
Abstract
Although definitive chemoradiation (CRT) has been used for locally advanced laryngeal cancer for more than 2 decades, studies focusing on CRT failures in advanced laryngeal cancer are scarce. In this study, we aimed to determine the failure patterns and the survival outcomes in the patients who had recurrence after concurrent CRT for laryngeal cancer. Clinical records of the patients who had definitive concurrent CRT for laryngeal cancer between 2001 and 2014 at a tertiary referral center were reviewed. The end points of the study were 1-, 2-, and 3-year overall survival (OS) and disease-specific survival (DSS).In our results, there were 48 failures and the mean time period from the first diagnosis of disease to the diagnosis of recurrence was 18.0 months (range 2-72; standard deviation: 15.6). The most common recurrence pattern was local recurrence in 21 (47.9%) patients followed by regional recurrence in 11 (22.9%) patients. The 1 and 3 years OS rates were 41.7%, and 19.2% for the entire cohort, and 64.5%, and 29.7% for the patients who had not systemic recurrence at presentation of recurrence, respectively. The 1 and 3 years DSS rates were 43.5%, and 20.0% for the entire cohort, and 69.0%, and 31.8% for the patients who had not systemic recurrence at presentation of recurrence, respectively. All patients who had systemic recurrence initially (n = 13) died within 9 months (median = 4 months, range: 1-9 months). This study reveals that survival outcomes are unfavorable in the CRT failures and careful patient selection is critical to minimize failures. In the presence of systemic recurrence, disease course is aggressive.
Introduction
Total laryngectomy (TL) has been the standard treatment in locally advanced laryngeal cancer until early 90s. However, it is shown that chemoradiotherapy (CRT) is a good treatment alternative in selected locally advanced laryngeal cancer cases and the reported laryngeal preservation rates are high when patients are selected properly. 1,2 The studies on medical treatment of locally advanced laryngeal cancer are usually focusing on laryngeal preservation and survival rates. For all that, studies focusing on failure patterns and oncological outcomes in CRT recurrences are very limited. In this study, determination of failure patterns and survival outcomes in CRT recurrences are aimed.
Materials and Methods
The medical records of the patients who had concurrent CRT for laryngeal cancer between 2001 and 2014 at our institution were reviewed and the patients who had recurrent disease were included. All of the patients had weekly cisplatin-based chemotherapy as radiosensitizer during radiotherapy (RT). Exclusion criteria were history of any other head and neck cancer, previous history of any malignant disease other than squamous cell carcinoma histology, presence of distant metastasis at the time of first diagnosis and diagnosis of a second primary cancer during staging procedure.
The demographic characteristics of the patients, the time interval from the first diagnosis to the diagnosis of the recurrence, the recurrence patterns, the treatments for recurrences, and the follow-up data were recorded.
The Primary Treatment
The patients were treated with 6 MV photon beam using intensity-modulated RT or 3-dimensional conformal technique. The larynx, bilateral neck, and bilateral supraclavicular fossae were targeted. The aimed RT dose to the primary site was 7000 cGy, to N+ neck was 6600 cGy, and to N0 neck was 5000 cGy. The dose was delivered 5 days per week with once daily fraction of 200 cGy. The therapy was considered as completed if total delivered dose to larynx exceeded 6000 cGy. If total delivered dose to the primary was 6000 cGy or less, the treatment was considered as uncompleted.
During RT, patients had either 35 mg/m2 cisplatin (CDDP) or 20 mg/m2 cisplatin and 20 mg/m2 docetaxel on weekly basis as radiosensitizer. Concomitant CRT was started 3 weeks after the completion of neoadjuvant chemotherapy in patients who had induction chemotherapy. In our clinical practice, induction chemotherapy is preferred at patients with high tumor volume to predict the RT response. The patients who had neoadjuvant chemotherapy had 35 mg/m2 CDDP weekly, during induction and during concomitant CRT.
All patients had meticulous medical follow-up after completion of the treatment protocol. Besides regular outpatient visits for every 2 months during the first year with decreasing frequency in the next years, magnetic resonance imaging was also obtained every 3 months for the first 2 years and every 6 months after 2 years. When a suspicion arise regarding recurrence, examination, and biopsy under general anesthesia was done and positron emission tomography (PET)—computed tomography (CT) was obtained.
Recurrent Tumors
All the recurrent tumors were staged according to the seventh edition of the Union for International Cancer Control TNM staging manual. After detection of the recurrence, either CT or magnetic resonance imaging scans were obtained for the evaluation of the primary and the neck, and a PET/CT was used for the detection of any systemic metastasis. All patients were treated medically and/or surgically according to the patients’ clinical status and their preference. The end points of the study were 1, 2, and 3 years overall survival (OS) and disease-specific survival (DSS). The OS and DSS rates were calculated for the entire cohort and the patients who had no systemic recurrence at presentation of recurrence. The time of diagnosis of recurrence were taken into account during survival analyses, so the survival outcomes were evaluated from the date of recurrence. The Kaplan-Meier method was used to analyze the survival outcomes. For statistical analyses, SPSS version 17.0 for windows was used.
