
Abstract
Background:
Mouth breathing (MB) is a pediatric public health concern potentially increasing dental caries risk. We investigated risk factors, relationships between clinical characteristics and medical costs, and their effects on caries severity.
Study design:
Observation study.
Setting:
Analysis of clinical characteristics, medical costs, and dental caries in MB children.
Participants:
Eighty-six children with MB secondary to adenoid hypertrophy (AH) and/or tonsillar hypertrophy, recruited from an ENT department (June-August 2023).
Measurements:
MB diagnosis via validated criteria; dental caries assessment; questionnaire on demographics, medical history, body mass index, Paediatric Yorkhill Malnutrition Score, perinatal factors, feeding practices, oral hygiene, parental education, and costs.
Results:
Caries prevalence was 40.7% (35/86). Caries correlated significantly with longer MB duration (P = .013), higher total IgE (P = .004), and delayed toothbrushing initiation (P = .001). AH severity (assessed by Pharyngeal Airway Space, P = .013; choanal obstruction grade, P = .006) correlated with caries. Non-caries children showed higher breastfeeding rates (P = .026). Multivariate analysis identified formula feeding (odds ratio (OR) = 10.099, P = .026), longer disease duration (OR = 1.495, P = .035), and delayed oral hygiene initiation (OR = 2.171, P = .025) as independent caries predictors. Medical costs positively correlated with maternal education (r = 0.280, P = .009), AH grade (r = 0.345, P = .001), disease duration (r = 0.383, P < .001), and prematurity (r = 0.457, P < .0001), with maternal education exerting the strongest cost influence. Delayed toothbrushing (r = 0.213) and formula feeding (r = 0.219) positively correlated with higher decayed, missing, filled teeth/decayed, missing, or filled surfaces (affected surfaces) indices.
Conclusion:
MB-associated caries is highly prevalent and costly. Multiple modifiable risk factors contribute to its occurrence in children.
Background
Mouth breathing (MB), defined as chronic airflow through the oral cavity due to nasal obstruction (such as chronic sinus issues, allergic rhinitis [AR], adenoid hypertrophy [AH], and/or tonsillar hypertrophy [TH]) 1 or habitual factors, disrupts normal nasal respiration. This compels children to breathe through their mouth for relief. These physical blockages often require medical intervention. Habitual factors like prolonged pacifier use or thumb sucking may also encourage MB by altering oral and facial muscles. This condition reduces salivary flow, 1 leading to xerostomia, pH imbalance, and increased bacterial colonization. 2
Epidemiological studies report an MB prevalence ranging from 4.7% to 34.5%,3 -5 establishing it as a growing public health concern with increasing recognition in both clinical and societal contexts. Concurrently, childhood dental caries represents a significant global burden. Untreated decay in primary teeth exceeds the prevalence of all other chronic pediatric health conditions. 6 The 2022 Global Oral Health Report estimates that 514 million children worldwide are affected by deciduous dental caries, 7 resulting in substantial annual health care expenditures. 7 While MB is hypothesized to compromise salivary flow—thereby diminishing oral clearance mechanisms and increasing caries risk 1 —robust evidence delineating specific MB-associated risk factors for caries remains limited.
Notably, a subset of pediatric patients continues to experience MB even after adenotonsillectomy,8,9 often due to persistent habitual patterns. This entrenched behavioral MB necessitates long-term oral rehabilitation and specialized dental care, contributing significantly to societal health care burdens. Consequently, identifying modifiable risk factors for caries in children with MB is critical for developing cost-effective preventive strategies and reducing future health care expenditures.
This study aimed to identify specific risk factors linking MB to dental caries, using dmft (decayed, missing, or filled teeth) and dmfs (decayed, missing, or filled surfaces) indices, in children and quantify related medical costs. We hypothesized that MB increases caries severity through specific habitual factors.
Materials and Methods
Study Subjects
This study received ethical clearance from the Institutional Review Board of the Third Affiliated Hospital of Sun Yat-sen University (approval no [2022]02-141-01) and adhered strictly to the ethical principles outlined in the Declaration of Helsinki. Written informed consent was obtained from the legal guardians of all participating children prior to enrollment. This cross-sectional study was approved by the Institutional Review Board of the Third Affiliated Hospital of Sun Yat-sen University. A cohort of 86 pediatric patients (aged 2-10 years) diagnosed with chronic MB secondary to AH and/or TH, who were scheduled for adenoidectomy and/or tonsillectomy between July 1 and August 1, 2023, was prospectively enrolled from the ENT Department (Table 1). All participants underwent standardized preoperative pediatric dental evaluations to assess dental caries status.
Questionnaire of MB Criteria.
