
Abstract
Objective:
Nasal septal perforation (NSP) is characterized by defects in the mucosal, cartilaginous, and bony structures of the septum, most commonly resulting from septoplasty. Spontaneous healing of NSPs is rare, necessitating surgical intervention once the condition stabilizes. Numerous techniques have been developed for NSP repair. This study presents a novel technique combining fascia lata grafts, platelet-rich plasma (PRP), and diced septal cartilage harvested from the patient’s remaining deviated nasal septum for the repair of medium-sized NSPs.
Methods:
A retrospective analysis was conducted on 32 patients who underwent NSP repair between July 2022 and July 2023. The repair utilized fascia lata, PRP derived from venous blood, and diced cartilage from residual septal cartilage. The procedure involved an open rhinoplasty approach for graft placement, followed by stabilization using endoscopic techniques.
Results:
The mean horizontal and vertical diameters of the septal perforations were 12.06 ± 2.87 mm and 13.12 ± 2.44 mm, respectively. All patients had medium-sized perforations (0.5-2 cm). The mean follow-up period was 12.03 ± 1.11 months. Complete closure was achieved in 28 of 32 cases (87.5%). The cohort included 18 males (56.3%) and 14 females (43.8%), with a mean age of 35.47 ± 5.31 years (range: 25-45). Ten patients (31.3%) were smokers, among whom 4 experienced incomplete closure. Smoking was not significantly associated with repair failure (P = .06).
Conclusion:
This novel technique combining fascia lata, PRP, and diced septal cartilage offers a reliable and effective approach for the repair of medium-sized NSPs.
Introduction
Nasal septal perforation (NSP) refers to a defect that penetrates the cartilaginous and bony components of the nasal septum, disrupting the mucosal layers on both sides. The etiology of NSP is multifactorial, encompassing traumatic, iatrogenic, and environmental causes. These include septal surgery, mucosal cauterization, prolonged nasal packing, instrumentation, digital trauma, or foreign bodies. Additionally, intranasal drug use (eg, decongestants, corticosteroids, or cocaine), occupational exposure to irritants like chromium, sulfuric acid, or powdered glass, systemic inflammatory diseases (eg, granulomatosis with polyangiitis, sarcoidosis, systemic lupus erythematosus, or rheumatoid arthritis), infections (eg, syphilis, tuberculosis, HIV, fungal infections, or leprosy), and neoplasms can also contribute to NSP development. Notably, septal surgery remains the most prevalent cause, with the incidence of NSP following septoplasty ranging from 0.5% to 3.1%.1,2
The clinical presentation of NSP depends on the defect’s size and location. Symptoms may include nasal obstruction, crusting, epistaxis, audible whistling during respiration, and impaired nasal airflow. However, smaller or asymptomatic perforations can remain undiagnosed. 3
Traditional methods for repairing NSP often use autologous fascia lata grafts, either alone or in combination with other grafts or flaps, to reconstruct the septal defect. More recently, biomaterials such as platelet-rich fibrin, platelet-rich plasma (PRP), hyaluronic acid, and adipose-derived tissue have been incorporated into repair strategies, showing promising results in promoting tissue regeneration and achieving defect closure. 4
Despite advancements in both open and endoscopic surgical techniques, no universally accepted method exists for managing NSP across different sizes and locations. This study proposes a novel approach for repairing medium-sized NSPs by utilizing diced septal cartilage and fascia lata grafts augmented with PRP, aiming to achieve reliable outcomes and enhanced tissue integration.
Materials and Methods
This retrospective study was approved by the local ethics committee, with formal permission granted by Prof. Cemil Taşcıoğlu City Hospital. Written informed consent was obtained from all participants. Over 60 patients diagnosed with NSP at Prof. Cemil Taşcıoğlu City Hospital between July 2022 and July 2023 were initially evaluated. Of these, 32 patients who experienced persistent symptoms—such as crusting, whistling, epistaxis, and nasal obstruction—and agreed to undergo surgical repair using a fascia lata graft were included. Patients who declined surgical intervention, those with comorbidities precluding the use of general anesthesia, and individuals in the pediatric age group were excluded. No patient had a history of comorbid conditions such as diabetes mellitus. Additionally, none of the patients had a history of intranasal substance use (involving nasal decongestants, corticosteroids, or cocaine). All patients underwent a detailed rheumatological examination before the operation and none were diagnosed with any diseases (such as granulomatosis with polyangiitis, sarcoidosis, systemic lupus erythematosus, or rheumatoid arthritis). Moreover, no signs of preoperative infection (such as syphilis, tuberculosis, HIV, fungal infections, or leprosy) were detected in any of the patients. Data regarding age, gender, perforation dimensions, and smoking status were collected. All included cases involved medium-sized NSPs, measuring between 0.5 and 2 cm in diameter.
