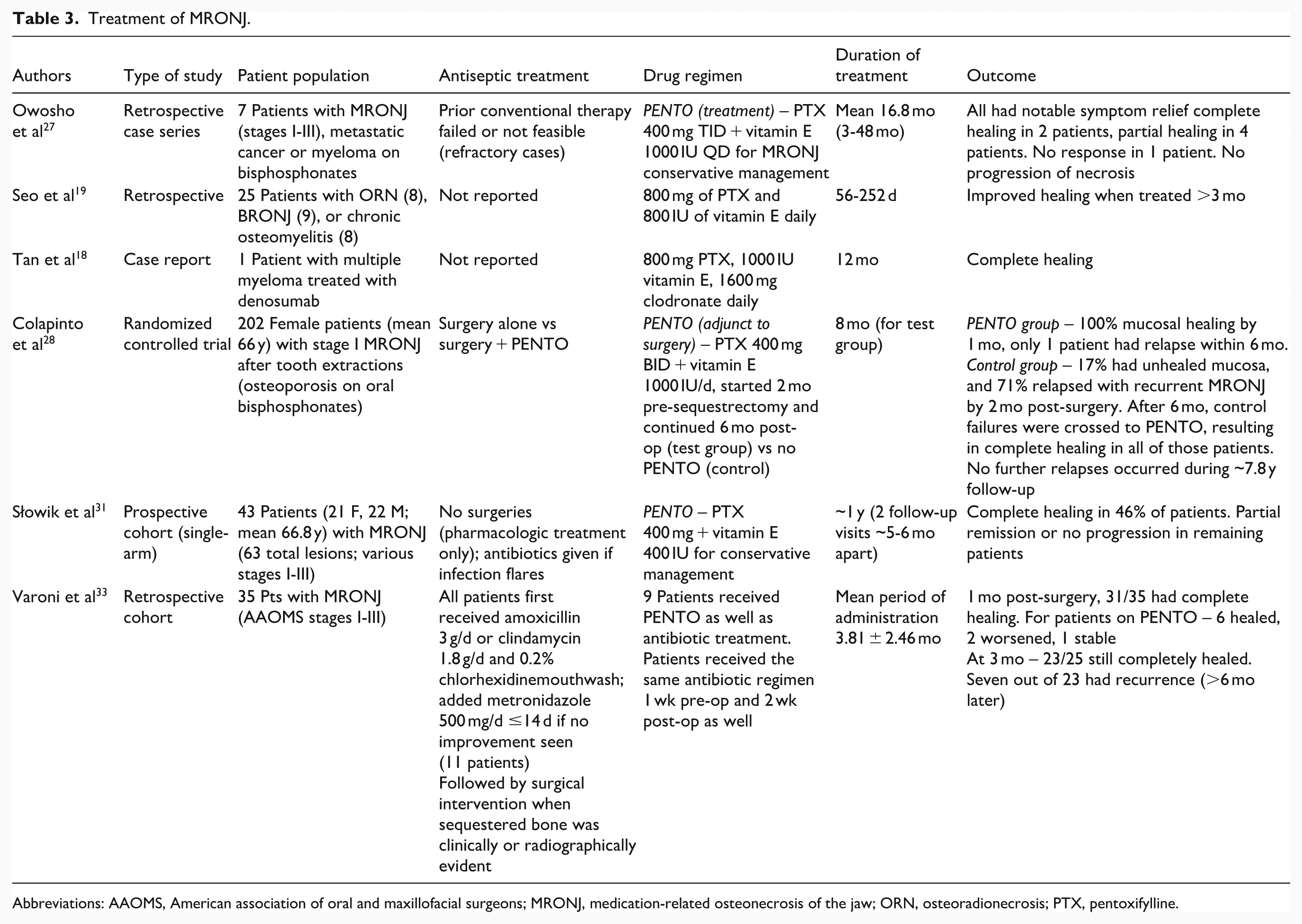
Abbreviations: AAOMS, American association of oral and maxillofacial surgeons; MRONJ, medication-related osteonecrosis of the jaw; ORN, osteoradionecrosis; PTX, pentoxifylline.