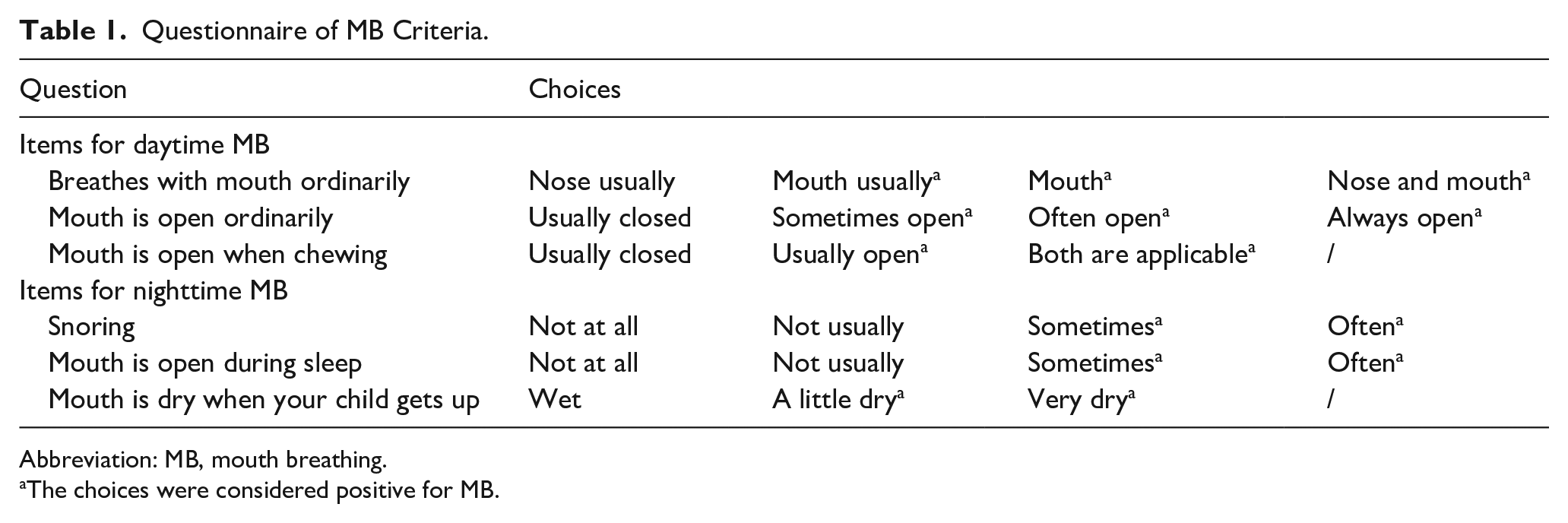
Abbreviation: MB, mouth breathing.
The choices were considered positive for MB.
Inclusion criteria comprised: (1) Age 2 to 10 years; (2) confirmed MB diagnosis through validated questionnaire screening 10 ; (3) absence of genetic predisposition to malocclusion, orofacial myofunctional disorders (eg, tongue thrusting), or parafunctional oral habits (eg, thumb sucking).
Exclusion criteria included: (1) Prior adenoidectomy/tonsillectomy; (2) history of orthodontic intervention or maxillofacial surgery; (3) comorbid conditions or behavioral patterns potentially contributing to MB (eg, neurological disorders, chronic AR, or habitual pacifier use).
Questionnaire
The questionnaire encompassed comprehensive demographic characteristics (age, sex), clinical parameters including medical history of MB, body mass index 11 (BMI), and nutritional status assessed through the Paediatric Yorkhill Malnutrition Score. It further documented perinatal factors (delivery mode), early-life nutritional patterns (infant feeding modalities), and developmental behaviors (dietary preferences, oral hygiene practices such as toothbrushing initiation age and frequency). Additional variables included comorbid chronic conditions, parental educational attainment, allergic profiles, and anatomical evaluations of AH severity via nasal endoscopic examination and lateral nasopharyngeal radiography. Supplementary behavioral assessments captured orofacial parafunctional habits (tongue thrusting, digit sucking, object biting) alongside epidemiological data on dental caries prevalence. Health care utilization metrics incorporated treatment costs from both otolaryngology and dental departments. All data collection protocols excluded participants with primary MB presentations to focus on secondary behavioral and pathological contributors.
MB Criteria
These children with MB were diagnosed using a validated questionnaire 10 (see Table 1). MB diagnosis followed established criteria 10 : Daytime MB required ≥2 positive responses indicating open-mouth posture, dry lips, or snoring; nighttime MB required ≥2 symptoms such as snoring or dry mouth upon waking (full questionnaire in Table 1). We administered this survey to assess both daytime and nighttime symptoms indicative of MB.