Surgical Procedure
The procedure was performed under general anesthesia. Local infiltration of the nasal septum was achieved using 1% lidocaine with epinephrine (1:100 000), and the nasal cavity was packed with gauze soaked in 0.1% xylometazoline hydrochloride to reduce intraoperative bleeding. After a 5-minute decongestion period, the size of the perforation was measured. The edges of the perforation were carefully incised with a sickle scalpel, and 1 mm of tissue was excised circumferentially to expose viable mucosa. Access to the nasal septum was obtained via a Goodman incision combined with bilateral alar rim incisions. The dorsal nasal skin was elevated, and bilateral mucoperichondrial flaps were raised to ensure complete circumferential coverage of the perforation. A deviated cartilage piece from the nasal septum was excised for use as a graft. The excised deviated cartilage was then cut into small pieces with a scalpel to create diced cartilage for the repair (Figure 1).

Harvesting of diced septal cartilage. Residual septal cartilage fragments are obtained during the correction of a deviated septum. The cartilage is prepared by finely dicing into small pieces for use in the repair of the nasal septal perforation.
Platelet-Rich Plasma
It was derived intraoperatively from autologous venous blood through centrifugation (Figure 2). PRP was prepared using the double-spin centrifugation method. Autologous blood was drawn under sterile conditions and initially centrifuged at a low speed (eg, 160 g for 10 minutes) to separate plasma and platelets from red blood cells. The supernatant containing PRP was then subjected to a second, higher-speed centrifugation (eg, 250-400 g for 10-15 minutes) to concentrate the platelets. This protocol, based on methods described by Marx, 5 Perez et al, 6 and Yin et al, 7 ensures an optimal platelet concentration while preserving growth factor integrity, making it suitable for regenerative applications.

Platelet-rich plasma (PRP). PRP is derived from autologous venous blood through centrifugation. The process isolates the platelet-rich component, which is then used to enhance the healing process and tissue regeneration in the repair.
Fascia Lata Graft
A ‘S’ incision is made along the lateral thigh, from the iliotibial band to the knee, allowing access to the fascia lata. The fascia is carefully dissected from the underlying muscle and surrounding tissues. The desired portion of fascia is harvested based on the size needed for the procedure. After harvesting, the incision is closed in layers to prevent complications such as hematoma or infection.
The harvested fascia lata graft was spread out, and diced cartilage was combined with PRP before being placed onto the graft (Figure 3). The fascia lata was folded around the cartilage and PRP mixture to encapsulate it, and the edges were secured with 4-0 Vicryl sutures (Ethicon, Johnson & Johnson, Somerville, NJ, USA) to create a composite graft (Figure 4). The composite graft was inserted between the bilateral mucoperichondrial flaps to cover the perforation entirely. Endoscopic evaluation was performed using 0° and 30° angled endoscopes to confirm proper placement and eliminate any gaps around the graft or perforation (Figure 5). The graft was stabilized with transseptal sutures using 4-0 Vicryl material (Ethicon, Johnson & Johnson, Somerville, NJ, USA), and the columella incision was closed with 6-0 PROLENE sutures (Ethicon, Johnson & Johnson, Somerville, NJ, USA). Bilateral silastic nasal splints were placed and left in position for 1 month.