Results
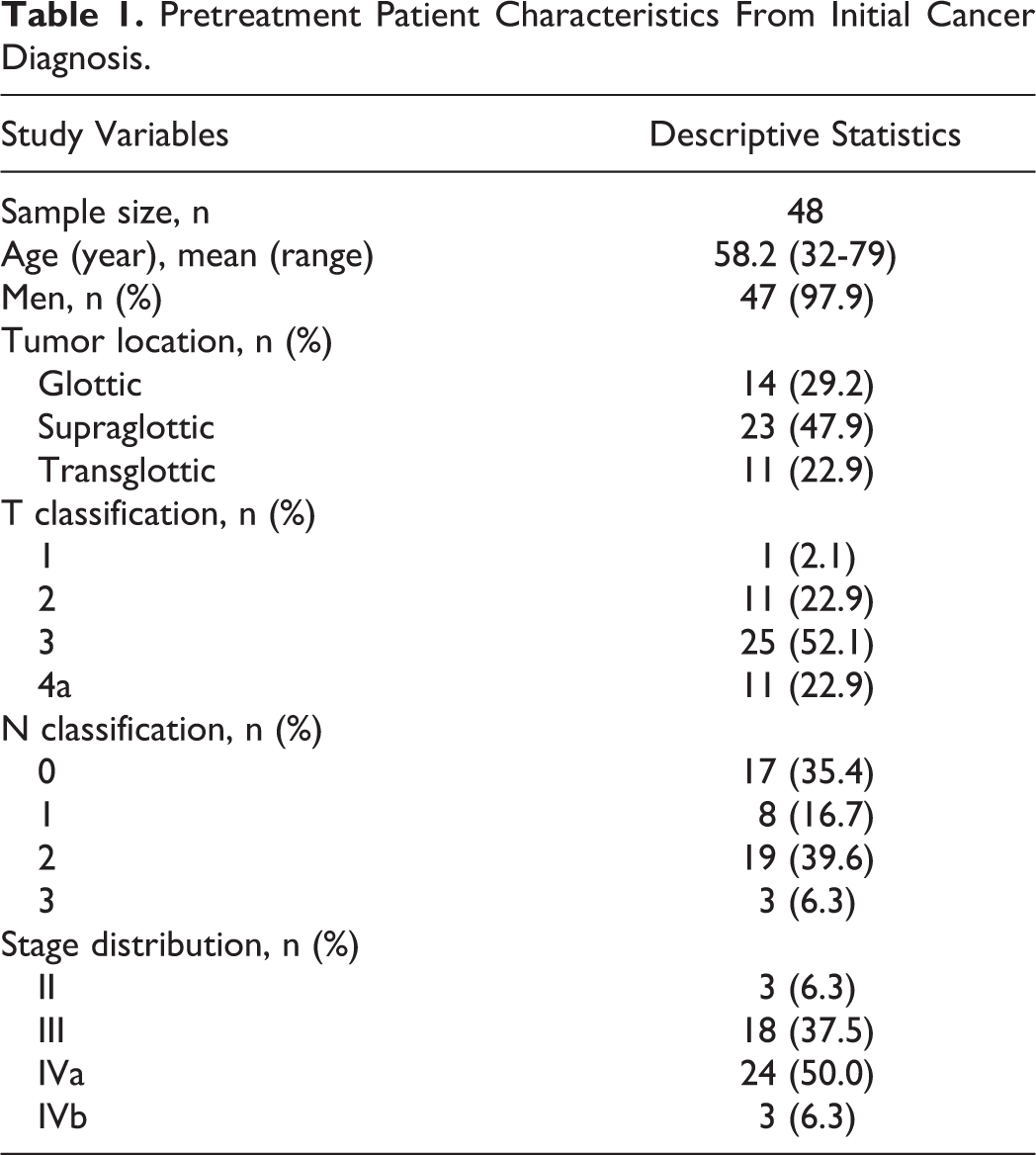
There were 48 CRT failures and the mean follow-up period was 34.7 months (range 8-110 months; standard deviation [SD]: 23.3 months). During the study period, there were 169 patients who had definitive concurrent CRT for laryngeal cancer. Pretreatment baseline characteristics of the patients from initial cancer diagnosis are given in Table 1. There were 13 (27%) patients who had induction chemotherapy before concurrent CRT. Partial or complete response was observed in these patients after induction therapy. Forty-three of the 48 patients completed the previously planned concurrent CRT protocol and had 6600 to 7000 cGy RT together with cisplatin but 5 of the patients could not. Two of these 5 patients had 4000 cGy, and the other 2 had 5000 cGy and discontinued because of the side effects. One patient had full dose RT but could not have concurrent chemotherapy in last 3 weeks. The mean time period from the first diagnosis of the disease to the first diagnosis of recurrence was 18.0 months (range 2-72; SD: 15.6). Initial recurrence patterns were as follows: local recurrence in 21 (47.9%) patients, regional recurrence in 11 (22.9%) patients, systemic recurrence in 8 (16.6%) patients, locoregional recurrence in 3 (6.3%) patients, local and systemic recurrences in 3 (6.3%) patients, locoregional and systemic recurrences in 2 patients (4.2%; Figure 1).