Assessment of Dental Caries
Prior to adenotonsillectomy procedures in the otolaryngology department, all MB children underwent standardized dental evaluations. Following oral rinsing and dental cleaning to remove excess saliva, comprehensive intraoral photographic documentation was performed, capturing occlusal, buccal, lingual, and palatal aspects of all teeth. Caries assessment adhered to World Health Organization guidelines, 12 utilizing the dmf index for primary dentition. 13 A single calibrated dentist evaluated preoperative caries status through 2 metrics: dmft and dmfs (affected surfaces), with criteria defined as follows: decayed (d) denoted lesions extending into dentin, missing (m) indicated teeth extracted solely for caries-related reasons, and filled (f) represented restorations completed for caries management, considering restoration dimensions, morphology, and overall dental health. 14 Enamel-limited lesions were excluded from scoring. Both dmft and dmfs indices were systematically recorded for subsequent statistical analysis (Figure 1).

Classic intraoral images from the mouth-breathing children. The image shows the common clinical manifestations: proclined incisors, high-arched palate, narrow dental arch, dental crowding, and dental caries. The blue arrow marks the location of tooth decay, and the red arrow indicates the filling material after the decayed teeth have been restored. (A) Right Buccal Occlusal View showed the spee cure was deep. (B) Left Buccal Occlusal View showed the upper incisors flared more than normal. (C, D) Maxillary and Mandibular Occlusal View. (E) Mesial View showed the full dentition condition. The red arrow indicated the filled teeth. The blue arrow marks the specific position of caries.
Statistical Analysis
All analyses were conducted using SPSS Statistics 27.0 (IBM Corp, Armonk, NY, USA). Normality of data distribution was assessed via the Kolmogorov-Smirnov test. Continuous variables with normal distribution were expressed as mean ± standard deviation and analyzed using independent t-tests (2-group comparisons) or 1-way ANOVA (multigroup comparisons). Non-normally-distributed data were reported as median (interquartile range) and evaluated with the Mann-Whitney U test (2-tailed) for between-group differences. Categorical variables were compared using chi-squared (χ2) tests. Multivariate logistic regression models identified independent predictors of dental caries, while linear regression analysis examined factors influencing medical costs in MB children, adjusted for potential confounders. Correlation analyses differentiated between Spearman’s rank correlation (nonparametric data) and Pearson’s correlation (normally-distributed data) to assess variable associations. A 2-sided significance threshold of P ≤ .05 was applied throughout the study.
Results
Demographics and Clinical Profile of MB Children
The study cohort comprised 86 children diagnosed with MB, aged 2 to 11 years (mean age: 8.12 ± 3.01 years; mean MB duration: 2.49 ± 1.84 years), with a male predominance (59 males vs 27 females, Table 2). Dental caries was identified in 35 children (40.7%, Figure 1), while 51 remained caries-free. Children with caries exhibited significantly-longer MB history (3.00 [1.00-5.00]) than those without caries (P = .013). A total of 65 cases were delivered naturally, and 2 cases were premature. Anthropometric analysis revealed a mean BMI of 16.76 ± 3.28, with underweight prevalence (≤18 kg/m², n = 61) substantially exceeding overweight/obese cases (>24 kg/m2, n = 3). 11 Oral hygiene practices demonstrated marked differences: caries-free children initiated toothbrushing earlier (2.89 ± 1.00 years) than caries-affected peers (3.69 ± 1.13 years, P = .001). Immunological profiling via ImmunoCAP revealed elevated total IgE levels in caries-positive subjects (267.94 ± 404.64 IU/mL) versus caries-negative counterparts (87.63 ± 124.07 IU/mL, P = .004), with 36 children exhibiting allergen sensitivity.
Demographic Data and Baseline Characteristics of Participants.