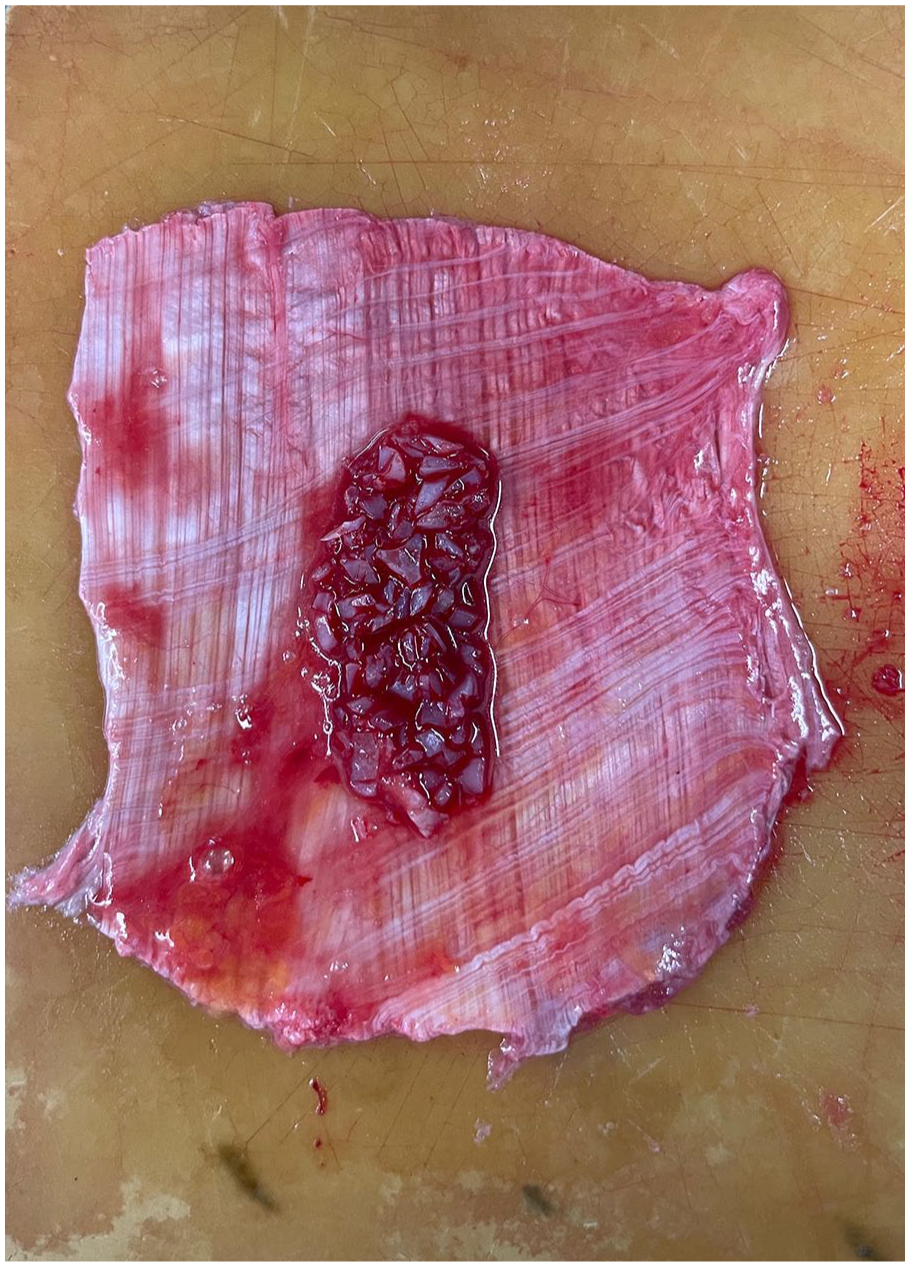
Fascia lata graft combined with diced cartilage and PRP. The fascia lata graft is spread out and combined with the diced septal cartilage and PRP to form a composite graft. This mixture is prepared for placement in the nasal septal perforation. PRP, platelet-rich plasma.

Formation of composite graft. The fascia lata is folded around the diced cartilage and PRP mixture, encapsulating the graft. The edges are secured with 4-0 Vicryl sutures to form a stable composite graft for septal perforation repair. PRP, platelet-rich plasma.