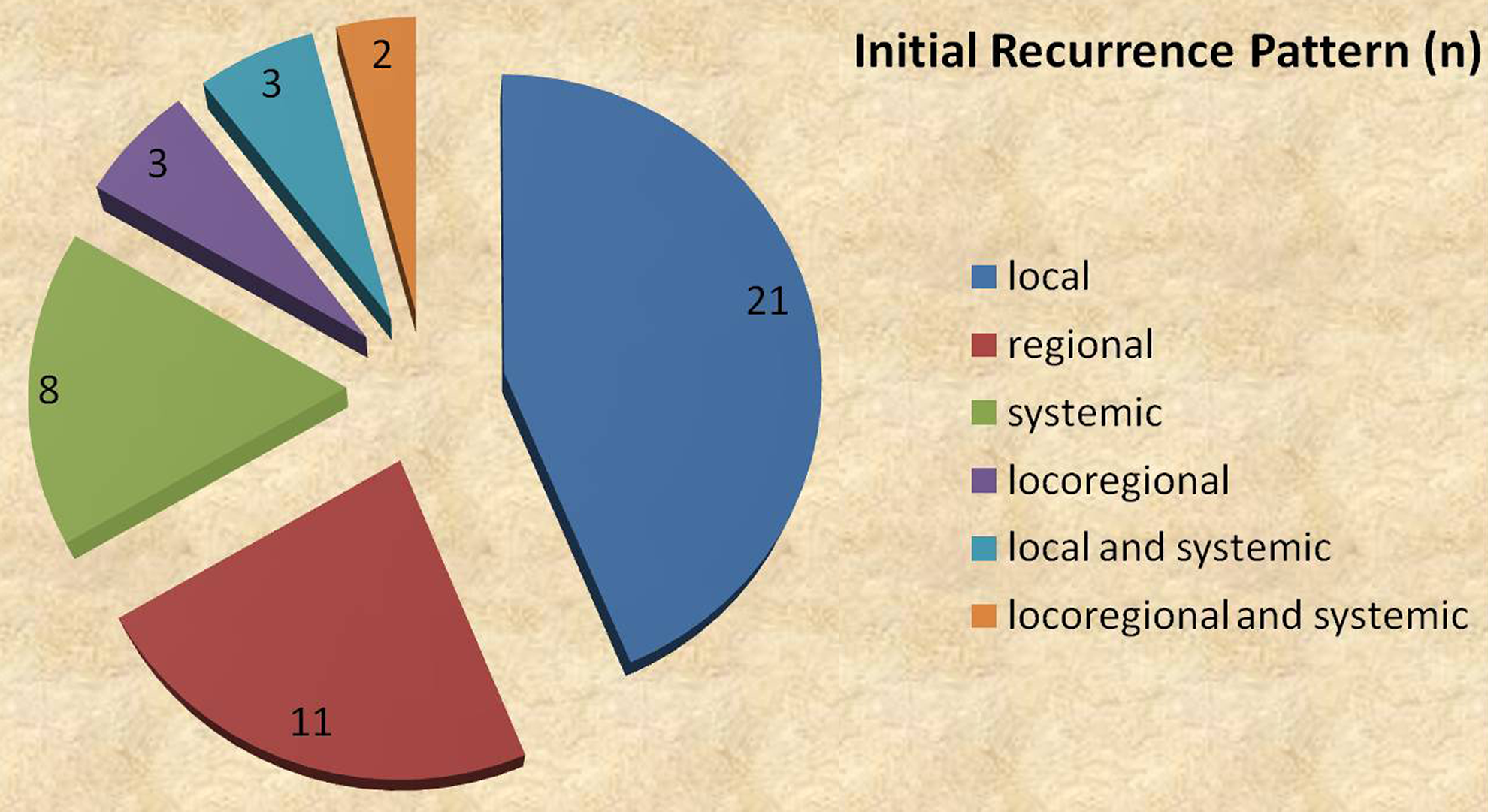
Patterns of recurrence at first presentation of recurrence.