PENTO as Prophylactic Treatment.
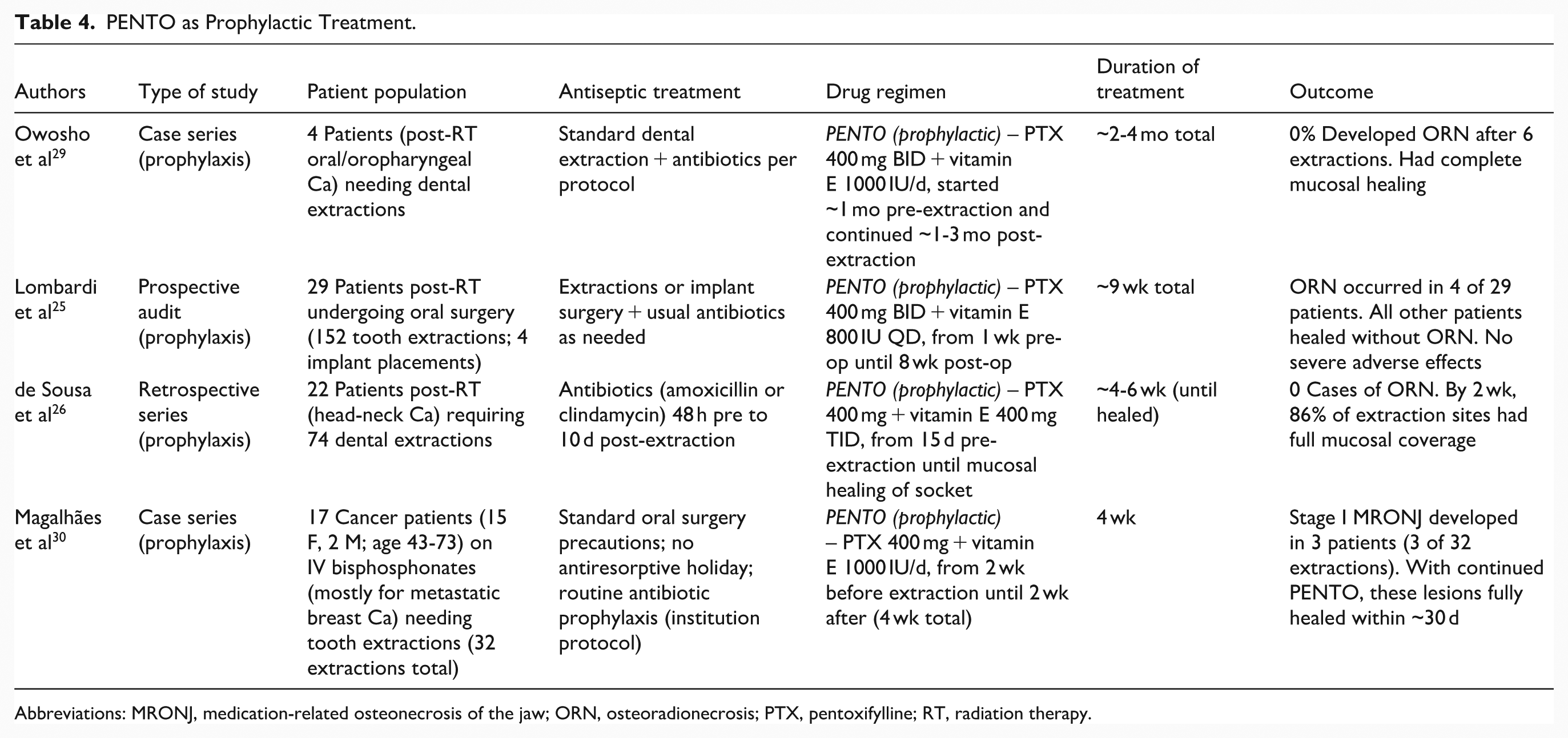
Abbreviations: MRONJ, medication-related osteonecrosis of the jaw; ORN, osteoradionecrosis; PTX, pentoxifylline; RT, radiation therapy.