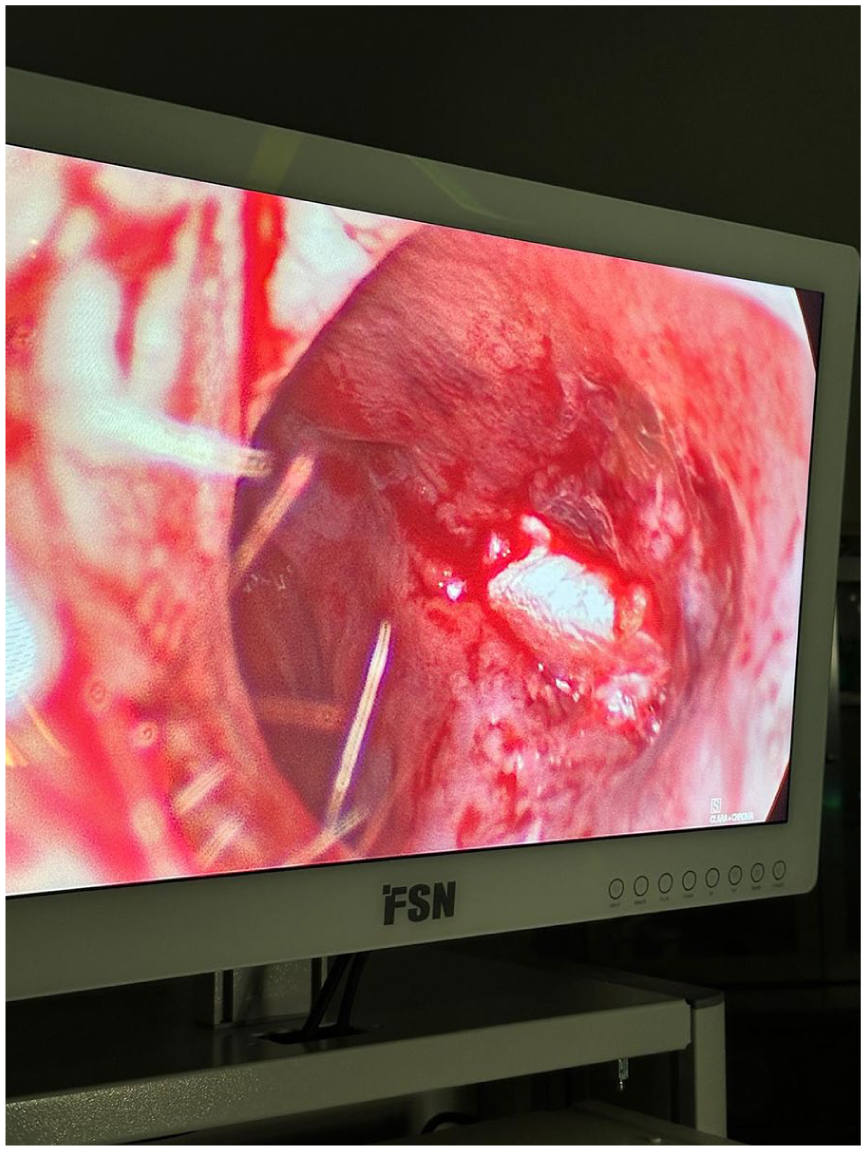
Endoscopic evaluation of graft placement. Endoscopic evaluation is performed using 0° and 30° angled endoscopes to confirm proper placement of the composite graft and ensure there are no gaps around the graft or the perforation site.
Postoperatively, the thigh is elevated to reduce swelling, and pain management is provided. All patients received amoxicillin-clavulanic acid (1000 mg twice daily) until splint removal. Moisturization of the nasal cavity was maintained with saline and oil-based nasal sprays, recommended at least 3 times daily until splints were removed. In cases where crusting persisted, continued use of nasal sprays was advised.
Postoperative graft integration and overall outcomes were monitored at the 1st, 3rd, 6th, and 12th months. Examples from the follow-up examinations conducted at the 1st and 12th months are presented (Figure 6).