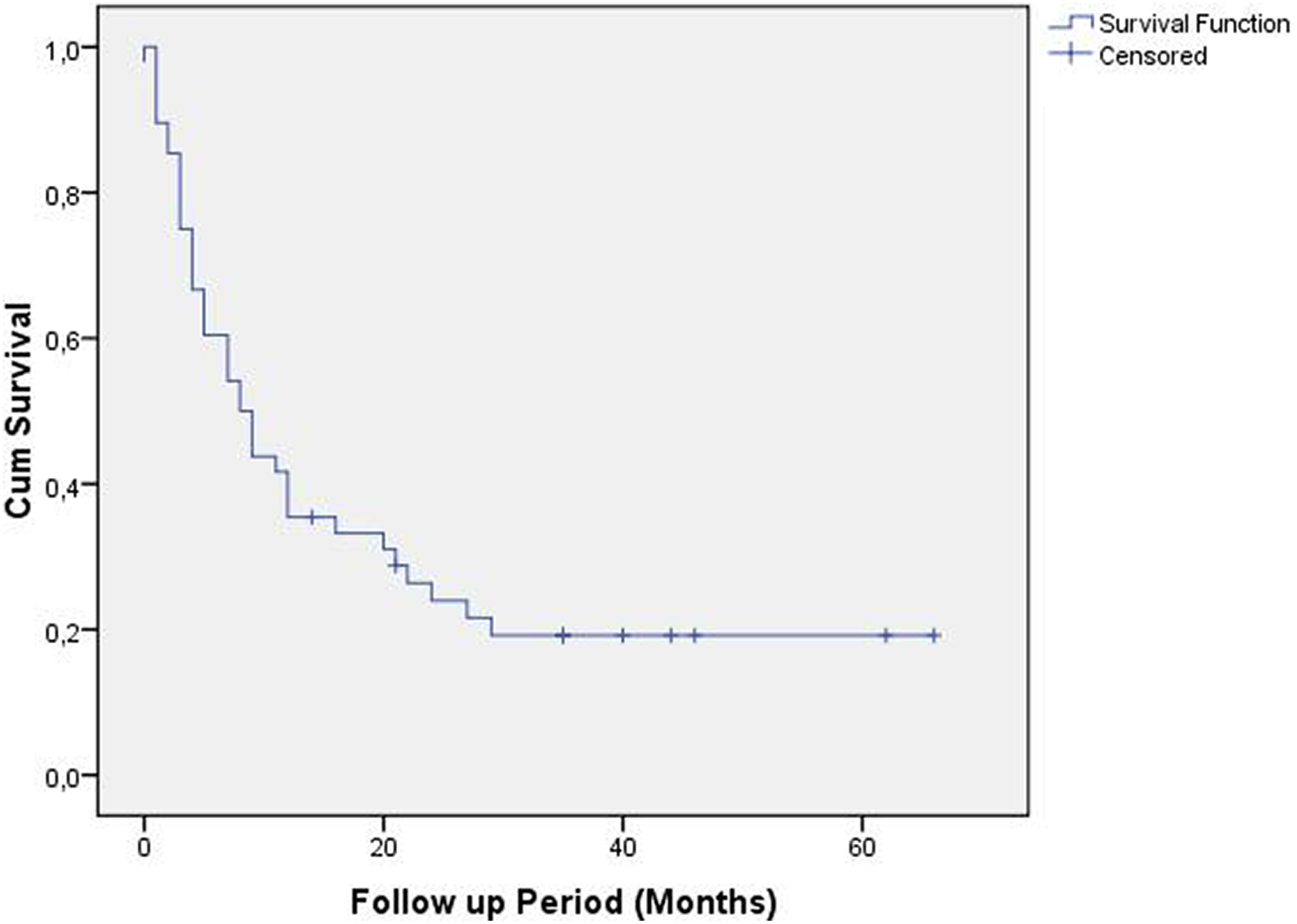
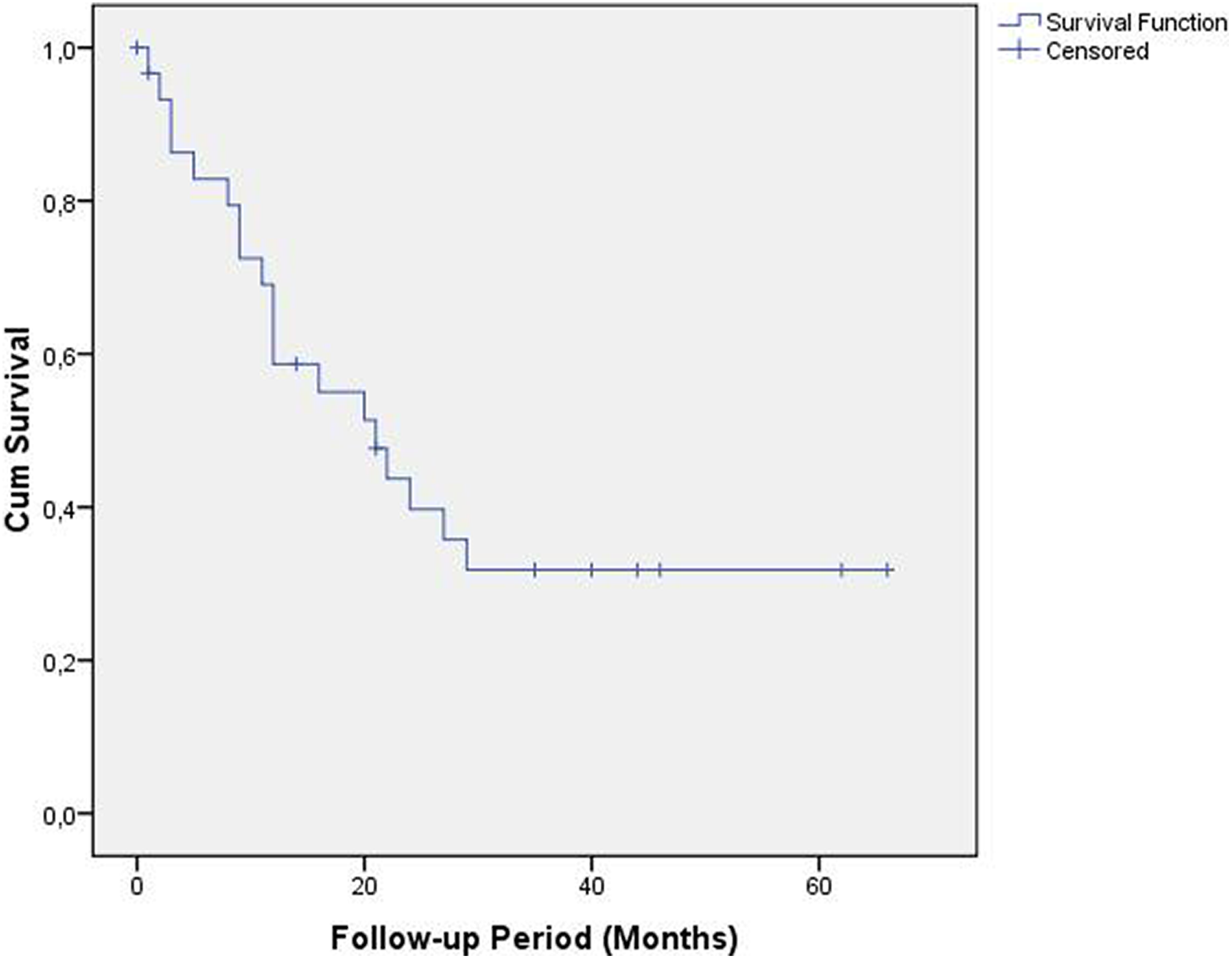
Overall survival for the