
Abstract
We present a case of a 49 year-old male who suffered from a homicide attempt with a crossbow arrow, resulting in a retained foreign body through his mandible, pterygoids, nasopharynx, and parotid gland. The patient was being managed conservatively with antibiotics to manage symptoms of recurrent infections prior to transfer to our center. The patient developed worsening congestion, foul drainage from the arrow exit wound, as well as developing worsening facial pain. The Head and Neck Oncology, Rhinology, as well as the Neurointerventional radiology services collaborated in a case for the subsequent safe removal of the crossbow arrow. The patient recovered well 3 months post-operatively with improvement in his pain and nasal symptoms.
Introduction
Penetrating injuries of the head and neck account for a minority of trauma cases in the United States. 1 These incidents tend to have a high mortality rate due to the vital importance of the neurovascular structures contained within this anatomic region. 2 Injuries with crossbow arrows to the head and neck have been previously described; however, to our knowledge, there has not been any case described of a patient living with a retained crossbow arrow for a 1-year period prior to removal.3,4 We present a case describing the complexity of care and the multidisciplinary approach required for appropriate and safe removal.
Case Presentation
A 49-year-old male presented as an outpatient to the Rhinology clinic at our institution as a referral for nasal obstruction in the setting of a foreign body coursing through the nasopharynx. The patient had been assaulted while driving about 1 year prior to evaluation in our clinic with a stray crossbow arrow, resulting in a retained fragment coursing through his head. The patient was managed conservatively prior to being evaluated at our institution due to concern for proximity to neurovascular structures. The patient had been doing well; however, he had been suffering from increasingly frequent infections resulting in purulent drainage from his left facial wound and nasal purulent drainage, as well as requiring treatment with multiple courses of antibiotics. He reported a Nasal Obstruction Symptom Evaluation (NOSE) score of 100/100 and a Sino-Nasal Outcome Test (SNOT-22) score of 102/110. He reported severe nasal obstruction and a constant foul smell, as well as persistent facial and otic discomfort. As such, he was interested in an intervention to remove the retained crossbow arrow. On examination patient had left-sided numbness along V1 to V3 and a noted wound along his left cheek overlying his parotid gland (Figure 1). His facial nerve exam was normal. Nasal endoscopy demonstrated thick mucus pooling in the nasopharynx with the metal object transversing the nasopharynx.

Left preauricular skin with a 2 cm raised erythematous chronically inflamed wound with purulent drainage at the site of the crossbow arrow exit.
Computed tomography demonstrated the arrow fragment measuring 12 cm through the left mandibular notch, coursing through the nasopharynx in a posterolateral direction and terminating posterior to the right mandibular condyle (Figure 2). Fractures of the posterior left zygomatic arch and left lateral pterygoid were also noted.

Computed tomography axial slice demonstrating trajectory of the crossbow arrow.
Given the complexity of the patient’s presentation and his recurrent infections, a multidisciplinary approach was taken to ensure safe removal of the foreign body. Physicians from different teams were involved in the care of the patient to include a head and neck oncologic surgeon, as well as a neurointerventional radiologist. Preoperative angiography with interventional radiology confirmed no vascular injury to the internal and external carotid artery systems, with noted stable incidental aneurysms small saccular aneurysm at the left middle cerebral artery bifurcation, as well as a small aneurysm of the right terminal internal carotid artery. The patient underwent embolization of the left internal maxillary artery due to proximity to the shaft of the arrow.
The patient was taken to the hybrid interventional radiology operating room on the following day with a head and neck surgeon, a rhinologist, and an interventional neuroradiologist. The patient was induced with general endotracheal anesthesia. The image guidance navigation system, as well as the peripheral nerve monitoring system, were set up and confirmed to be working. The patient was prepped in a sterile fashion and draped appropriately. The initial phase of the surgery involved achieving appropriate visualization of the nasopharynx with appropriate decongestion using epinephrine-soaked pledgets. A posterior septectomy was then performed to achieve adequate exposure of the nasopharynx.
At this point, the head and neck surgery team performed their portion of the case. A wide local excision was performed to include the area of the skin involved with the foreign body skin reaction. Afterward, a neck dissection was performed on the left side to identify the internal jugular vein, as well as both the internal and external carotid artery, which were marked with vessel loops. A superficial parotidectomy was then performed, and identification of the facial nerve branches was completed (Figure 3). The crossbow arrow was noted to be between the buccal and zygomatic branches, which were reflected superiorly and inferiorly. Subsequently, the masseter was resected along the superior and inferior aspects of the crossbow arrow to expose the condylar process.