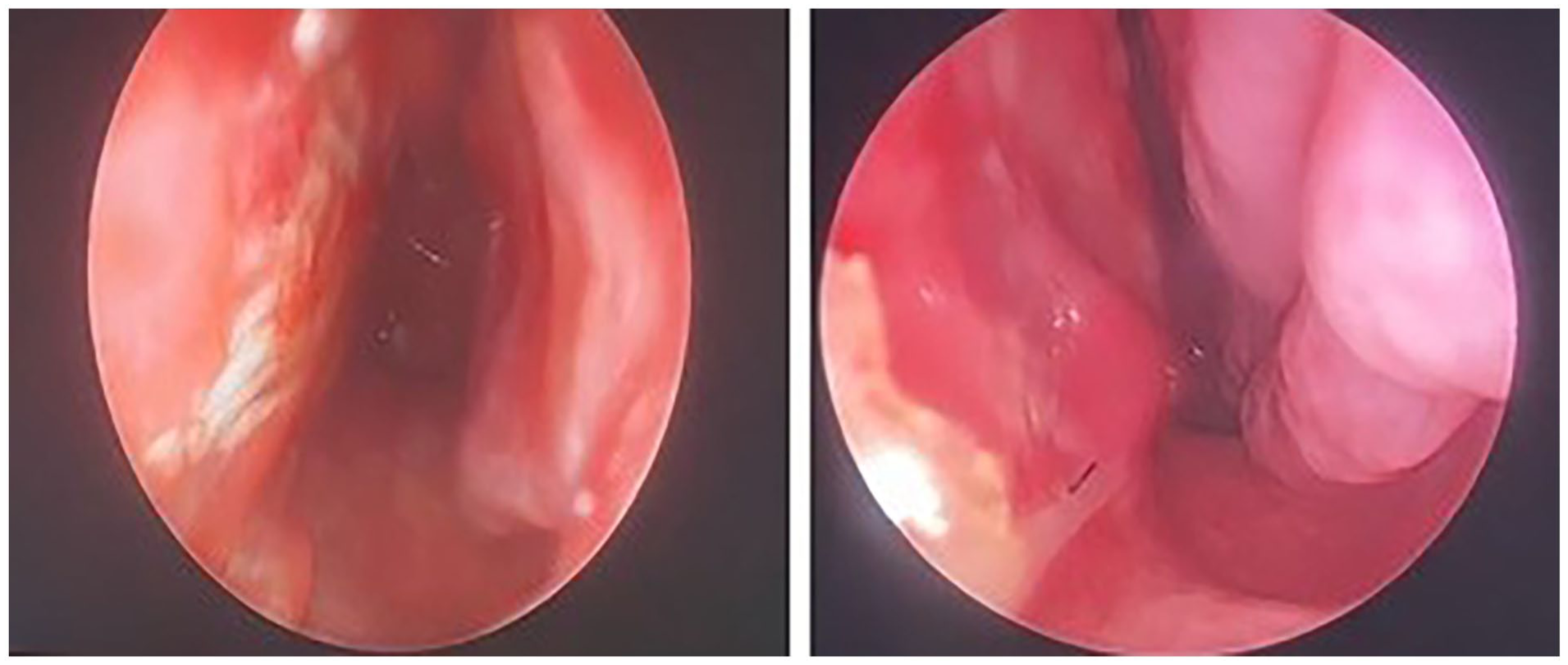
Follow-up postoperative evaluation. The graft integration is evaluated during the follow-up examinations at the first and twelfth months postoperatively. The figure shows the outcome of the nasal septal perforation repair and the healing process.
Statistical Analysis
Categorical variables such as smoking status, gender, and perforation etiology were analyzed using Fisher’s exact test or chi-square test as appropriate. Continuous variables such as age and perforation dimensions were analyzed using the Mann–Whitney U-test. Statistical significance was defined as P < .05. Analyses were performed using IBM SPSS Statistics version 25.0 (IBM Corp., Armonk, NY, USA).