entire cohort.
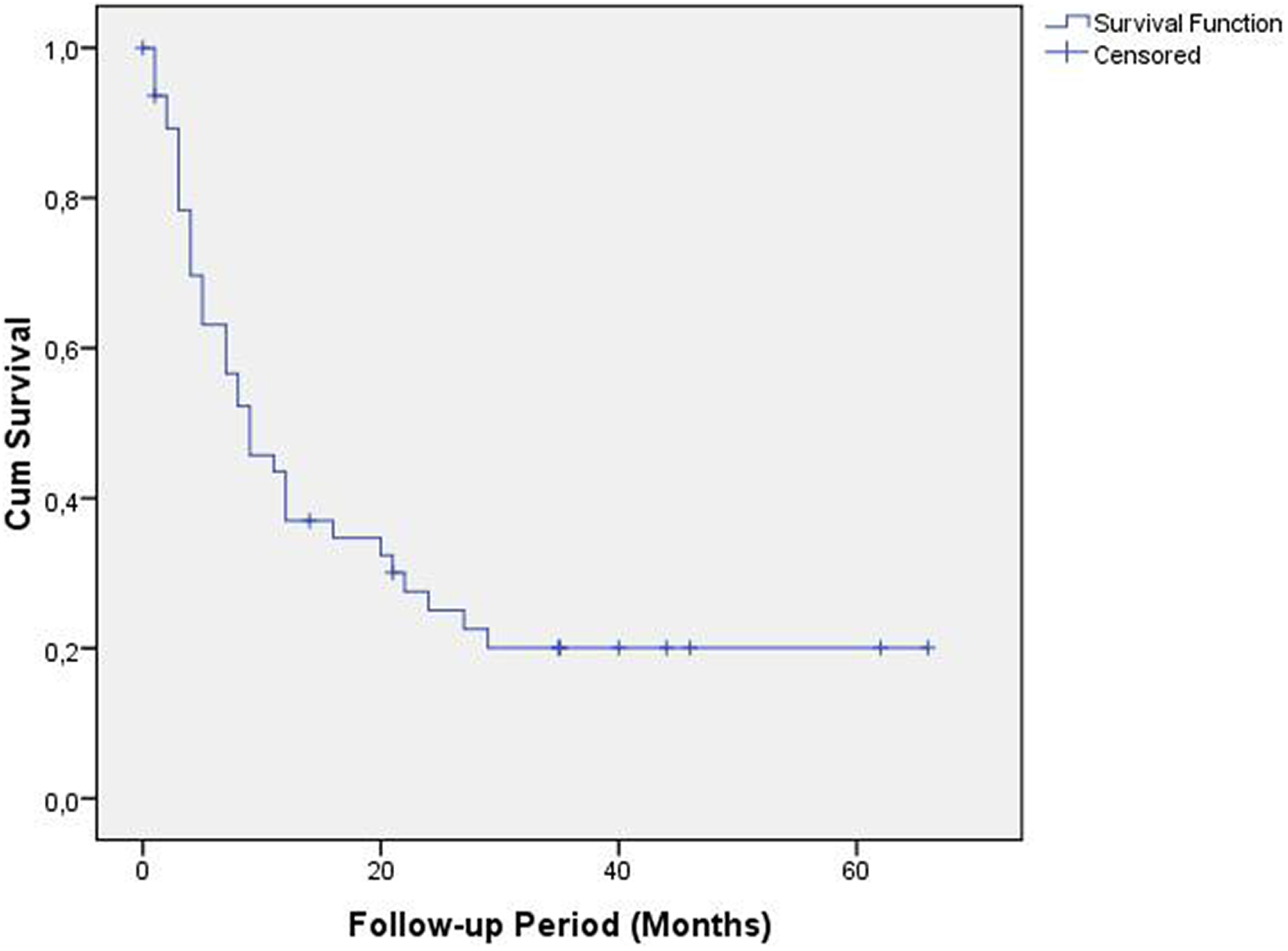
Disease-specific survival for the entire cohort.