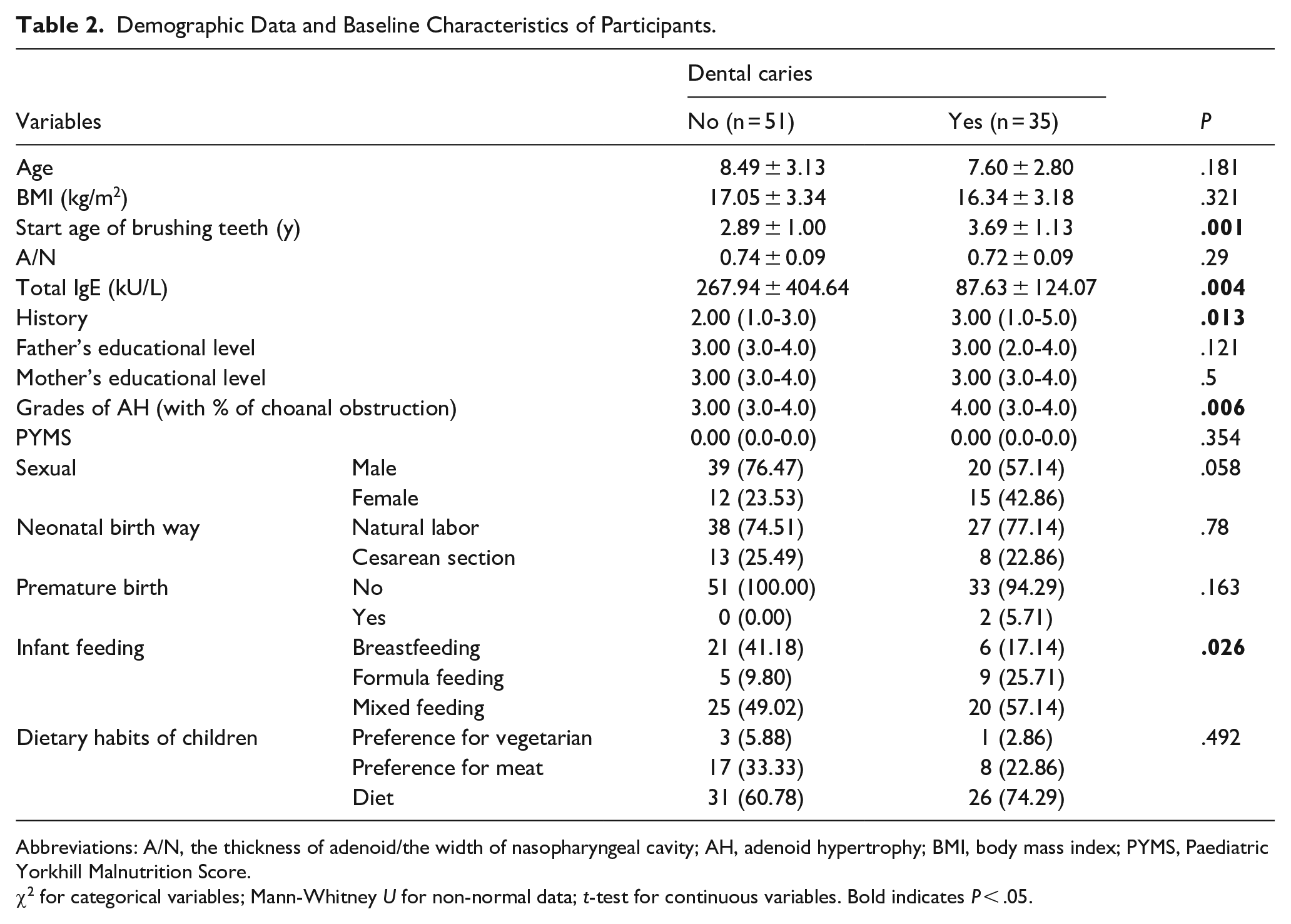
Abbreviations: A/N, the thickness of adenoid/the width of nasopharyngeal cavity; AH, adenoid hypertrophy; BMI, body mass index; PYMS, Paediatric Yorkhill Malnutrition Score.
χ2 for categorical variables; Mann-Whitney U for non-normal data; t-test for continuous variables. Bold indicates P < .05.
Infant feeding patterns showed 27 exclusively breastfed and 14 formula-fed cases, while childhood dietary preferences skewed toward carnivorous diets (n = 25) over vegetarian (n = 4). AH severity, graded via choanal obstruction percentages, 15 predominated at Grade IV (75%-100% obstruction, n = 43, 50%), particularly among caries-positive children (71.43% Grade IV vs 29.42% in caries-negative group, P = .006). Pharyngeal Airway Space (PAS) measurements corroborated these findings, demonstrating greater obstruction severity in caries-affected children (7.00 [5.4-9.4], P = .013). Notably, non-caries children exhibited distinct feeding modality distributions, with breastfeeding prevalence (n = 21) significantly outweighing formula feeding (n = 1) and mixed feeding (n = 25, P = .026). These results collectively highlight associations between caries status, developmental oral hygiene practices, immunological profiles, and anatomical obstruction severity in pediatric MB patients.