Results
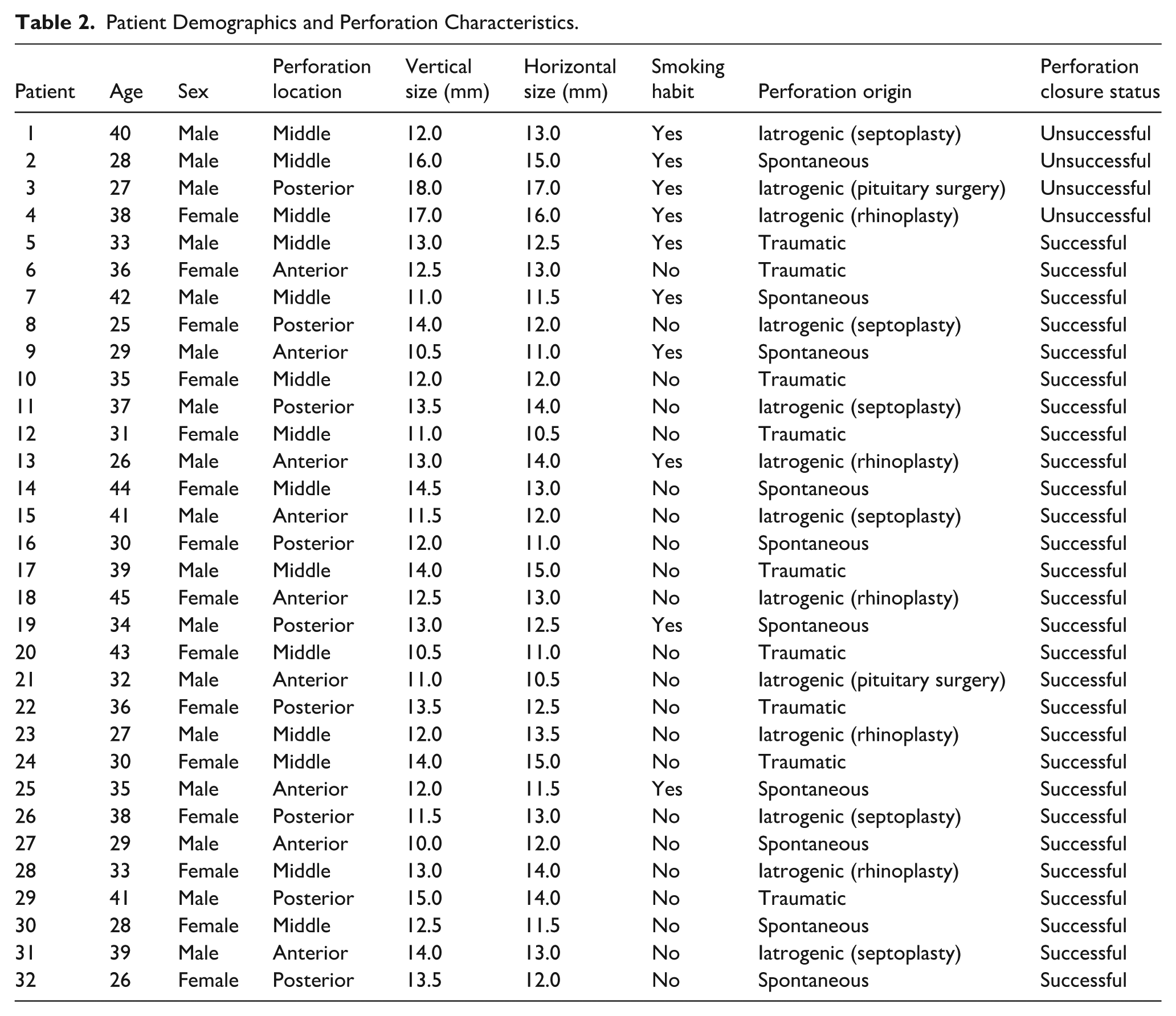
The study included 32 patients with medium-sized NSPs, ranging from 0.5 to 2 cm, with a mean horizontal size of 12 mm and a mean vertical size of 13 mm. The cohort consisted of 18 males (56.3%) and 14 females (43.8%), with a mean age of 35.47 years (range: 25-45). All patients were followed for 12 months, regardless of whether the perforation was successfully closed or remained persistent. Complete closure of the perforation was achieved in 28 out of 32 cases (87.5%).
Preoperative assessments included comprehensive rheumatological evaluations to exclude systemic conditions such as granulomatosis with polyangiitis, sarcoidosis, systemic lupus erythematosus, and rheumatoid arthritis. Additionally, no preoperative infections—including syphilis, tuberculosis, HIV, fungal infections, or leprosy—were detected in any of the patients.
Of the 32 patients, 10 (31.3%) were active smokers. Among this group, 4 patients experienced incomplete closure of the perforation at the 12-month follow-up, accounting for all cases of unsuccessful closure in the study (Table 1). In contrast, all 22 non-smokers achieved complete closure. Detailed characteristics of all patients, including age, gender, perforation etiology are presented in Table 2. No statistically significant association was found between perforation closure and patient age (Mann–Whitney U-test, P = .73) or perforation etiology (chi-square test, P = .26). However, statistically significant differences were found between closure status and perforation vertical size (Mann–Whitney U-test, P = .03) as well as horizontal size (Mann–Whitney U test, P = .01), with unsuccessful closures tending to have larger perforation dimensions. Fisher’s exact test showed no statistically significant association between smoking status and unsuccessful NSP repair outcomes (P = .06).