Recommended PENTOCLO Protocol.
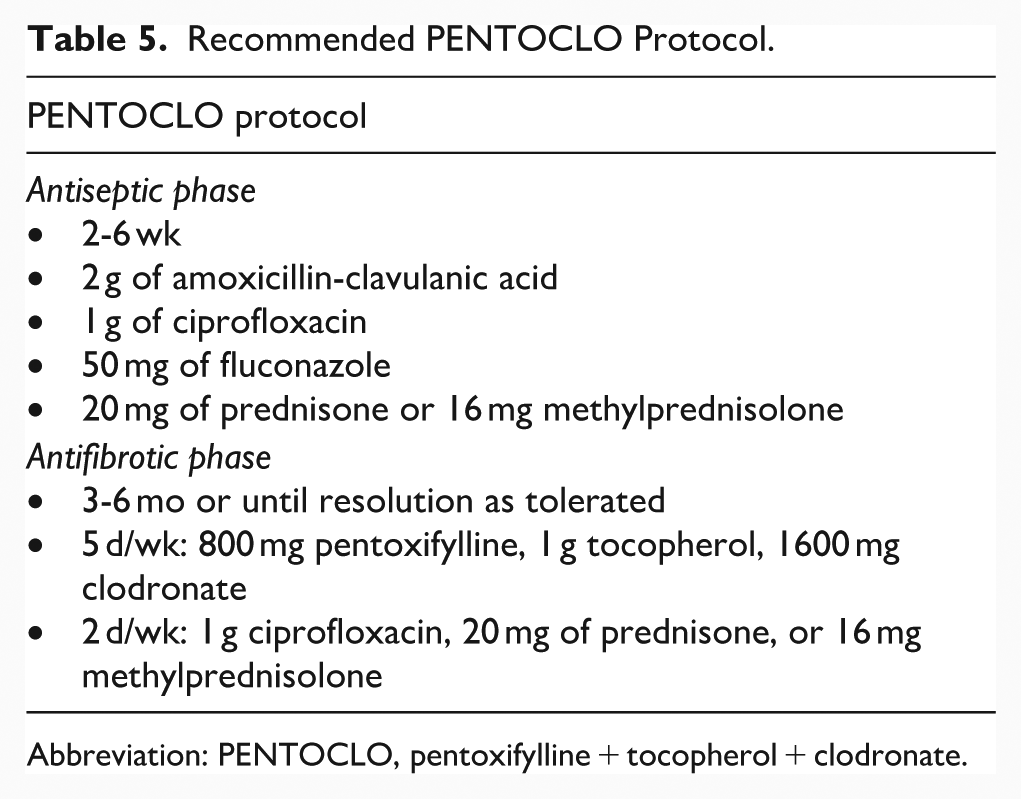
Abbreviation: PENTOCLO, pentoxifylline + tocopherol + clodronate.
Results
Study Selection
A total of 22 studies met inclusion criteria from the reviewers’ combined searches. The included studies are summarized in Tables 1 to 4.
