
Abstract
Penetrating transorbital injury with skull base involvement is a rare occurrence from a crayon. We report a case of a 2-year-old male who sustained a penetrating crayon injury through the right orbit and lamina papyracea into the posterior ethmoid sinus complicated by cerebrospinal fluid leak. There have been no other reported cases of this type of injury by a crayon.
Introduction
Transorbital penetrating injuries usually occur in young children and are an uncommon subset of head trauma that require prompt multidisciplinary surgical intervention. 1,2 Although the literature is limited, most cases of penetrating orbital trauma are reported as being caused by pens, knives, and chopsticks. 3 Overall, transorbital penetrating intracranial injuries make up about 0.4% of traumatic brain injuries and have the potential to be severe with a high mortality rate. 4
Case
A 2-year-old male presented to the emergency department with a crayon embedded in his right eyelid inferior to the medial canthus after falling from his bed onto a green crayon that he was holding in his hand (Figure 1A). Computed tomography (CT) scan revealed penetrating injury in the right inferomedial orbital rim that extended through the lamina papyracea (Figure 1B) and then into the ethmoid sinus (Figure 1C), with the outside CT showing that the crayon had traversed the orbit with the tip extending to the sphenoid sinus (Figure 1D).
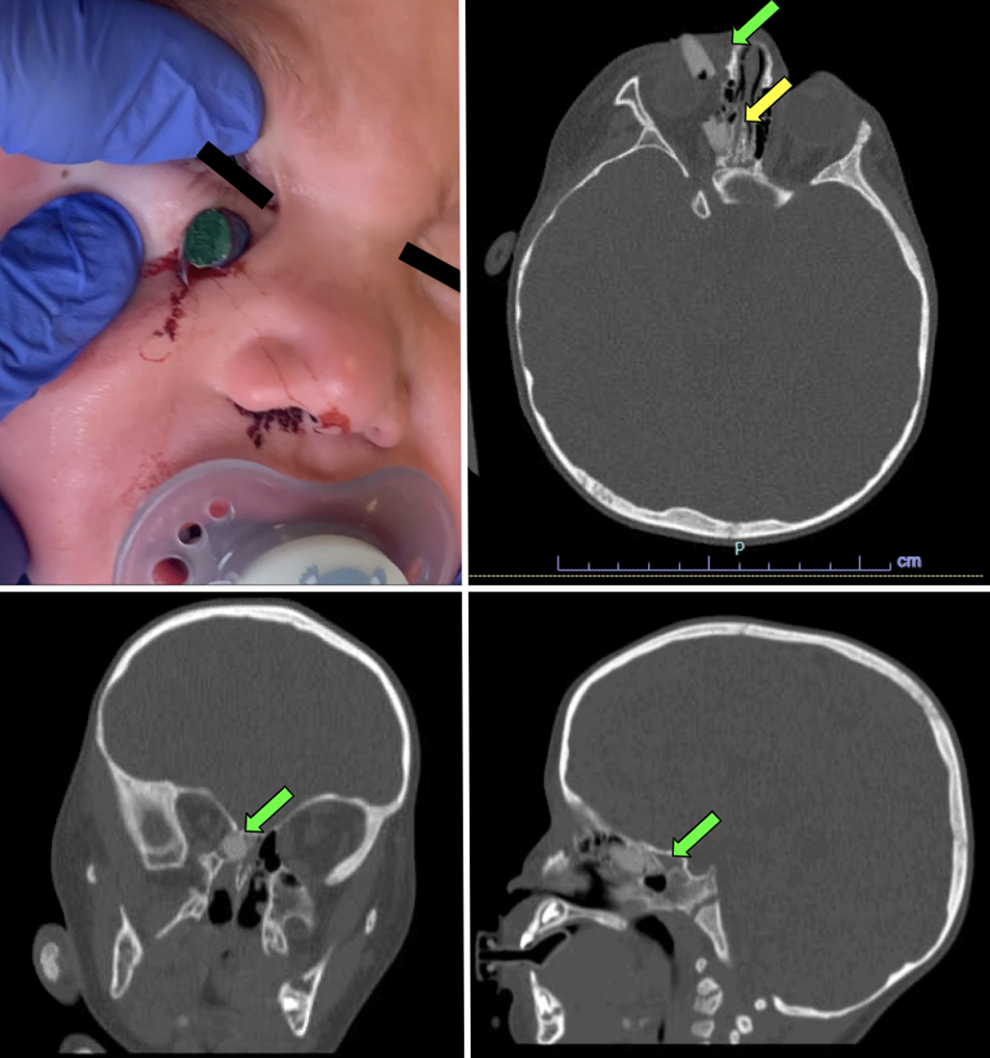
Preoperative penetrating orbital trauma. (A) Crayon seen penetrating through inferomedial eyelid. (B) Axial computed tomography (CT) scan showing crayon extending through the orbital rim (green arrow) to the lamina papyracea (yellow arrow). (C) Coronal CT showing crayon extending into ethmoid air cells, abutting the skull base. (D) Sagittal CT showing crayon fragment extending to the posterior ethmoid cells and face of the sphenoid sinus.