Patient Characteristics With Unsuccessful Septal Perforation Repair.
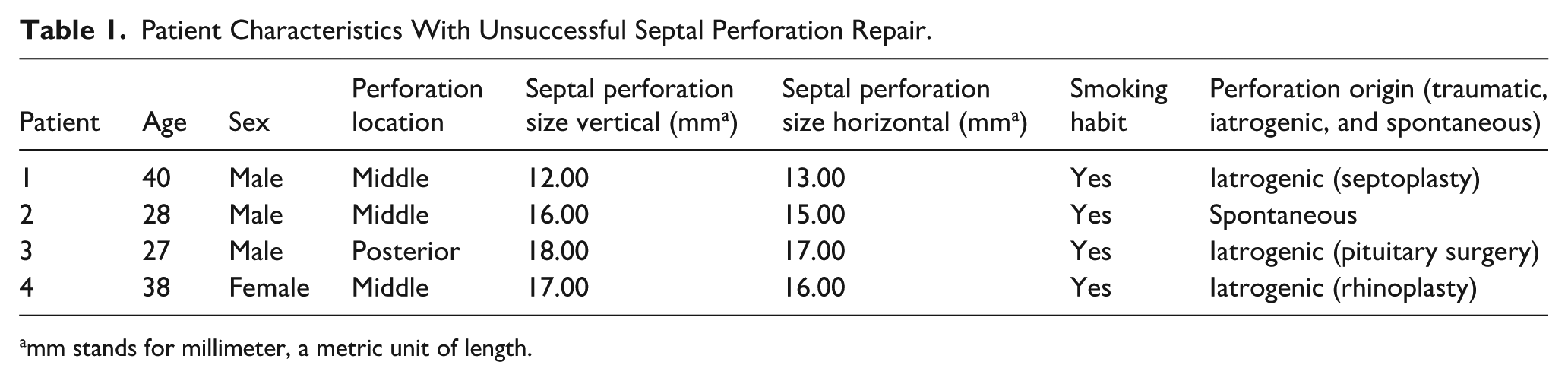
mm stands for millimeter, a metric unit of length.
Patient Demographics and Perforation Characteristics.
No complications were encountered during or after the surgical procedure. No infections were observed at the donor site. The administration of antibiotics—continued until the removal of nasal splints due to foreign body reaction—did not result in any adverse effects in any of the patients. During follow-up, no obstructive symptoms or breathing difficulties were observed related to the combined graft. Furthermore, the thickness of the double-layered composite graft was found to be comparable to that of the native nasal septum.
Discussion
The treatment of NSP can be broadly classified into 3 main approaches. Repairing medium and large-sized NSPs (>0.5 cm) is particularly challenging and carries the risk of persistent perforation.4 -8 In our study, patients with medium-sized perforations were included due to the difficulty of utilizing diced cartilage obtained from deviated septal cartilage.
Another option involves the use of composite grafts, such as conchal cartilage with intact perichondrium, tragal cartilage interposition grafts, and mucosal transposition flaps with human acellular dermis.8 -11 While these techniques demonstrate high success rates, none provide a universal solution for all types of NSP. Among graft materials frequently used for medium and large perforation repair, fascia, and cartilage grafts stand out due to their high success rates. However, cartilage grafts other than nasal septal cartilage have limitations, such as the curved structure of auricular conchal or tragal cartilage grafts and the technical challenges associated with harvesting costal cartilage.
Fascia lata and temporal fascia are commonly used tissues in otolaryngologic surgery. While temporal fascia is widely employed with success, it has limitations regarding durability and availability.9,10,12 In contrast, fascia lata is highly favored due to its thickness and the ability to be harvested in larger sizes. This tissue is utilized not only for perforation repair but also in endoscopic anterior skull base surgery for duraplasty and as a camouflage material in rhinoplasty. Clinical studies have demonstrated successful use of fascia lata, particularly in large or recurrent NSP cases, and when combined with costal cartilage as a sandwich graft.13,14 In our study, we exclusively used fascia lata as the graft material and harvested diced cartilage from the patient’s own deviated nasal septum, thus avoiding the need for an additional donor site.