Analysis of Clinical Characteristics Influencing MB
A multivariable logistic regression model was constructed incorporating MB duration, PAS, oral hygiene initiation age, total IgE levels, AH severity, and infant feeding modalities, which identified critical predictors of dental caries risk in pediatric MB patients. The model demonstrated that delayed commencement of toothbrushing (odds ratio [OR] = 2.171, P = .025), prolonged MB history (OR = 1.495, P = .035), and formula-based infant nutrition (OR = 10.099 vs breastfeeding) significantly elevated caries susceptibility, while mixed feeding conferred a 4.538-fold increased risk (Table 3). Paradoxically, elevated total IgE levels exhibited a modest protective effect (OR = 0.994 per IU/mL increase; 95%CI 0.990-0.998), though this association requires cautious interpretation given the complex immunopathological interplay. Notably, earlier initiation of regular toothbrushing practices emerged as a strong protective factor, with each year delay in hygiene initiation progressively amplifying caries risk.
Multivariable Analysis for Dental Caries of Mouth Breathing Children.
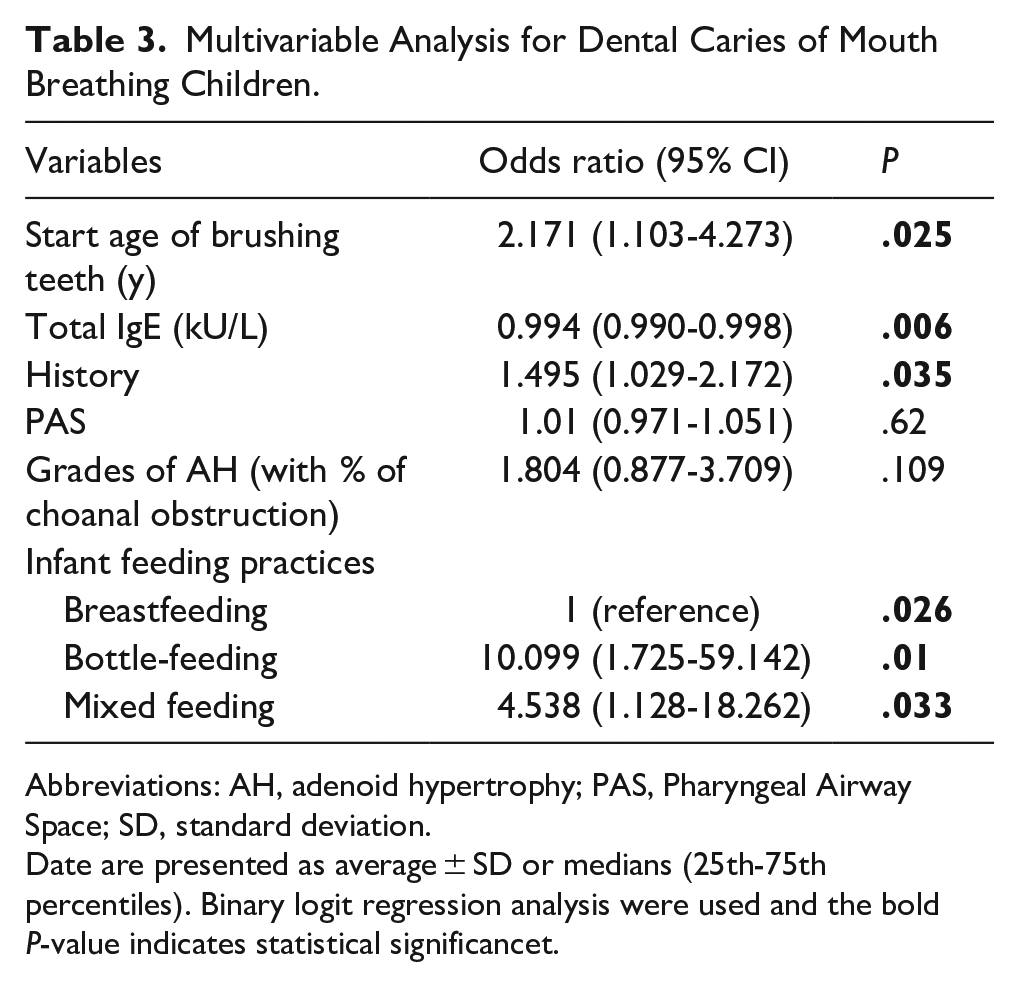
Abbreviations: AH, adenoid hypertrophy; PAS, Pharyngeal Airway Space; SD, standard deviation.
Date are presented as average ± SD or medians (25th-75th percentiles). Binary logit regression analysis were used and the bold P-value indicates statistical significancet.
Higher Maternal Education Level Increases Medical Costs for MB Children
Pearson correlation analysis revealed significant positive associations between medical costs and maternal education level, AH obstruction grades, duration of medical history, and prematurity status in MB children (Table 4). Multivariate linear regression analysis, adjusting for potential confounders, identified these 4 factors—prolonged medical history (r = 0.383, P = .000), elevated maternal education (r = 0.280, P = .009), severe AH obstruction (r = 0.345, P = .001), and prematurity (r = 0.457, P < .0001)—as independent predictors of increased health care expenditures. Notably, maternal education demonstrated the strongest influence on cost escalation among all determinants (Table 5).