Study Characteristics
ORN Treatment Studies
Several studies evaluated PENTO with or without clodronate in patients with established ORN of the jaw. The largest early study was a Phase II trial by Delanian et al, who treated 54 patients with refractory mandibular ORN using prolonged PENTOCLO therapy. The patients had advanced, nonhealing ORN (Notani stages II-III) and had failed prior conventional treatments. 4 Another French group’s retrospective series by Robard et al examined 27 ORN patients treated with PENTOCLO. 12 More recently, a prospective single-arm study by Dissard et al in France enrolled 27 ORN patients on PENTOCLO with serial outcome measurements. 23 In the UK, Patel et al reported on 169 ORN cases managed with PENTO or PENTOCLO (retrospective multicenter data). 24
These ORN treatment studies predominantly included patients with a history of high-dose radiation for head and neck cancer (mostly oral cavity or oropharyngeal tumors). Mandibular ORN was the most common site, and many cases were advanced (with exposed bone, chronic ulceration, and in some cases pathologic fracture). Interventions varied slightly: All studies used PTX (400 mg taken 2-3 times daily) plus tocopherol (typically 400-500 mg taken 2-3 times daily, ie, total 800-1000 IU/day). Clodronate (1600 mg/day) was included in the regimen in Delanian et al, Robard et al, Dissard et al 2020, and Patel et al (some patients), but not in others. Treatment durations ranged from about 3 to 6 months in the smallest series up to 24 months in the prospective study. Many protocols continued therapy until clinical healing was achieved or for a maximum set duration. Co-interventions commonly included an initial course of antibiotics (and sometimes corticosteroids) prior to starting PENTO/PENTOCLO. Notably, in Patel et al’s series, any patients who received concurrent surgical resection or HBOT were excluded to isolate the effect of medical management.
ORN Prophylaxis Studies
Three smaller studies investigated the preventive use of PENTO in patients who had received head and neck radiotherapy and were undergoing dental extractions. Owosho et al reported an initial case series of 4 such patients who received prophylactic PENTO for several weeks before extraction. 29 Lombardi et al conducted a clinical audit including 29 irradiated patients who underwent 75 oral surgical procedures under a PENTO prophylaxis protocol. 25 A Brazilian study by de Sousa et al included 22 post-RT patients (74 extractions) managed with a standardized PENTO prophylaxis regimen. 26 All prophylaxis studies used PTX 400 mg twice daily plus tocopherol (400-800 IU daily) initiated 1 to 2 weeks before the dental extraction and continued for 2 to 8 weeks. All patients received antibiotics per standard oral surgery protocols. These studies assessed outcomes including the incidence of ORN, mucosal healing, and postoperative complications. We also included 1 study on MRONJ prevention: the case series by Magalhães et al, which used prophylactic PENTO around tooth extractions in 17 cancer patients receiving IV bone-modifying agents. 30
MRONJ Management Studies
We included multiple reports on the use of PENTO in patients with established MRONJ. Owosho et al presented an initial series of 7 cancer patients with refractory MRONJ treated with PENTO as a conservative therapy. 27 A high-quality randomized trial was recently published by Colapinto et al, focusing on stage I MRONJ patients who underwent sequestrectomy with or without adjunctive PENTO. 28 Additionally, Słowik et al reported a prospective observational study of 43 MRONJ patients treated with PENTO without surgery. 31
The MRONJ studies cover a range of patient populations: The Owosho et al and Słowik et al studies included patients with various cancers (breast, myeloma, prostate, etc) on bisphosphonates or denosumab, often with advanced MRONJ. By contrast, Colapinto et al’s randomized controlled trial (RCT) focused on a relatively-homogeneous subset: women with osteoporosis on long-term oral bisphosphonates who developed stage I MRONJ after extractions. Interventions in MRONJ studies were generally PTX 400 mg (2-3 times daily) plus tocopherol 800 to 1000 IU daily. Clodronate was not used in any MRONJ study (adding a bisphosphonate would be counter-intuitive in bisphosphonate-related osteonecrosis of the jaw). Duration of therapy was often 6 to 18 months. In the RCT, PENTO was given for 8 months total around the time of surgery. Some MRONJ patients had minor operative interventions (eg, sequestrectomy or extensive debridement), while others were managed nonsurgically. Outcomes assessed included complete mucosal healing, improvements in pain/infection, radiographic bone fill, relapse of MRONJ, and need for subsequent surgery.
Risk of Bias
The overall quality of evidence is moderate to low. The single RCT (Colapinto et al) had a robust design with clearly-defined outcomes, but it was unblinded and only included stage I MRONJ patients, limiting generalizability. The cohort and case series studies mostly lack control groups and have potential selection bias. Many ORN studies were retrospective and relied on clinical endpoints without blinded assessment. According to Newcastle-Ottawa Scale, most cohort/series had fair quality (some concerns in selection and outcome assessment domains). Despite these limitations, consistency of results across independent studies lends support to certain findings, as discussed below.