PRP, which has recently gained widespread clinical use, is rich in growth factors, cytokines, chemokines, and cell adhesion molecules that contribute to healing, tissue proliferation, and regeneration.15,16 It is an autologous biological material easily obtained from the patient’s own blood. Despite its extensive use, the exact mechanism of PRP remains unclear. Several proteins within PRP have been highlighted, including transforming growth factor-β (TGF-β), epidermal and vascular endothelial growth factors (EGF and VEGF), platelet-derived growth factors, fibroblast growth factors, and insulin-like growth factors (IGF-1). TGF-β, secreted by platelets and macrophages, has an anti-proliferative role in healthy epithelial cells. 17 It targets marrow stem cells, fibroblasts, and pre-osteoblasts, promoting bone regeneration and long-term healing while inhibiting osteoclast activity. Additionally, TGF-β contributes to epithelial and vascular endothelial cell growth and collagen production. EGF promotes cell proliferation and differentiation via the EGF receptor and plays a crucial role in angiogenesis and wound healing. 18 VEGFs, as signaling proteins, encourage the differentiation of precursor cells into mature endothelial cells and the maturation of specific blood vessels such as capillaries. 19 Based on these mechanisms, our clinical experiences show that combining PRP with fascia lata grafts significantly enhances NSP repair success rates. 14 We believe PRP acts as a strong adhesive within the fascia lata and diced cartilage structure, while also playing a crucial role in early postoperative graft nourishment.
Ensuring graft viability postoperatively is crucial for optimal outcomes. Postoperative drying and crusting are common complications; therefore, nasal splints were used for 1 month to protect the graft. Patients were instructed to maintain nasal cavity moisture with saline and oil-based sprays at least 3 times daily until splint removal. 20 After splint removal, saline irrigation and debridement during follow-ups further contributed to successful healing.
While traditional open approaches have historically been preferred for NSP repair due to direct visualization and operative control, recent advances in endoscopic techniques have significantly enhanced surgical outcomes. Techniques utilizing anterior ethmoid artery flaps or greater palatine artery pedicled flaps via endoscopic access have shown high success rates and low morbidity in appropriately selected cases.21,22 The referenced article was published prior to the development of contemporary endoscopic techniques and does not reflect current surgical capabilities. 23 In our study, we utilized an open approach primarily to harvest deviated septal cartilage and to achieve optimal graft bed preparation under direct visualization. However, we also employed endoscopic assistance during graft placement and stabilization to enhance intraoperative precision, particularly in posterior regions that are otherwise challenging to visualize. Thus, our technique combines the advantages of both approaches, ensuring adequate exposure and precise positioning of the composite graft.
In this study, only 4 unsuccessful outcomes were observed, all in smokers. No significant correlation was found between patient age and perforation closure rates. Smoking impairs blood flow and neovascularization, leading to graft rejection. Between the third and fourth days post-injury, reparative cells such as fibroblasts, epithelial cells, and endothelial cells become active, contributing to extracellular matrix production, barrier regeneration, and new vessel formation. Smoking disrupts this healing process by inhibiting fibroblast activities such as chemotaxis, migration, and proliferation, while also reducing collagen production. Although statistical analysis in this study did not demonstrate a significant association between smoking and repair failure risk (P = .06), clinical experience and previous literature suggest that with a larger sample size, a statistically significant detrimental effect might be observed. This observation highlights the potential detrimental effects of smoking on graft viability and healing, warranting further investigation. 24
A limitation of this study is the relatively small sample size, limiting the ability to make broad comparisons between different techniques. A larger cohort would be necessary to more thoroughly assess the relative efficacy of various NSP repair approaches. Additionally, future studies could evaluate outcomes based on different perforation sizes to better understand the impact of grafting techniques on perforations of varying diameters.
Conclusion
This novel technique, combining fascia lata, PRP, and diced septal cartilage, offers a reliable and effective approach for repairing medium-sized NSPs. The technique has shown promising results in achieving complete perforation closure and highlights the importance of addressing modifiable factors such as smoking to optimize surgical outcomes.
Footnotes
Ethical Considerations
This study was approved by the University of Health Sciences, Prof. Dr. Cemil Tascioglu City Hospital Ethic Committee (23.05.2022, E-48670771-514.99).
Consent to Participate
The study was designed as a retrospective study. All patients signed written informed consent.
Author Contributions
All authors contributed to the planning, design, literature survey, experiment, and active intellectual support.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data for this study are presented in this paper.