The patient was taken emergently to the operating room to remove the embedded crayon through a transorbital approach. Postoperative imaging showed a retained foreign body in the right posterior ethmoid abutting the face of the sphenoid sinus (Figure 2). Otolaryngology was then consulted, and the patient was taken back to the operating room for a combination endoscopic and open transconjunctival approach by otolaryngology and ophthalmology to remove the remaining foreign body. Removal was accomplished by a transorbital approach to retract the orbital contents out of the ethmoid sinus as well as an endoscopic approach to perform sphenoidotomy. The retained crayon piece was identified in the right posterior ethmoid cell and superior aspect of the sphenoid sinus and removed. Crayon wax was noted along the skull base with an adjacent area concerning for skull base dehiscence. A small cerebrospinal fluid leak was identified intraoperatively, and reconstruction was performed with Neurosurgery using a dural graft and fibrin glue.
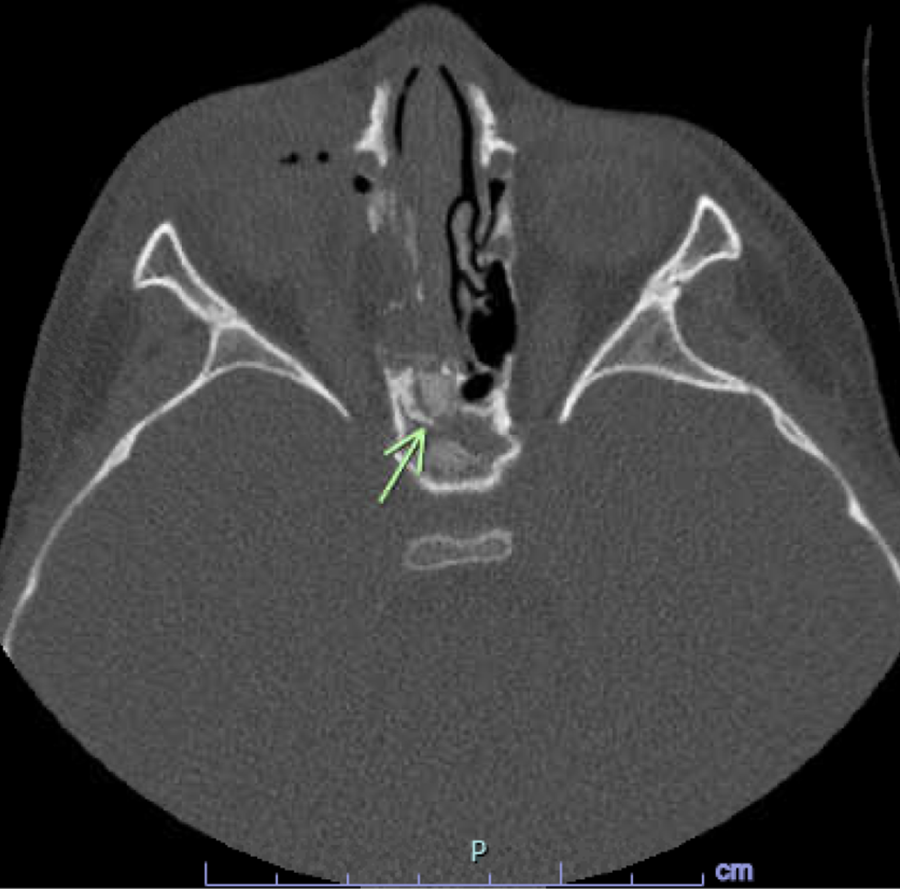
Postoperative computed tomography (CT) prior to endoscopic intervention. Foreign body fragment (crayon, green arrow) is seen left behind in the posterior ethmoid, abutting the face of the sphenoid.
The patient did well postoperatively with good extraocular motility and alignment but was found to have strabismus and mild enophthalmos. One month postoperatively, the patient had no further drainage and full orbital movement and no vision impairment.
Discussion
Pediatric maxillofacial trauma has been shown to exhibit a bimodal peak in early childhood (age 2-5 years) with a second peak in adolescence. Large case series have identified motor vehicle crashes as the most common cause of maxillofacial trauma, followed by falls as was seen in this patient. 5 Transorbital trauma with a penetrating mechanism requires prompt treatment to prevent serious ophthalmologic and intracranial complications. Careful assessment for a retained foreign body is required as its location can influence surgical planning and may require a multidisciplinary approach for complete removal and to minimize iatrogenic injury. Postoperative care should include imaging in select cases to ensure complete removal of the foreign body. Perioperative antibiotics are needed as well due to the introduction of bacteria into the sinuses and intracranial cavity by the foreign body. 2,4
Penetrating orbital injuries have the potential to cause severe brain injury if the cranium is entered, typically via the orbital roof, superior orbital fissure, optic canal, or ethmoid roof similar to the case seen here. 6 Major neurological deficit in these cases may be delayed in presentation, and if a foreign body is retained in the orbit or cranium, severe infectious complications can be seen. 2 More immediate complications include intracerebral hematoma, cerebral contusion, intraventricular hemorrhage, pneumocephalus, brain stem injury, and cerebrovascular injuries. 2
Conclusions
Penetrating transorbital trauma requires expedited treatment to prevent serious ophthalmologic and intracranial complications. Often, a multidisciplinary approach is necessary to ensure complete removal of foreign bodies and minimize iatrogenic injury. Preoperative imaging is essential to identify involved structures and ensure surgical resection is complete. In select cases, postoperative imaging may be necessary to ensure all foreign bodies have been removed and prevent infectious complications.
Footnotes
Authors’ Note
This manuscript is original and has not been submitted elsewhere in part or in whole.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.