Comparative Outcomes
Efficacy in ORN Treatment
The included evidence suggests that the combination of PENTO (with or without clodronate) can achieve meaningful healing in a substantial proportion of ORN patients. In the pivotal Phase II trial by Delanian et al, long-term PENTOCLO therapy led to complete restoration of the mandible in all 54 patients, including mucosal closure and radiographic bone regeneration (with no remaining sequestra). 4 These patients had “refractory” ORN, having failed previous standard therapies, so a 100% healing rate was remarkable. A later retrospective study by Robard et al reported complete mucosal healing in 59% of their ORN cases after PENTOCLO, with clinical improvements in most others. The median time to healing in Robard et al’s series was ~82 days (range 1-9 months), and healing tended to occur faster in patients who had ORN precipitated by surgery (49 days) than in those who had received concomitant chemoradiation (169 days).
The prospective cohort by Dissard et al reinforces these positive outcomes. They observed progressive reduction in exposed bone area over time on PENTOCLO, with 76.5% of patients achieving complete healing by around 10 months of therapy. 23 Importantly, no ORN progression was seen in the remaining patients. Symptomatic relief was also documented: Dissard et al noted continuous improvements in the SOMA scores (measuring pain, trismus, dysphagia, etc) by 50% at 2 years. Delanian et al’s trial similarly reported significant pain reduction and improved mouth opening. 4
Collectively, these studies indicate that PENTO/PENTOCLO therapy can lead to complete ORN resolution in roughly 55% to 100% of patients, depending on disease severity and duration of therapy.
Avoidance of Surgery
One major goal in ORN management is to avoid radical mandibular resection. The need for mandibular resection was markedly reduced in patients on PENTO/PENTOCLO. Robard et al noted that their protocol “reduced indications for major surgery.” In Dissard et al’s cohort, none of the patients who responded to PENTOCLO required rescue surgery, implying a potential to spare patients from surgical morbidity. Patel et al’s study explicitly showed that even when complete healing was not attained, PENTO/PENTOCLO often stabilized the condition, converting an acute surgical problem into a chronic manageable condition.
Comparison of PENTO Versus PENTOCLO
A salient question is whether adding clodronate improves outcomes over PENTO alone. Clodronate is a non-nitrogenous bisphosphonate thought to have an osteoclast-modulating effect and was hypothesized to assist in bone remodeling in ORN. However, Patel et al provides the largest comparative insight: in their 169-patient series, PENTO alone was significantly more effective than PENTOCLO in achieving ORN healing (54% overall healing, with P = .0001 favoring PENTO). Given that clodronate can cause gastrointestinal side effects and adherence issues, some clinicians might opt for PENTO alone unless future studies show a clear benefit to adding clodronate.
Predictors of Response in ORN
Certain subgroups appeared to respond differently. Patel et al found an inverse relationship between ORN stage and healing rate – patients with Notani stage I ORN demonstrated greater healing than those with stage III disease. This suggests that medical therapy works best before extensive necrosis and bone fragmentation occur. Additionally, Patel et al reported that ORN secondary to oropharyngeal cancer radiotherapy responded more favorably than ORN from other primaries, possibly related to the radiation field or dose. Delanian et al’s trial suggested patients whose ORN followed surgery + RT healed faster than those after chemo + RT, possibly because chemotherapy exacerbates tissue hypoxia and fibrosis. Another key factor is infection control. Patel et al noted that patients who healed had required on average 1.3 antibiotic prescriptions versus 4.3 in those whose disease progressed – indicating that persistent infection can undermine the benefits of PENTO.
