
Abstract
The History of Rigid Nasopharyngoscopy
Visualization of the nasopharynx proved a challenge in the early 20th century. With few methods available to treat middle ear disease, otolaryngologists favored cannulation of the eustachian tube for dilation and insufflation of the middle ear. Still, blind passage of curved metal eustachian tube catheters often failed. Some tried transoral visualization of the nasopharynx with a headlight, soft palate retractor and small angled mirrors, but this provided only a limited view.
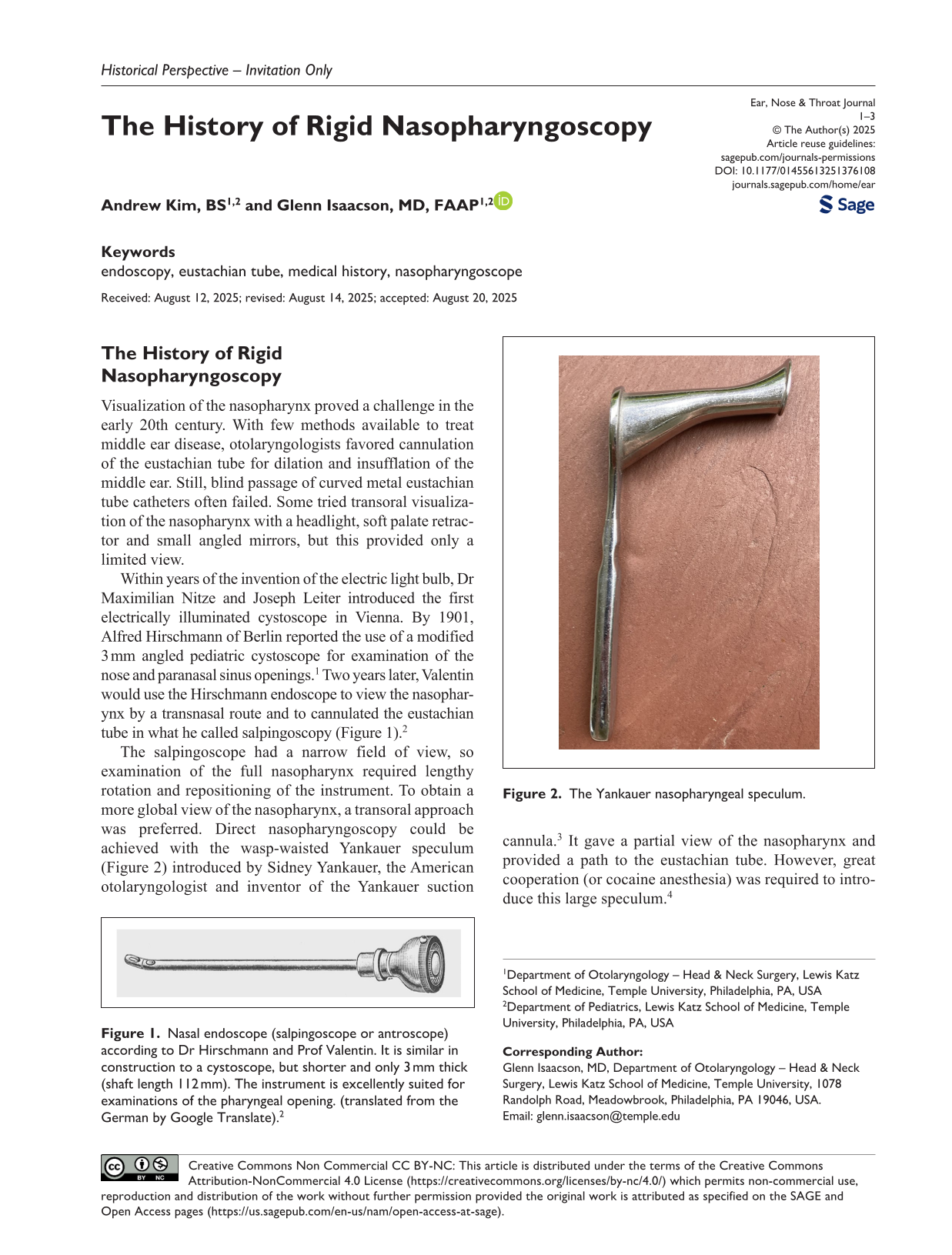
Within years of the invention of the electric light bulb, Dr Maximilian Nitze and Joseph Leiter introduced the first electrically illuminated cystoscope in Vienna. By 1901, Alfred Hirschmann of Berlin reported the use of a modified 3 mm angled pediatric cystoscope for examination of the nose and paranasal sinus openings. 1 Two years later, Valentin would use the Hirschmann endoscope to view the nasopharynx by a transnasal route and to cannulated the eustachian tube in what he called salpingoscopy (Figure 1). 2
Nasal endoscope (salpingoscope or antroscope) according to Dr Hirschmann and Prof Valentin. It is similar in construction to a cystoscope, but shorter and only 3 mm thick (shaft length 112 mm). The instrument is excellently suited for examinations of the pharyngeal opening. (translated from the German by Google Translate). 2
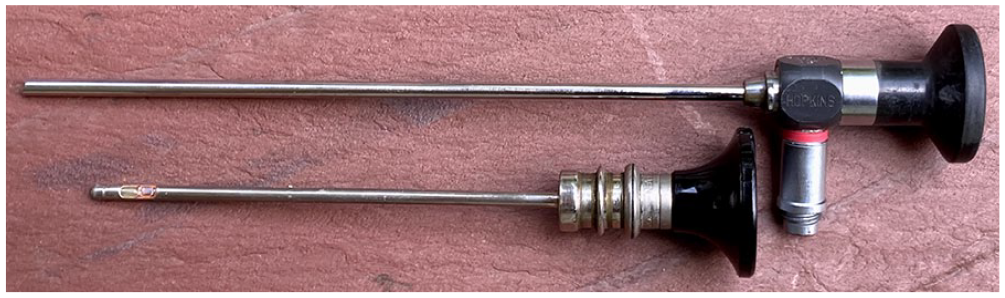