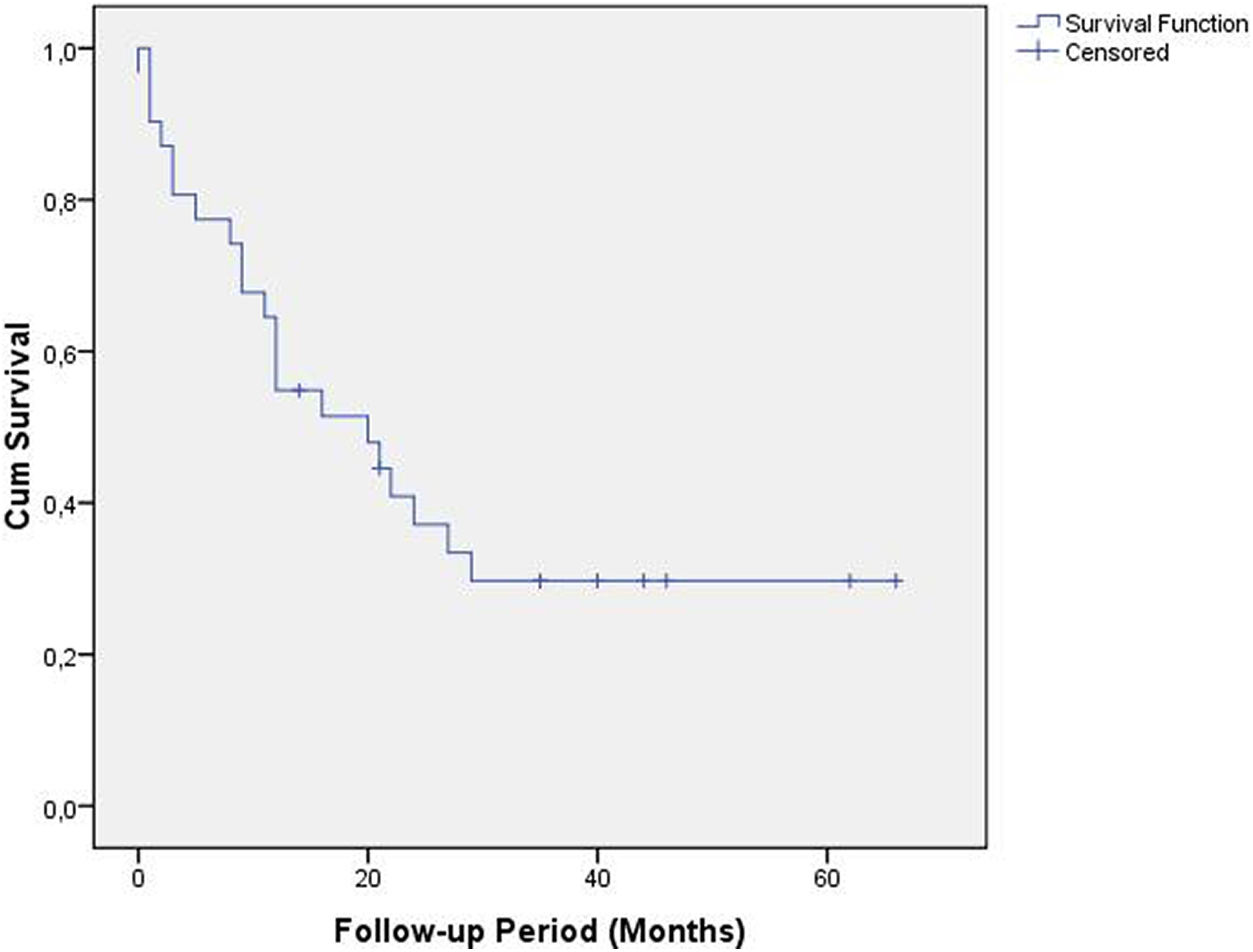
Overall survival for patients who had not systemic recurrence at presentation of recurrence.