Efficacy in ORN Prevention
All 3 included studies on ORN PENTO prophylaxis reported low rates of ORN after dental extractions. Historically, the risk of ORN after extraction in an irradiated mandible can range widely. In the small case series by Owosho et al, none of the 4 patients developed ORN (0% incidence) with PENTO prophylaxis. While the sample is too small for definitive conclusions, it is notable that 2 of these patients had therapeutic extractions of molars in high-dose irradiated bone yet healed without complications.
Lombardi et al’s 29-patient audit found ORN in only 4 patients (5.6%) despite a total of 152 extractions performed. Importantly, these were relatively-complex extractions – nearly half involved raising mucoperiosteal flaps or removing multiple teeth. Only dental extractions resulted in ORN in their series; implant placement, which was performed in 4 patients, led to ORN in 1 patient (25% of implant cases). Lombardi et al’s data showed no cases of severe ORN requiring mandibulectomy.
The de Sousa et al study in Brazil likewise demonstrated zero ORN cases out of 74 extractions when using PENTO prophylaxis. By 2 weeks post-extraction, 86% of sockets had complete mucosal coverage, and there were no instances of dry socket or necrotic bone exposure. One socket (of 74) had a minor local infection, which resolved with antibiotics. These outcomes are markedly better than what would be expected without prophylaxis or even with other approaches like antibiotics alone or HBOT. Notably, even HBOT, which has been used for decades to prevent ORN, does not guarantee prevention – previous reports suggest HBOT prophylaxis yields ORN rates around 4% to 8% post-extraction. Although cross-study comparisons are imperfect, the 0% ORN in de Sousa et al (and Owosho et al) and ~5% in Lombardi et al indicate PENTO could be at least as effective as HBOT.
Another advantage observed was improved wound healing and reduced postoperative pain with PENTO. In de Sousa et al, most patients had no pain by 1 week post-extraction. This suggests that PENTO’s effects (perhaps improved microcirculation via PTX and enhanced tissue repair via tocopherol’s antioxidant action) may promote faster mucosal regeneration.
Efficacy in MRONJ Management
The use of PENTO for MRONJ is a newer application, but available studies indicate symptomatic relief and, in many cases, lesion improvement or resolution. While MRONJ is pathogenically distinct from ORN, there are overlapping features (bone ischemia, inflammation) that PENTO could favorably influence.
Symptomatic Improvement
All reports on PENTO in MRONJ note improvement in pain and swelling. Owosho et al found that every patient experienced relief of symptoms on PENTO. Some patients with chronic pain or foul discharge reported significant improvement within a few months. Treatment benefitted patient quality of life, independent of whether full bony healing occurred.
Effects on Bone Healing
Radiographic and clinical evidence of bone healing has been observed with PENTO in MRONJ, though results vary by stage of disease. In the Owosho et al series, radiographs demonstrated new bone formation in areas of lytic defects or sequestrum margins in all patients during PENTO treatment. Clinically, 2 of 7 patients had complete resolution of exposed bone, and another 2 had partial reduction in exposed bone. The remaining sites showed no progression; only 1 site showed no change in exposed bone despite radiographic improvement. In Słowik et al, who treated a broader MRONJ population, 46% of patients achieved full remission. The others mostly had stable disease or downstaging of MRONJ – for instance, some stage II lesions became asymptomatic stage I lesions. Only the most advanced cases (stage III with extensive bone involvement) had low rates of complete remission (around 7.5%), indicating that advanced MRONJ may require additional surgical intervention. Even in advanced cases, PENTO often led to enough improvement to avoid immediate major surgery, as none of Słowik et al’s 43 patients required resection during the follow-up period.
Disease Stage and Context
Similar to ORN, earlier-stage MRONJ appears to respond best. Patients with stage I MRONJ can often completely heal with conservative measures. This is dramatically demonstrated in the Colapinto et al RCT, where all stage I patients receiving surgery + PENTO healed, compared to a high failure rate with surgery alone. In that trial, adjunctive PENTO reduced the 6 month relapse rate from 71% in controls to <1% in the treatment arm, effectively preventing the usual cycle of recurrent MRONJ after initial surgery. Moreover, even those who initially did not receive PENTO eventually healed once the regimen was introduced. This provides strong evidence that PENTO synergizes with surgical debridement to promote definitive healing in early MRONJ. In more advanced MRONJ (stages II-III), surgical resection is often recommended as first-line. However, PENTO may offer a management strategy for patients who are not surgical candidates. The evidence suggests many stage II patients can at least exhibit symptomatic improvement with PENTO, and some might fully heal over extended treatment. Importantly, no study reported worsening of MRONJ due to PENTO, which is encouraging given the progressive nature of untreated MRONJ.