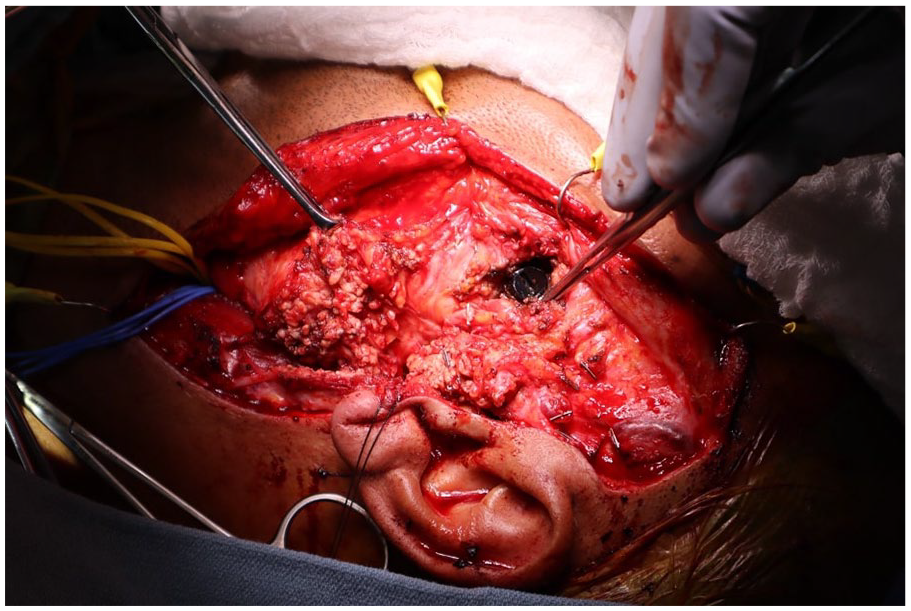
Crossbow arrow visualized after superficial parotidectomy and neck dissection.
Once adequate exposure was achieved, a nasal endoscopy was introduced into the nasopharynx to allow for endoscopic visualization (Figure 4). The interventional radiology team was on standby with access via the right femoral artery available in case of intervention for bleeding beyond what could be controlled via the left carotid artery system. The crossbow arrow was then removed atraumatically. The nasopharyngeal cutaneous fistula created was visualized; no bleeding was noted within the nasopharynx (Figure 5). Antibiotic irrigation was performed. A fragment of the temporalis muscle was placed into the created fistula to create a plug. Endoscopic confirmation was done to ensure adequate sealing of the fistula. A #10 JP drain was placed within the neck, and the incision was subsequently closed with advancement of local tissue in multiple layers.
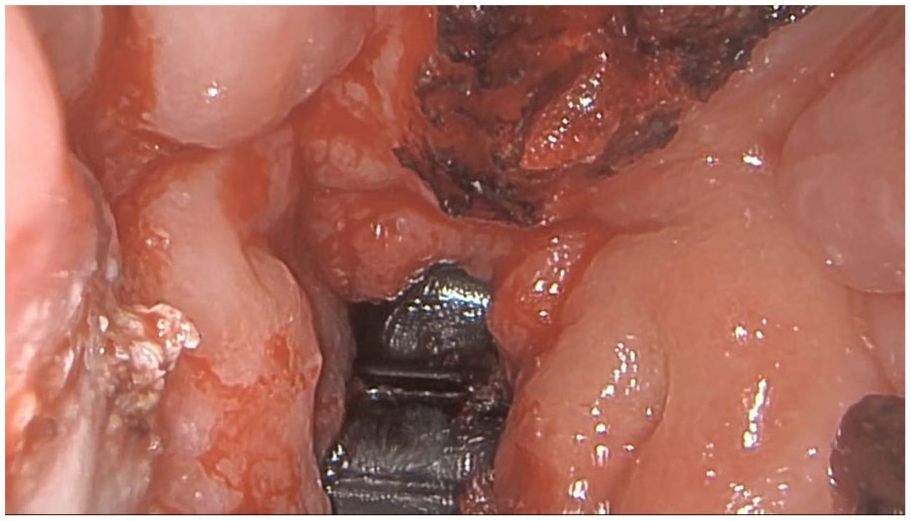
Endoscopic view of crossbow arrow in nasopharynx after posterior septectomy.