Pearson Correlation Analysis Between Clinical Characteristics and Medical Cost in Children With Mouth Breathing.
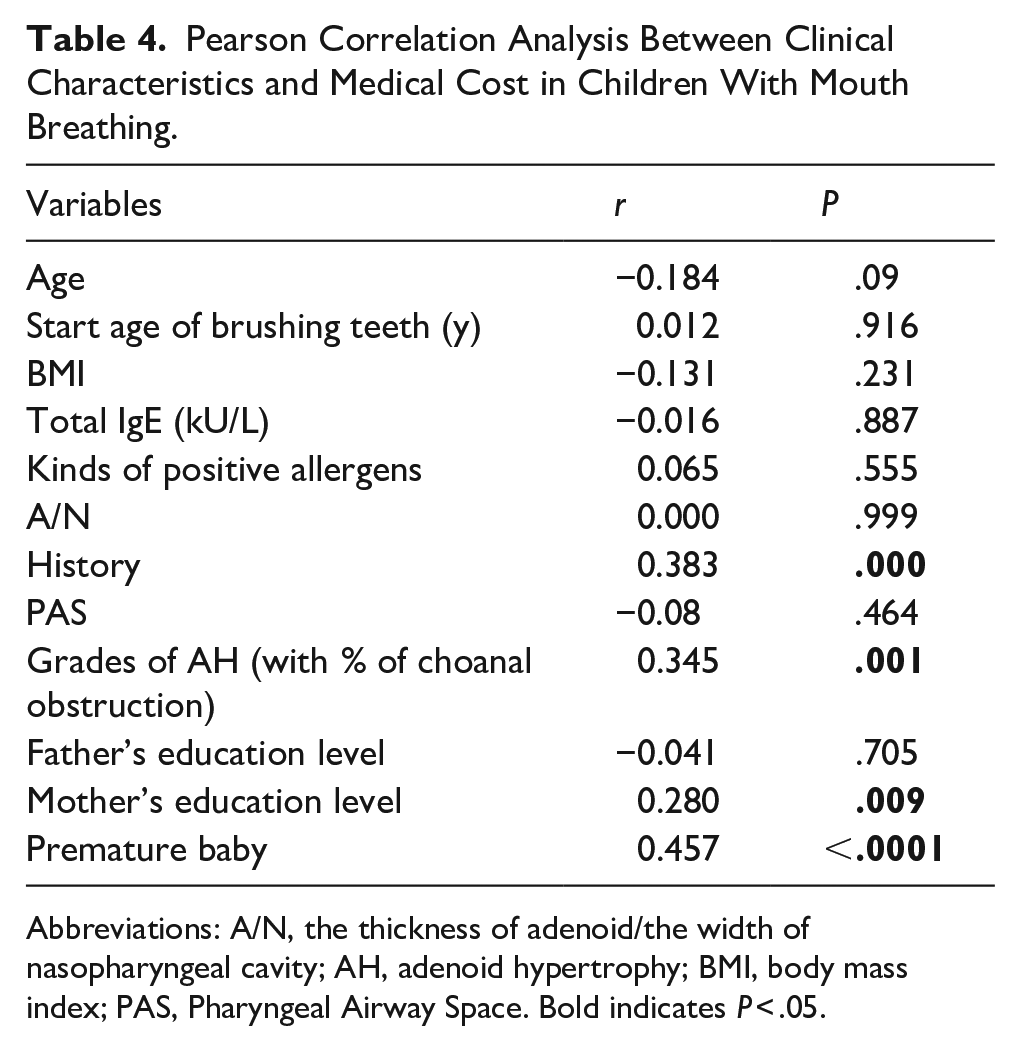
Abbreviations: A/N, the thickness of adenoid/the width of nasopharyngeal cavity; AH, adenoid hypertrophy; BMI, body mass index; PAS, Pharyngeal Airway Space. Bold indicates P < .05.
Multivariate Linear Regression Analysis for Medical Cost of Mouth Breathing Children.