MRONJ Prevention
The concept of preventing MRONJ in at-risk individuals is relatively new. The case series by Magalhães et al suggests that PENTO prophylaxis around dental extractions might reduce the incidence or severity of MRONJ. In their 17 patients, the MRONJ incidence was 17.6% (3 out of 17 patients), which may seem high. All cases were stage I and healed promptly with continued PENTO. Without prophylaxis, MRONJ incidence after extraction in high-risk patients can be significantly higher and often of higher stage. Although this is a small case series, it hints that PENTO could potentially convert developing MRONJ into a milder, self-limiting form.
Safety and Tolerability
Across all studies and indications (ORN and MRONJ, treatment, and prevention), the PENTO regimen was consistently reported as safe and well tolerated. No serious adverse drug reactions were attributed to PENTO/PENTOCLO in any study. Minor side effects were occasionally observed, such as gastrointestinal discomfort, nausea, or dizziness. These did not typically require discontinuation of therapy. For example, in the de Sousa et al prophylaxis study, ~1 in 7 patients had mild nausea, which resolved spontaneously. PTX is known to cause hypotension or tachycardia in some cases, but no cardiovascular adverse events were reported, even with long-term use. Liver and kidney function remained stable as per the reports that mentioned monitoring.
One theoretical concern was whether adding clodronate could cause MRONJ. Clodronate is an oral first-generation bisphosphonate with a much lower potency. None of the PENTOCLO studies reported any MRONJ-like complications in their ORN patients. Thus, clodronate appeared safe in ORN patients.
Discussion
This systematic review indicates that PENTO/PENTOCLO has significant promise in both the treatment and prevention of refractory jaw osteonecrosis caused by radiation or medications. While the evidence is composed mainly of observational studies and small trials, the consistency of positive outcomes across diverse settings is noteworthy.
For ORN of the jaw, PENTO/PENTOCLO has transitioned over the past decade from an experimental approach to a recognized conservative management option. The therapy targets the underlying pathophysiology of radiation-induced endarteritis, hypoxia, and fibrosis by improving blood flow, scavenging reactive oxygen species, and reducing fibrosis. Clodronate is theorized to aid in bone remodeling. This pharmacologic approach can lead to healing of necrotic bone in a substantial subset of patients, something previously thought to be achievable only with surgery. This is a paradigm shift from the radical resection philosophy for ORN.
Importantly, most of the studies, which utilized PENTOCLO for ORN treatment, have included a preemptive antiseptic phase. This consists of 2 to 6 weeks of treatment of antibiotics, antifungals, and steroids, most commonly consisting of 50 mg of fluconazole and 2 g of amoxicillin-clavulanate ±1 g ciprofloxacin for antibiotics and either 16 mg methylprednisolone or 20 mg prednisone.4,7,11,12 This is important for controlling possible infectious sources in the irradiated tissue.
Initially trialed in breast cancer patients with postradiation fibrosis, this drug combination has now demonstrated positive outcomes in head and neck cancer patients with soft tissue fibrosis and ORN after radiation, as well as patients with MRONJ. One limitation of this review is the inconsistency of outcome measures across studies. Some studies track mucosal healing via physical examination while other evaluated radiographic evidence of bony healing. The length of follow-up is also significantly variable with no consensus on when to consider a patient healed and when to discontinue the medications.