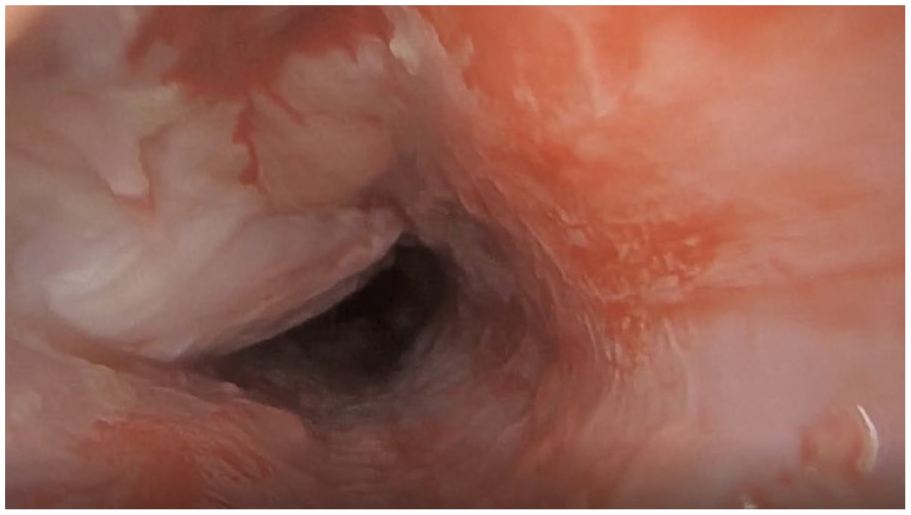
Nasopharyngeal-cutaneous fistula at site of crossbow arrow after removal as viewed from the cutaneous side into the nasopharynx.
Discussion
We present a case of a penetrating crossbow arrow injury to the head and neck. To our knowledge, this is the first case described whereby the offending foreign body has been managed beyond the acute phase of injury with complications relating to persistent infection of the involved soft tissue. Recurrent infections and repeated antibiotic treatments prompted referral to our department and subsequent coordination of care.
Penetrating injuries of the head and neck can be life-threatening in accordance with the structures involved in the path of the injury. 5 The major structures involved can include the carotid arteries, jugular veins, the pharynx, larynx, esophagus, and the skull base with adjacent injury to the brain. The combination of vital organs and critical blood supply involvement may confer a higher mortality rate. In the case presented, while the arrow was present near major branching vessels, they were not directly involved. Additionally, the skull base was spared from injury, sparing the patient from any concerns for a large cerebrospinal fluid leak or any cerebral injury.
The orientation of the arrow upon entry may also affect the structures involved. In this case presented, the patient suffered from a homicide attempt with a nearly horizontal orientation of the entry wound. Previous reports of suicide attempts with crossbows have been reported.6,7 The trajectory of these injuries tends to be vertically oriented and may cause cerebral injury and disruption of the skull base. Aside from concerns related to disruption of the skull base, special attention must be given to the management of the airway in these patients. Depending on the involved structures, mobility of the mandible may be limited, and obstruction of the pharynx may result from the retained arrow.6,8 Each modality for intubation must be evaluated, with tracheostomy being a potentially life-saving procedure for these patients.
At the patient’s 3-month post-operative follow-up, he reported improvement in his nasal obstruction, sense of smell, and facial pain. He endorsed some associated pain around the incision site along his left face and some dizziness, which continued to improve at his subsequent visits. His post-operative SNOT-22 score was 13/110 (down from 103 pre-operatively). While the original referral to our tertiary center was made through the Rhinology division for purposes of nasal obstruction, the removal would not have been possible without the surgical expertise of our Head and Neck division for a transparotid approach, and without the backup for hemorrhage control from our Neurointerventional department.
Conclusion
Penetrating injuries to the head and neck have a high risk of complications and associated mortality. We present the case of a penetrating injury and long-term sequelae associated with a crossbow arrow injury. Consideration in preparation for surgical removal must be given to potential complications, most notably vascular control in the presented case. This case highlights the importance of multidisciplinary care and collaboration that can be provided at a tertiary academic center.
Footnotes
Consent to Participate
Patient provided written consent to participate.
Consent for Publication
Patient provided written consent to allow for their case to be published.
Author Contributions
H.A.P.: writing and constructing of manuscript, compiling of images. M.W.: manuscript editing, primary neurovascular expert in case. R.F.: manuscript editing, head and neck contribution during surgical care. B.B.: manuscript editing, head and neck contributing during surgical care, and coordination of care. A.J.: manuscript editing, primary coordination of care, and rhinologist during surgical care.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.