Disease-specific survival for patients who had not systemic recurrence at presentation of recurrence.
Pretreatment Patient Characteristics From Initial Cancer Diagnosis.
Early recurrences are in fact persistent disease and a reasonable tumor-free time period should be completed to call a failure as a recurrence. In this cohort, there were 7 early failures. One of these patients experienced a failure on the first follow-up visit (2 months after the completion of the CRT), 4 of them on the fourth month and 2 patients on the fifth month. Three of these patients had systemic failure, 3 had local, and 1 had loco-regional. Three patients diagnosed with systemic recurrence did not have a detected systemic disease initially so that we cannot call this situation as a persistent disease. Probably these patients had occult systemic disease initially. Early failures were not excluded to protect the integrity of the study.
All patients but 5 (30/35, 85.7%), who presented with local and/or regional recurrence, underwent radical salvage surgeries. Four patients with only local recurrence and 1 patient with only regional recurrence had palliative platinum-based chemotherapy because of either patient preference or presence of unresectable tumor. Two patients with local recurrence had partial laryngectomy and all other patients had total laryngectomy. Neck recurrences were treated by either radical or modified radical neck dissections.
All of the 13 patients who had systemic recurrence at presentation had systemic platinum-based chemotherapy and did not have surgeries. Patients who experienced progressive disease despite of radical surgery for recurrent disease also had systemic platinum-based chemotherapy. Thirty (86%) of the 35 patients who did not have a systemic recurrence undergone a salvage surgery, total laryngectomy, and/or neck dissection, according to the site of recurrence but 5 (14%) of the patients had only palliative chemotherapy. Thirty (63%) of the patients had a radical surgery for curative intent in the entire cohort.
Thirteen (61.9%), and 6 (28.6%) of the patients who had only local recurrence initially were alive after 1 and 2 years follow-up, respectively. Six (54.5%), and 5 (45.5%) of the patients who had only regional local recurrence initially were alive after 1 and 2 years follow-up, respectively. Regardless of being simultaneous or not, none of the patients (n = 8) who had local and regional recurrence together could survive beyond 27 months and the median survival time was 16 months (range 3-27 months). All patients who had systemic recurrences initially (n = 13) died within 9 months (median = 4 months, range 1-9 months).There were 2 patients who died due to cardiac disease. At that time, they were tumor-free after salvage laryngectomy.
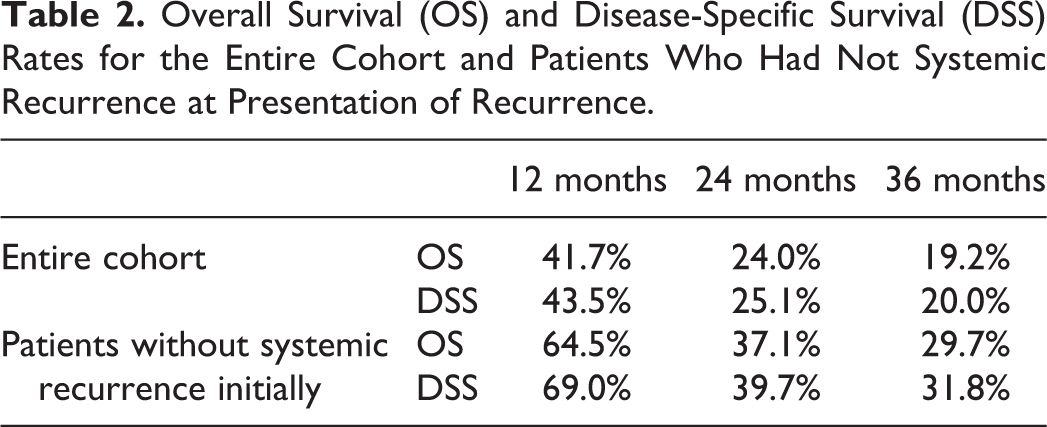
The 1 and 3 year OS rates were 41.7%, and 19.2% for the entire cohort, and 64.5%, and 29.7% for the patients who had not systemic recurrence at presentation of recurrence, respectively(Figures 2 -5 and Table 2).
Overall Survival (OS) and Disease-Specific Survival (DSS) Rates for the Entire Cohort and Patients Who Had Not Systemic Recurrence at Presentation of Recurrence.
Discussion
Management of advanced laryngeal cancer comprises 2 main options: surgery and CRT. In the past, TL was the standard treatment; however, treatment strategies continue to evolve and organ preservation is an important goal without sacrificing locoregional control in modern practice. Open partial laryngectomy and even endolaryngeal laser surgery can be used in some selected advanced cases. There are many studies regarding supracricoid laryngectomy with high-local control rates in the literature. 3 -5
As a second alternative, definitive CRT has been used for locally advanced laryngeal cancer for more than 2 decades. Although sequential treatment protocols were used initially in 90s, concurrent schemes became more popular after RTOG 91-11 trial. 1 According to many previous reports, the local control and the survival rates are highly satisfactory when patients are selected appropriately. 2,1,6 On the other hand, the survival outcomes in CRT failures are not well-studied and there are only a few available retrospective studies comprised of limited number of patients. In our study, 3-year OS rate was 30% and survival outcomes are similar according to the studies on this issue. Van der Putten et al reported 35% 5-year disease-free control rate, 27% OS rate, and 35% DSS rate in their study comprised of 60 patients. 7 There were both laryngeal and hypopharyngeal patients with cancer in this study. Median survival was 12 months for the 38 patients who were not suitable for salvage surgery. Patients in whom the tumor was controlled had a 5-year OS of 70%. Leon et al reported 38% 5-year survival for 42 patients who had local and/or regional recurrence after sequential CRT for locally advanced laryngeal cancer. 8 A total of 67% of patients with advanced laryngeal carcinoma treated with induction chemotherapy and RT were candidates to salvage surgery and 5-year survival rate for the 28 patients treated with salvage surgery was 57%. Tan et al and Esteller et al reported similar results but the number of the laryngeal cancer patients in these 2 studies are relatively low. 9,10
The reasons of low oncological outcome in this patient group could be grouped as tumor-related, treatment-related, and patient-related. Probably, the cancer cells survived after an intensive CRT protocol have more aggressive biological behavior. It was shown that the recurrent tumors are often understaged, present with multiple tumor foci, and invades perineural space more frequently. 11 Reirradiation without significant morbidity is not possible in most cases and resistance to chemotherapy and RT should be expected since these did not work previously. On the other hand, motivation, immune system, and nutritional status of the patients would not be at an optimal status. Even if a patient is eligible for a salvage surgery; difficulty in predicting tumor spread in irradiated neck and larynx, technical difficulties during surgery, possible requirement for additional reconstructions, quite high-complication rates and prolonged hospitalization periods have negative effects on oncological outcomes.
Most patients with recurrent head and neck cancer have very poor prognosis but the site of the recurrent disease has a great impact on the success. Patients with a recurrent laryngeal cancer who underwent TL may have better chance to survive when compared to recurrences in other head and neck sites. 12 Every effort should be made to salvage in case of resectable recurrent disease in the larynx and/or the neck. Since reirradiation is not possible and brings along severe complications and even mortality, surgery is the single treatment option in this cases if cure is aimed. Salvage surgery is not a reasonable option in recurrent head and patients with cancer with systemic metastasis since life expectance is not long in this patient group.
Although results of this study provide valuable survival data, there are also some limitations. The first limitation of this study is lack of data about wound infection, laryngocutaneous fistula, hospital stay, and other morbidities. Since the aim of this study was determination of survival data in this unique patient group, we did not focus on these issues. Other limitations were relatively small sample size and retrospective and descriptive nature of the study. However, these patients form a very complicated group that all the head and neck surgeons struggle to deal with and concrete data about the survival outcomes in this patient group are limited. For those reasons, we believe that the results we have given in this study may help head and neck surgeons to predict the survival and inform the patients at the beginning of the treatment modality selection process and at the time when recurrence has detected. In this study, we have shown that even short term OS and DSS rates are quite low. According to these results, therapeutic interventions are not highly successful in most cases and efforts should be focused on careful patient selection to reduce failure rates. According to our experience and the previous literature, the patients with T4a tumors, high-volume disease (massive preepiglottic and paraglottic invasion, massive subglottic disease, bulky neck disease, etc), loss of laryngeal functions (laryngeal obstruction, aspiration, and dysphagia) prior to treatment are not ideal candidates for definitive CRT 2,13,14 .
Since oncological outcomes are not favorable in recurrences after CRT, patients should be informed about this issue before making initial treatment decision after the first diagnosis of the laryngeal cancer. After diagnosis of the recurrence, the expected prognosis and the therapeutic options should be thoroughly discussed together with potential complications and changes in quality of life.
Conclusions
In the presence of systemic recurrence, disease course is very aggressive and systemic treatment is not effective. According to our results, recurrent laryngeal cancer after CRT failure has an aggressive course and therapeutic interventions are usually unsuccessful in this patient group. Careful patient selection has utmost importance to reduce failure rates.
Footnotes
Authors’ Note
All of the above listed authors contributed to design of this review paper, review of the previous studies regarding this issue, writing of the manuscript, and critical revision of the paper for intellectual content. All of the above listed authors approve the final version of the manuscript and fully agree that accuracy and integrity of any part of the work are appropriately investigated and confirmed, and all questions related to these issues were resolved. This study was presented at the 7th European Congress on Head and Neck Oncology, Budapest/Hungary, September 7-10, 2016. This material has never been published and is not currently under evaluation in any other peer-reviewed publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.