The concept of using PENTO prophylactically is new but compelling. If validated in larger trials, this could change practice by providing a simple regimen to administer before and after dental extractions in irradiated patients, potentially replacing HBOT protocols. The practicality of an oral drug regimen is a major advantage over HBOT. HBOT is significantly more costly than the PENTOCLO medications, and there is limited access to centers with HBOT capabilities. 9 Additionally, patient compliance appears good with side effects minimal, which is crucial for prophylaxis. While only case series evidence is available so far, the absence of ORN in multiple cohorts with PENTO prophylaxis is encouraging.
When considering MRONJ, the inciting factor is antiresorptive or antiangiogenic medications rather than radiation. However, the pathogenic end result shares similarities. The results of using PENTO in MRONJ, particularly early stage, are quite promising and mirror the ORN experience. The 2023 randomized trial by Colapinto et al provides level I evidence that adding PENTO dramatically improves outcomes of surgical treatment of MRONJ. In the control group of that study, standard care (sequestrectomy and antibiotics) led to a relapse rate of 71%, consistent with the challenging nature of MRONJ. The fact that the PENTO group had near 0% relapse is striking and suggests that PENTO addresses the underlying impaired healing environment that persists even after removing necrotic bone. PTX’s ability to increase blood flow and reduce TNF-alpha might improve the post-surgery healing response, and tocopherol could help by reducing oxidative stress in the surgical site. This trial’s findings may well pave the way for PENTO becoming a standard adjunct in MRONJ management, at least for early stages.
Our own clinical experience with the PENTOCLO protocol has demonstrated promising results and improvement in control of acute postradiation oropharyngeal ulceration, mandibular ORN, and temporal bone osteomyelitis. Our experience has been in line with the positive preliminary results of the PENTOCLO protocol; however, the exact combination of medications, dosing, antiseptic portion, necessary duration of treatment, and surveillance remain nubilous. Yet, time to resolution is variable and clinical healing can be assessed by patient reported symptoms and physical examination; radiographic evidence of healing is limited in its delay to provide meaningful guidance. One study suggested the usage of 18F-FDG PET/CT imaging as a more effective surveillance tool to quickly identify patients with positive response. This is crucial as patients who do not respond to PENTOCLO may benefit from surgical options, which offer better odds when expedited. They found that 18F-FDG PET/CT was able to determine patients who were worsening on the therapy versus healing or stable after an average interval of 6 months from the prior 18F-FDG PET/CT. They also justified that this means of follow-up could serve multiple purposes for the patient’s surveillance including identifying other ORN sites or tumor recurrences and helping with surgical planning if needed. 20 Another group responded to this paper calling into question the metrics used by the authors and cautioning that patients may be incorrectly identified as nonresponders and undergo needless treatments. 21
There is a risk of recurrence of disease after the cessation of PENTOCLO, which is not well described. 22 Some clinicians continue treatment beyond the resolution of ORN to mitigate this. 22 Across the board, more research is necessary to determine the best ways to treat and follow these patients. MRONJ patients, likewise, have new hope for recovery or at least symptom palliation. While further high-quality studies are needed to establish standardized treatment protocols, current evidence supports incorporating PENTO into multidisciplinary care of these challenging conditions. Importantly, PENTO are inexpensive and generally accessible, which makes this approach feasible even in resource-limited settings. The positive findings thus far should be leveraged to inform clinical practice while we await more definitive evidence, with the understanding that careful patient selection and close monitoring remain paramount.
Conclusion
The use of the PENTO/PENTOCLO protocol for the treatment and prevention of ORN and MRONJ has shown promising outcomes across multiple studies. This paper is one of the first to collect these studies and present a compiling case for continued development and interest in these healing protocols for some of our most challenging patients. More research is needed to determine appropriate duration of treatment and surveillance methods. Additionally, other applications for this treatment regimen should be explored.
Footnotes
Ethical Considerations
There are no human participants in this article, and informed consent is not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Jason Ohlstein serves on the Editorial Board of the Ear, Nose & Throat Journal and is the Lead Guest Editor of the special collection “Scary Head and Neck Infections.” There are no other conflicting interests to declare.