The salpingoscope had a narrow field of view, so examination of the full nasopharynx required lengthy rotation and repositioning of the instrument. To obtain a more global view of the nasopharynx, a transoral approach was preferred. Direct nasopharyngoscopy could be achieved with the wasp-waisted Yankauer speculum (Figure 2) introduced by Sidney Yankauer, the American otolaryngologist and inventor of the Yankauer suction cannula. 3 It gave a partial view of the nasopharynx and provided a path to the eustachian tube. However, great cooperation (or cocaine anesthesia) was required to introduce this large speculum. 4

The Yankauer nasopharyngeal speculum.
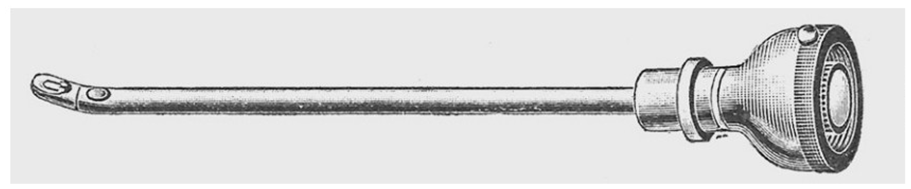
In 1909, Harold Hays devised an alternative to direct transoral nasopharyngoscopy. Built by R. Wappler of Wappler Electrical Engineering Co (New York City, NY), the Hays pharyngoscope (Figure 3) included a horizontal shaft containing the lamps, lenses and a 90° mirror. The shaft acted as a tongue depressor while an illuminated mirror provided a panoramic view of the nasopharynx. 5
The Hays pharyngoscope and its method of insertion.
Meanwhile, others worked to advance the transnasal approach. Edgar M. Holmes in Boston modified a female cystoscope, which he sold as the Holmes’s Electric Nasopharyngoscope. 6 Holmes designed an integrated wire cotton applicator to apply cocaine, adrenalin, and a 15% solution of argyrol (a popular disinfectant) to the eustachian tube for the treatment of acute otitis media. When radium treatment of the adenoids later became popular, insertion of the radiation probe was facilitated by rigid nasopharyngoscopy. To document the effects of radiation, Captain John E. Hendricks of the U.S. Army Medical Corps attached a camera to the nasopharyngoscope with a series of adaptors. 7
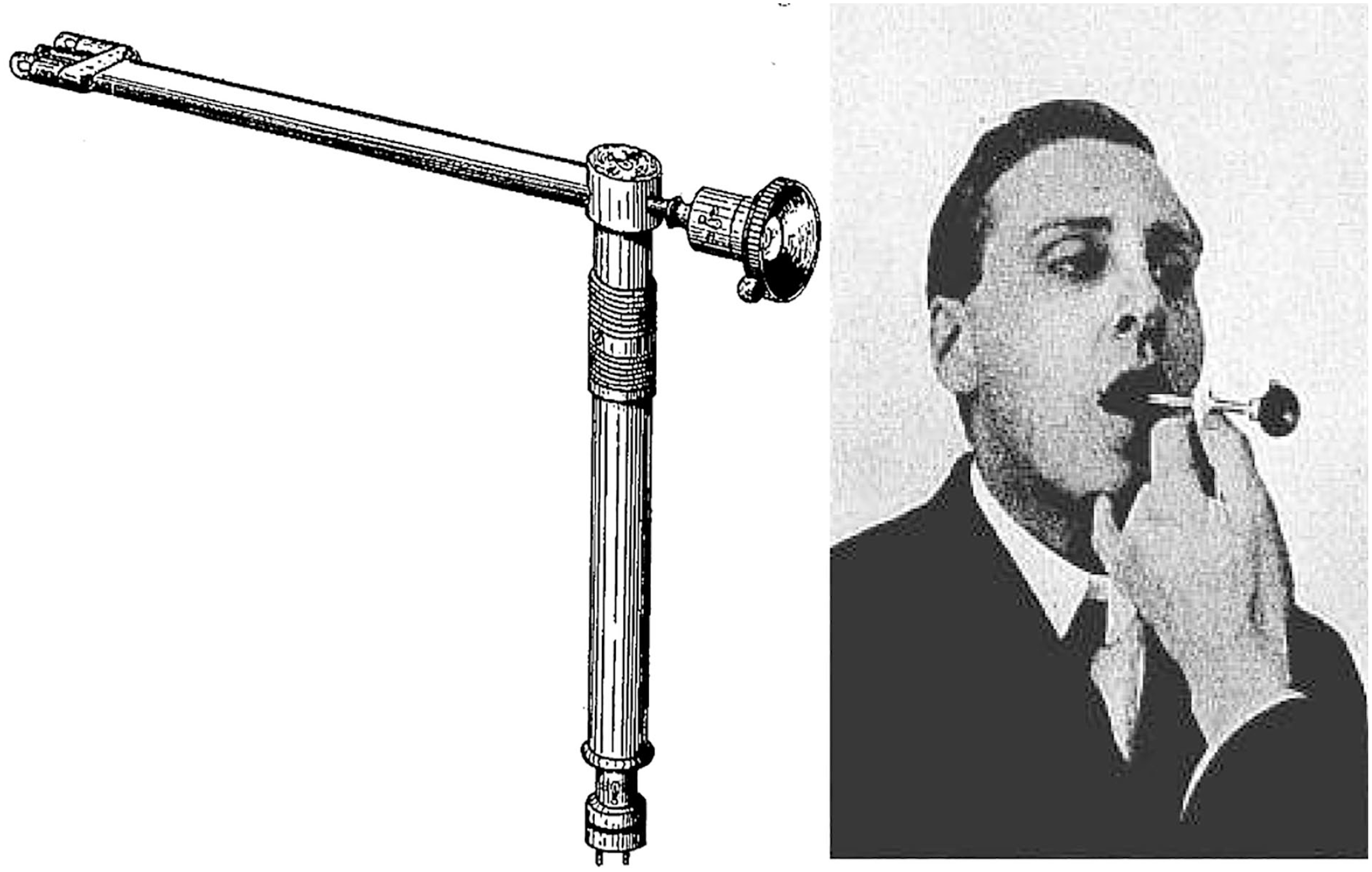