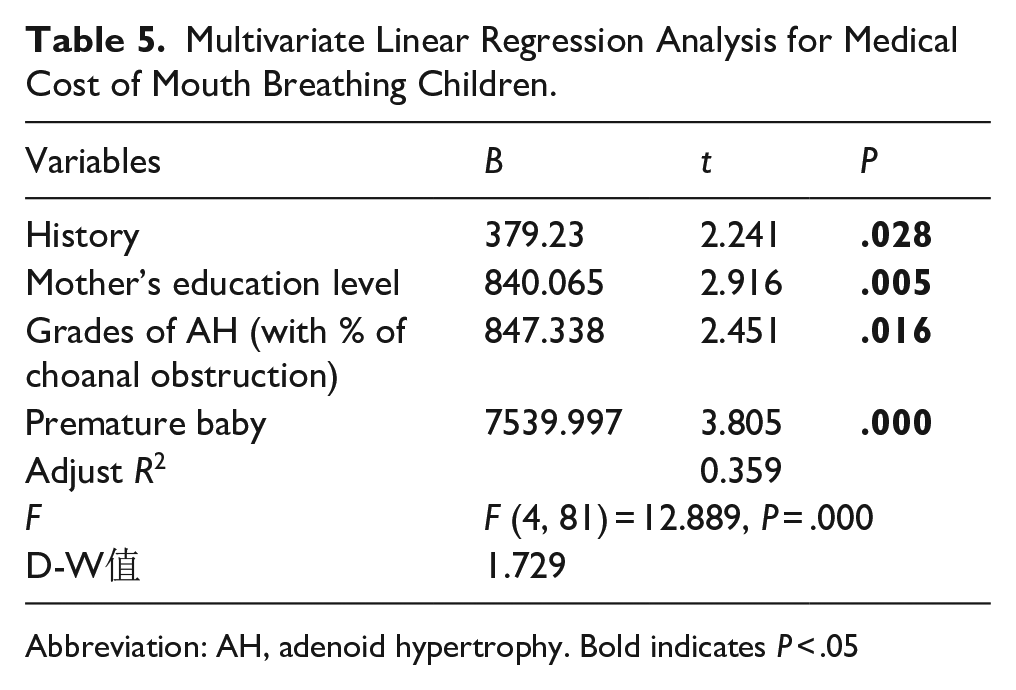
Abbreviation: AH, adenoid hypertrophy. Bold indicates P < .05
Risk Factors for Dental Caries Severity and Correlation Analysis in MB Children
Building on prior research that examined associations between clinical characteristics and dental caries prevalence, this study further assessed caries severity using dmft and dmfs indices. Expanding previous findings, we analyzed correlations between these indices and 4 significant variables identified earlier: toothbrushing initiation age, tIgE levels, medical history duration, and infant feeding practices (Table 6). A statistically-significant positive association between later initiation of toothbrushing and elevated dmfs scores (r = 0.213, P = .049) was found. Notably, there was a positive correlation between infant feeding practices and dmft values (r = 0.219, P = .042). There were no significant associations between caries severity indices and tIgE levels or medical history. These findings highlight the differential impacts of developmental oral hygiene practices and early-nutritional patterns on caries progression metrics.
Spearman Correlation Analysis Between Severity of Dental Caries and Clinical Characteristics.
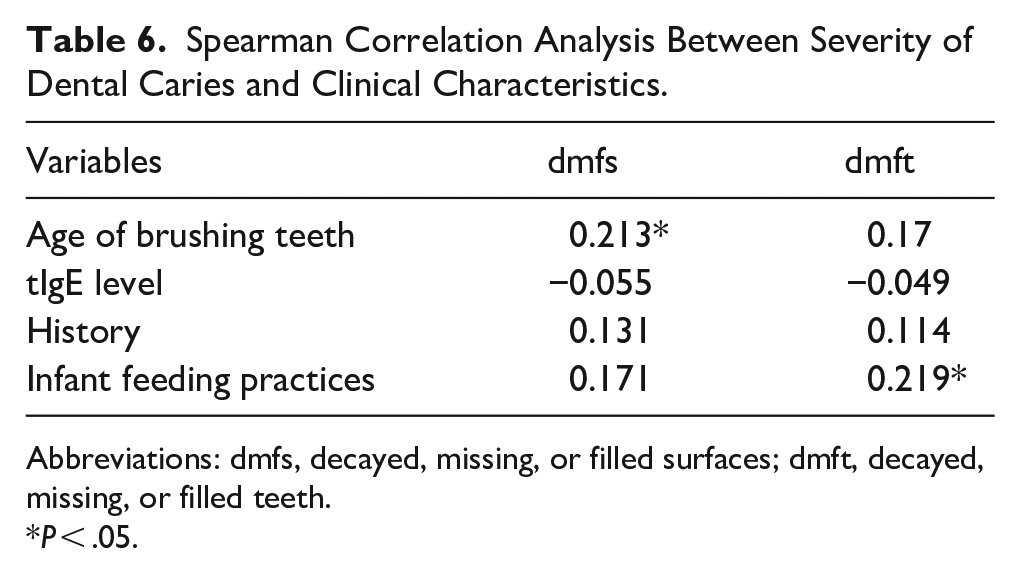
Abbreviations: dmfs, decayed, missing, or filled surfaces; dmft, decayed, missing, or filled teeth.
P < .05.
Discussion
A child’s developing jaw and oral anatomy may inadvertently promote MB. Chronic MB can alter facial development,16,17 particularly during childhood—a critical period of rapid maxillofacial growth. 18 While most parents express concern about their children’s maxillofacial deformities, they often overlook the dental caries risk associated with long-term MB.
MB reduces salivary flow, creating a xerostomic environment that disrupts oral homeostasis. Saliva performs critical functions including acid neutralization, digestive initiation, and early-caries remineralization. 19 Diminished salivary buffering capacity enables cariogenic pathogens like Streptococcus mutans to demineralize enamel through acidic metabolites. Concurrently, MB-induced xerostomia impairs saliva’s protective clearance of food debris and bacteria, exacerbating plaque accumulation while reducing acid-neutralizing and remineralization capacities—thereby accelerating cariogenic processes.20,21 Chronic MB correlates with sustained reductions in salivary flow and pH, increasing enamel demineralization and caries risk. 22 In contrast, intermittent MB (eg, during exercise) typically causes only transient dry mouth and poses minimal long-term mineralization risks unless combined with other factors like high-sugar diets. Caries in primary teeth can impair children’s mastication, growth, and development. Severe cases may lead to speech difficulties, jaw development issues, and nutritional deficiencies—while also elevating future risk for permanent tooth caries. 2
Early-childhood caries arises from frequent sugar consumption within an environment of enamel-adherent, acid-producing bacteria in complex biofilms, alongside enamel developmental defects. 23 Our analysis revealed a 41% caries prevalence among MB-affected children, exceeding rates in general populations: 25.9% in Japanese 3 year-olds and 27.9% in American children aged 2 to 5 years. These findings highlight the need for greater clinical attention to oral respiration patterns in caries prevention strategies. 24 Given this study’s limited sample size, the observed prevalence was lower than China’s Fourth National Oral Health Epidemiological Survey, 25 which reported caries rates of 50.8% (3 year-olds), 63.6% (4 year-olds), and 71.9% (5 year-olds).
Globally, dental caries in the primary dentition imposes substantial indirect economic burdens, with recent estimates ~US$1.55 billion annually. 7 The global burden of early-childhood caries, particularly severe in China, necessitates urgent prioritization of preventive strategies for high-risk populations such as MB children. Our analysis identified the longer the medical history, the higher the probability of dental caries, of which increases by 1.295 times; the older a child start brushing teeth, the higher the probability of dental caries, of which the risk will increase by 2.171 times. These findings align with meta-analytic evidence demonstrating reduced caries prevalence in breastfed children, 26 though prolonged breastfeeding (>12 months) may paradoxically elevate risk. 27 Collectively, these insights advocate for age-specific oral hygiene guidelines and targeted public health interventions in high-prevalence regions. It is worth noting that breastfeeding duration exhibits heterogeneous effects on caries risk. To mitigate confounding variables (eg, postweaning dietary patterns), this study analyzed breastfeeding limited to ≤6 months. 28 Our analysis demonstrated a protective effect of infant breastfeeding against caries incidence, supporting its integration into early-preventive oral care strategies.
Second, early-toothbrushing initiation age significantly influenced outcomes (Table 4). Our study found children began regular brushing at ~3 years on average. By contrast, current guidelines recommend introducing fluoride toothpaste upon the eruption of the first primary teeth (around 6 months of age, coinciding with complementary food/drink introduction). 28 The study cohort comprised children aged 2 to 11 years who demonstrated the capability to independently maintain regular toothbrushing routines. To isolate the variable of parental supervision, this investigation prioritized evaluating the timing of oral hygiene initiation over fluoride exposure analysis. Our findings emphasize that early establishment of toothbrushing habits, mediated by caregiver oversight, significantly influences caries prevention outcomes. Furthermore, parental supervision efficacy exhibited a statistically-significant correlation with educational attainment levels. This association underscores how disparities in caregiver education may disproportionately elevate caries-related health care expenditures, particularly in populations with limited access to preventive dental resources, which was the same as some research.29,30 Educated mothers may seek specialized care such as frequent dental visits, advanced treatments, increasing costs despite lower caries prevalence due to preventive practices. What’s more, education correlates with awareness of oral health risks, prompting early interventions (eg, orthodontic evaluations) that incur expenses but mitigate severe outcomes.
Surprisingly, allergies may confer a protective effect against dental caries. