
Abstract
Introduction
Nasal septal perforation (NSP) refers to a structural defect penetrating the cartilaginous and bony nasal septum, affecting the mucosa on both sides. NSP can result from various factors, including trauma or iatrogenic events (such as septal surgery, cauterization of the nasal mucosa, prolonged nasal packing or probing, digital manipulation, or the presence of foreign bodies), intranasal drug abuse (involving nasal decongestants, corticosteroids, or cocaine), occupational exposure (to substances such as chromium fumes, sulfuric acid, swarf, or powdered glass), inflammatory conditions (such as Granulomatosis with Polyangiitis, sarcoidosis, systemic lupus erythematosus, or rheumatoid arthritis), infectious diseases (such as syphilis, tuberculosis, HIV, fungal infections or leprosy), and neoplasms. However, septal surgery remains the most common cause of NSP.1,2 The recorded incidence of septal perforation following septoplasty has been documented within a range of 0.5% to 3.1%. Standard NSP symptoms include epistaxis, breathing difficulties, whistling sounds, crusting, and nasal airway obstruction. The presence or absence of symptoms directly correlates with the size and location of the nasal septum perforation. 3
Conventional approaches to repair NSP often include the application of homologous fascia lata grafts, either as an independent technique or in conjunction with other grafts or flaps. Numerous studies have highlighted the efficacy of biomaterials such as platelet-rich fibrin, platelet-rich plasma, hyaluronic acid, and adipose tissue in repairing NSP, showcasing their effectiveness in restoring tissue integrity. 4
Despite various surgical techniques using open or endoscopic approaches, there currently needs to be a universally accepted technique for repairing NSPs of different sizes and locations. Our research introduces an innovative method for repairing medium-sized NSPs using diced septal cartilage and a fascia lata graft combined with fat tissue called TriCelluFuse.
Materials and Methods
This retrospective study was conducted with the approval of the local ethics committee, and Prof. Cemil Taşçioğlu City Hospital granted permission. Informed consent was obtained from all participants enrolled in the study. The research involved more than 50 patients diagnosed with NSP, assessed between January 2021 and January 2023 at Prof. Cemil Taşçioğlu City Hospital. Of these, 22 patients with persistent symptoms such as crusting, whistling, epistaxis, and nasal obstruction who agreed to undergo NSP repair using a fascia lata graft were included in the study. Patients who declined surgery, those with comorbidities preventing the use of general anesthesia, and pediatric age groups were excluded. The study recorded the age, gender, dimensions of the perforation, and smoking habits of the participants. All patients with NSPs were chosen as medium-sized (0.5-2 cm).
All procedures were performed under general anesthesia. The nasal septum mucosa was injected with 1% lidocaine with a 1:100,000 epinephrine solution, and the nasal cavity was treated with nasal packing soaked in 0.1% xylometazoline hydrochloride to minimize intraoperative bleeding. After 5 minutes of decongestion, the size of the septal perforation was measured. The perforation edges were incised using a sickle scalpel, and the free edges were excised 1 mm circumferentially to create viable mucosa. A Goodman incision was combined with incisions on the alar rim on both sides. The dorsal nasal skin was elevated to reach the nasal septum between the medial crura of the lower lateral cartilages. The bilateral mucoperichondrial flaps were raised to cover all points of the NSP in a 360° manner. In the subsequent stage of surgery, the patient’s right thigh was prepared (Figure 1), and a fascia lata graft and fat tissue were harvested at the same incision. The diced cartilage graft was obtained from the remaining fragments due to deviation in the nasal septal cartilage. No alternative donor site was used for the diced cartilage graft. Fat tissue and diced cartilage were placed on the spread fascia lata graft (Figure 2). The fat graft was shuffled into microfat using a 2.4 mm anaerobic transfer technique from Luer to Luer (Figure 3). Fat was The fascia lata graft was sutured at its free edges. It was folded to encompass the central fat tissue and diced cartilage, using 4.0 Vicryl material to create the TriCelluFuse graft (Figure 4). The graft was gently inserted through the mucoperichondrial flaps, covering the NSP circumferentially. Endoscopic examinations were performed at 0° and 30° angles to ensure no accidental gaps around the graft or NSP. Transseptal sutures were performed using a 4/0 Vicryl suture passing through the graft. The columella incisions were sutured with a 5/0 prolene suture. Silastic nasal splints were inserted bilaterally and remained in the nasal cavities for 1 month. All patients received amoxicillin + clavulanic acid (1000 mg BI) until the removal of nasal splints. To maintain moisture in the nasal cavities, patients were advised to use nasal saline and oily sprays at least 3 times a day until the removal of the nasal splints. In the cases of nasal crusting after removal of the splint, continued use of nasal sprays was recommended.
The patient’s right thigh underwent preparation to harvest the fascia lata graft.
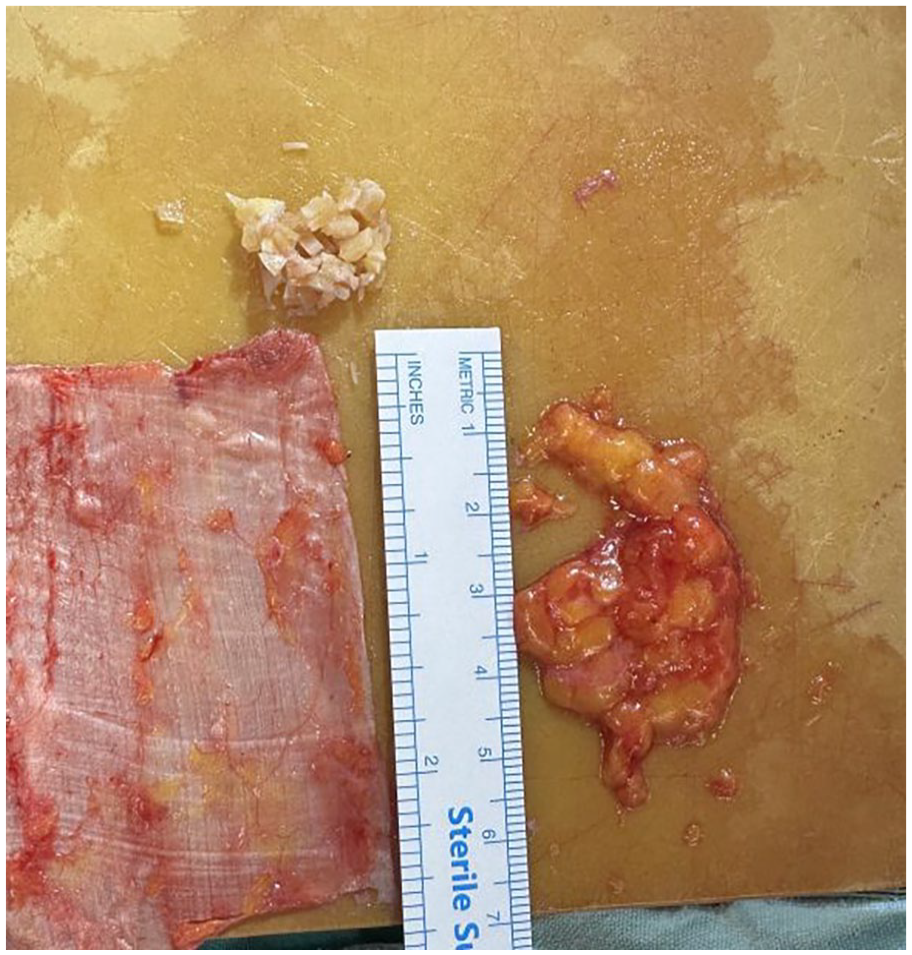
Fascia lata graft, fat tissue, and diced cartilage graft obtained from septal cartilage.
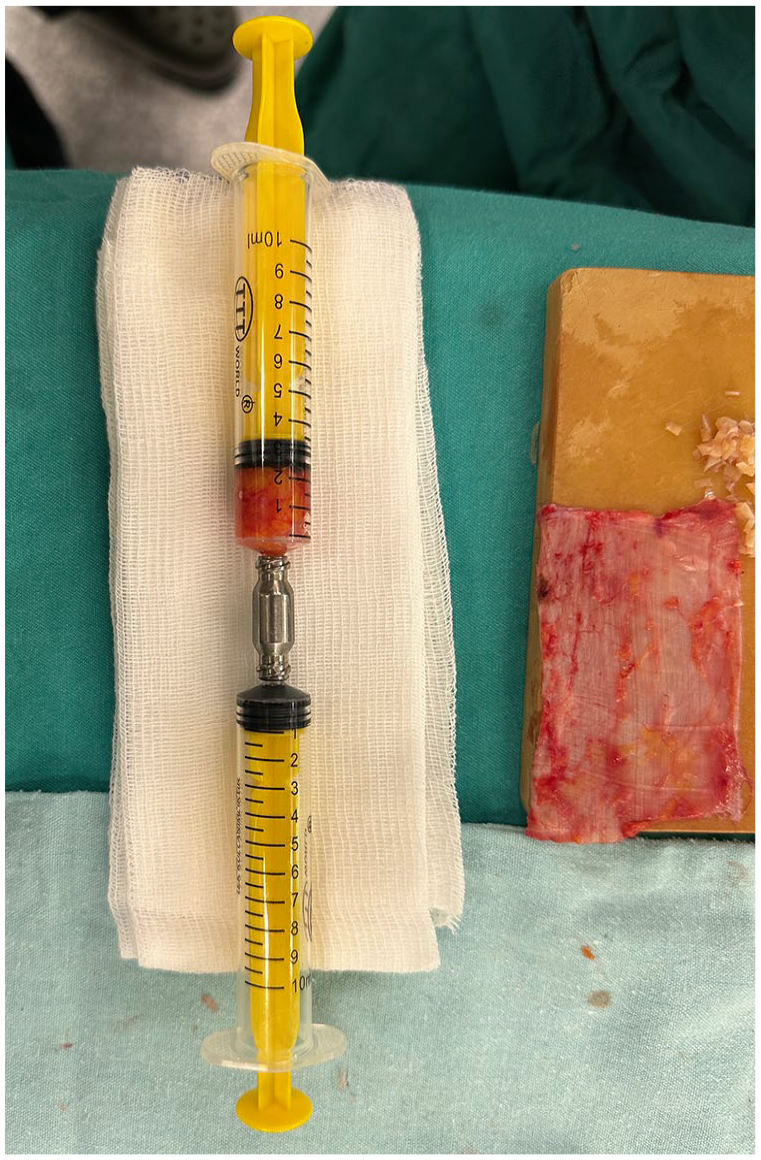
Preparation of the fat tissue with a microdebrider.
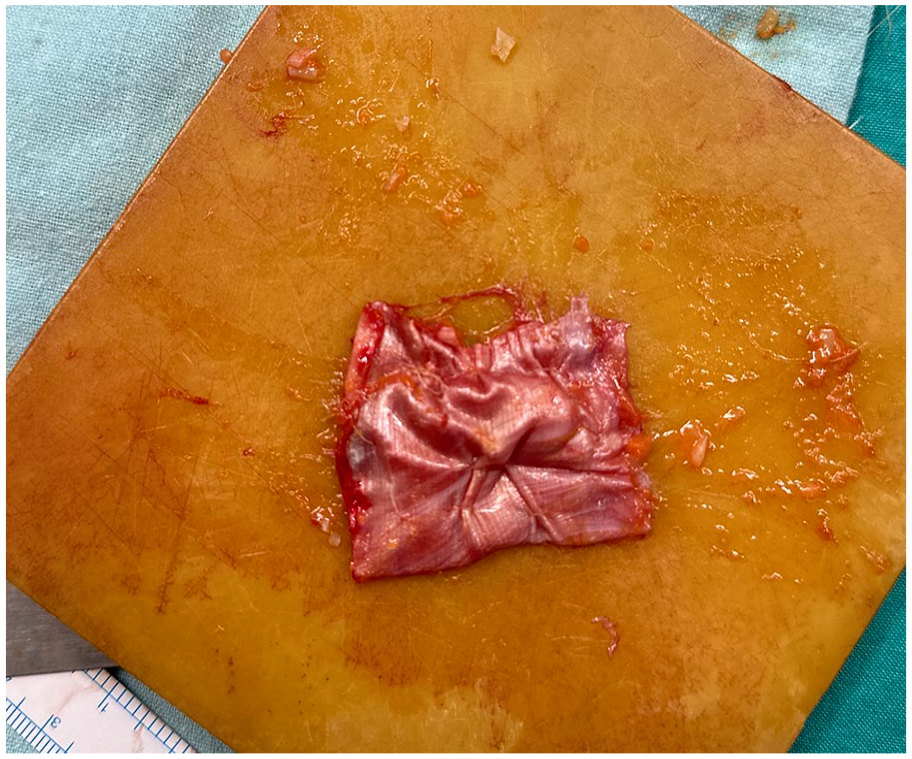
The edges of the fascia lata graft were stitched together, forming a fold around the central fat tissue and diced cartilage, thus forming the TriCelluFuse graft.
Postoperatively, all cases were monitored at the first, second, sixth, and twelfth months, and the graft condition was observed (Figure 5).
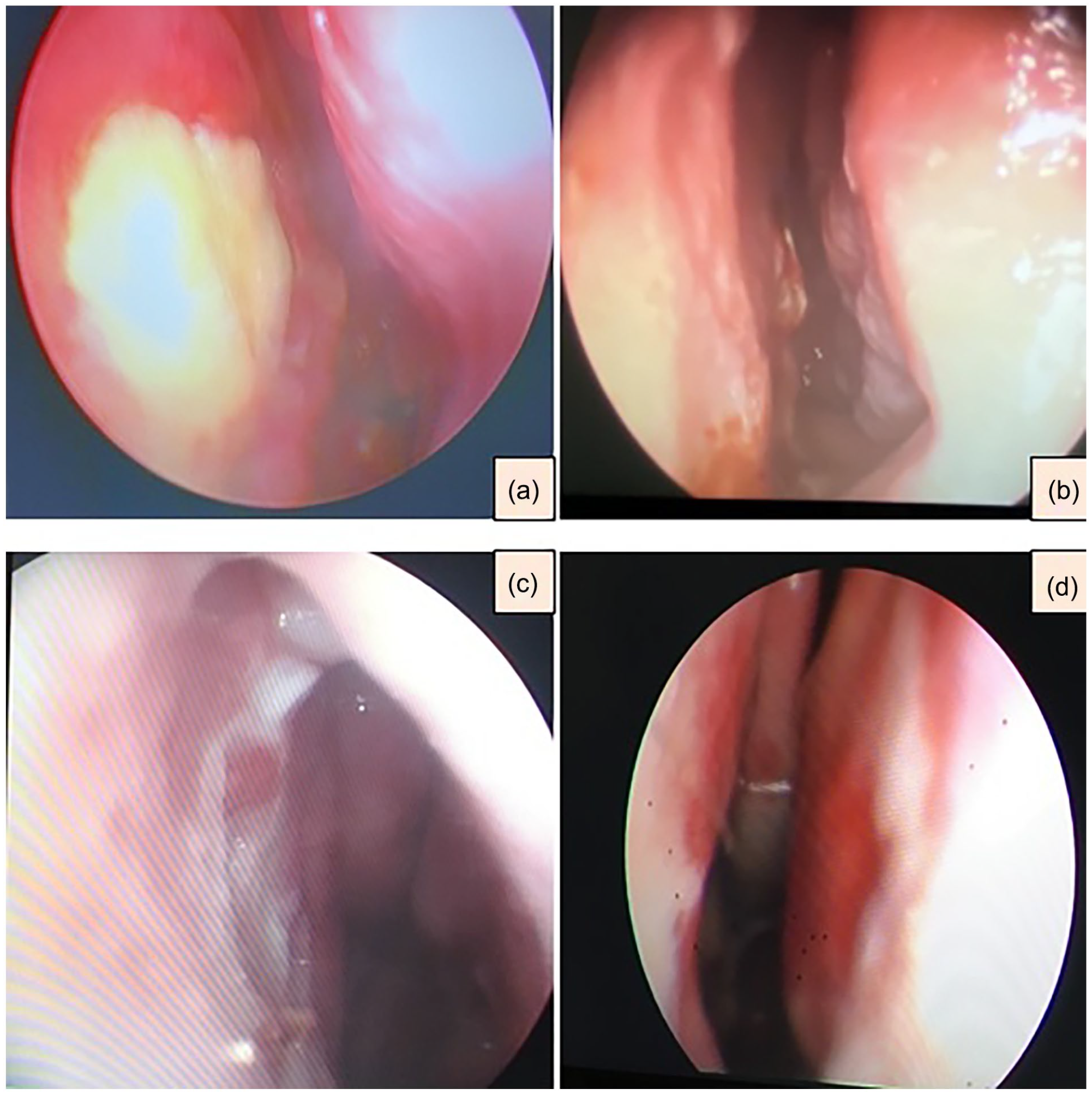
Post-surgery endoscopic examination showing the state of the graft at intervals of the first, second, sixth, and twelfth months (denoted as a, b, c, and d, respectively).
Results
All patients with NSP were selected with a medium initial and final perforation size (0.5-2 cm). In 20 out of 22 patients (91%), the etiology of the perforation was iatrogenic due to previous surgery. The perforation was spontaneous in 2 patients (9%). No patient had a history of comorbid conditions such as diabetes mellitus. Additionally, none of the patients had a history of intranasal substance use (involving nasal decongestants, corticosteroids, or cocaine). All patients underwent a detailed rheumatological examination before the operation and none were diagnosed with any diseases (such as Granulomatosis with Polyangiitis, sarcoidosis, systemic lupus erythematosus, or rheumatoid arthritis). Moreover, no signs of preoperative infection (such as syphilis, tuberculosis, HIV, fungal infections, or leprosy) were detected in any of the patients. The mean follow-up period was 12 months. Complete closure of the NSP was achieved in 19 out of 22 patients (86.3%). Among the cases, 15 were male (68%), and the ages ranged from 25 to 45 years, with a mean age of 35. Eight cases (36%) were smokers. After 12 months postoperatively, closure was not achieved in 3 medium-sized NSPs due to smoking. No complications were observed at the donor site. Within the smoker group, there were 3 failures and 5 successful closures. Conversely, in the non-smoker group, all patients (14 patients) achieved successful closures. These data were analyzed using the Fisher exact test to ascertain the presence of a statistically significant difference in closure success between the smoker and non-smoker cohorts. The analysis revealed that the failure rate in the smoker group was statistically significant (P = .036) (Table 1). These findings suggest an association between smoking and an increased risk of failure in NSP closure procedures; however, it is essential to note that this relationship is associative rather than causal.
Septal Perforation Closure Incidence in Both Groups.
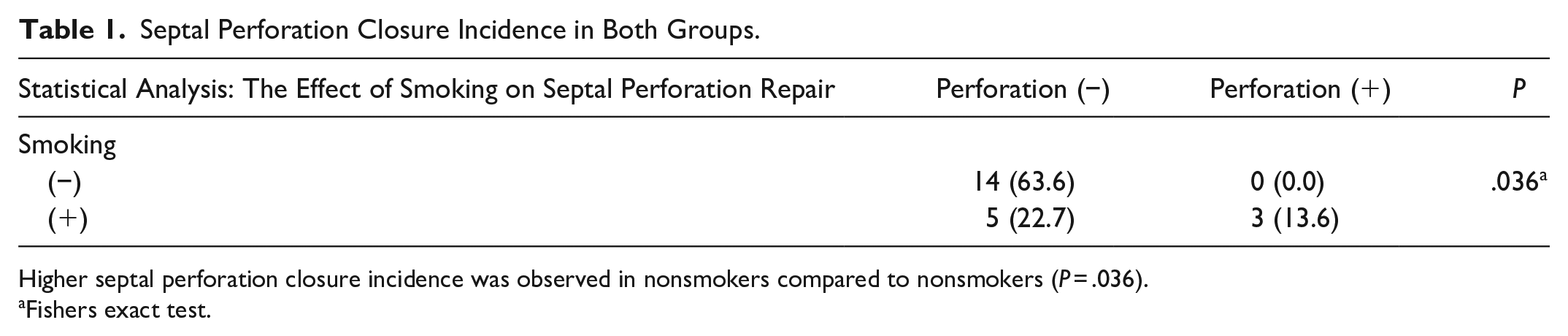
Higher septal perforation closure incidence was observed in nonsmokers compared to nonsmokers (P = .036).
Fishers exact test.
Discussion
NSP treatment can be divided into 3 main approaches. First, it is known that the repair of medium and large NSPs (>0.5 cm) is challenging and is associated with the risk of persistent NSP.4,5 Our study included patients with medium-sized septal perforations since repair of diced cartilage tissue obtained from the deviated septal cartilage is difficult. Another alternative treatment option is the nasal septum button. However, it has limitations, such as side effects and the potential for the defect to grow. 6
Secondly, alternative methods involve composite grafts, such as conchal cartilage grafts with intact perichondrium, tragal cartilage interposition grafts, and mucosal transposition flaps with human acellular dermis.7-9 While these techniques have demonstrated high success rates, none offer a comprehensive cure for all types of NSPs. There are disadvantages associated with cartilage grafts because ear cartilage is curved and limited, and the harvesting of costal cartilage can be more challenging. Another study in our clinic reported successful repair of NSPs even using a fascia lata and costal cartilage sandwich graft. 10 Although the temporal fascia is widely used, it has limitations in strength and quantity. 8 Additionally, the use of 2 different graft materials increases the risk of morbidity at the donor site.
The fascia lata graft, traditionally used in camouflage rhinoplasty due to its thickness and potential for substantial sizes, requires a separate incision. It may lead to minor additional morbidity and scarring on the thigh. 11 In our study, we obtained the fascia lata of the fat graft through an incision made for it from subcutaneous fat tissue. We exclusively used fascia lata as graft material, taking into account its thickness and abundance. Additionally, we obtained the diced cartilage graft from the patient’s nasal septal cartilage, avoiding using another donor area. The drawback of this technique lies in aesthetic concerns on the lateral aspect of the leg, particularly in young women.
Regarding the surgical approach, the open technique offers superior visibility compared to the endoscopic approach. 12 The endoscopic method might have limitations in effectively manipulating the inferior and posterior septal regions. However, endoscopy improves visualization during surgery and allows for checks of graft stability. 13
Ensuring graft vitality during the postoperative period is crucial. Postoperative drying and crusting are common, so we used nasal splints for 1 month after the operation to protect the graft. Nasal cavities should be kept moist using normal saline and oil sprays at least 3 times a day until the removal of the splints.5,14
Studies have shown that fat tissue contains numerous growth factors, cytokines, chemokines, and cell adhesion molecules.16,17 These components support the fascia lata graft and promote the healing process, tissue proliferation, and regeneration.17,18 Fat tissue stands out in the literature as a readily available autologous biological material. Using fat tissue in conjunction with fascia lata graft in our fusion graft model has contributed to the high success rate achieved in NSP.
Three to 4 days post-injury, reparative cells such as fibroblasts, epithelial, and endothelial cells become active, contributing to extracellular matrix production, barrier regeneration, and new vessel formation, which gives the tissue a reddish, granular look. After 2 to 3 weeks, collagen undergoes remodeling, involving synthesis and degradation, with fibrils aligning along tension lines, which can last for months to years. Smoking disrupts this healing process by inhibiting fibroblast activities, including chemotaxis, migration, and proliferation, and reduces collagen production. Only 3 unsuccessful outcomes were observed in our investigation, all identified in smokers. 19 Smoking significantly hampers blood supply and neovascularization in the graft area, ultimately leading to rejection.
Conclusion
The TriCelluFuse technique combines fascia lata, fat tissue, and diced septal cartilage. It is a secure and reliable method for closing NSPs, has a significant success rate, and should be considered a viable option for people with nasal septal perforations.
Footnotes
Author Contributions
All authors contributed to the planning, design, literature survey, experiment, and active intellectual support.
Availability of Data and Materials
All data for this study are presented in this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the University of Health Sciences, Prof. Dr. Cemil Taşçioğlu City Hospital Ethic Committee (23.05.2022, E-48670771-514.99).
Informed Consent
The study was designed as a retrospective study. All patients signed written informed consent.