Despite all these advances, image quality remained poor. Distal incandescent illumination limited visual detail, as brighter bulbs produced too much heat to allow for lengthy examination or treatment. Moreover, the standard biconvex lenses in these modified cystoscopes were subject to errors of field curvature and astigmatism, especially when fitted in a narrow tube (Figure 4).
Above, a 30° Hopkins rigid rod endoscope with glass-rod lenses and “cold” fiberoptic illumination. Below – a National-Fontar rigid nasopharyngoscope, circa 1950 by National Electric Instruments (Elmhurst, NY, USA). It used conventional biconcave lenses and was illuminated by a distal electric light bulb.
To address these limitations, Harold Hopkins, the British physicist and mathematician, employed 2 brilliant innovations. He filled the shaft of the endoscope with a series of strongly refracting glass-rod and meniscus lenses. (UK patent 1959, No 954629). The rod lenses lost less light than did air and increased the field of view. The meniscus lenses corrected chromatic aberration. Next (1960), 8 in cooperation with the Karl Storz Company (Tuttlingen, Germany), Hopkins surrounded the endoscope’s central shaft with light-conducting glass fibers. This incoherent fiberoptic illumination delivered strong distal light while keeping the heat source far removed from the patient. High-resolution rigid nasopharyngoscopy was born.
Footnotes
Ethical Considerations
This article does not contain any studies with human or animal participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
This article contains no new data. All data included are available through conventional library sources. The authors would be pleased to assist interested researchers via the corresponding author’s email.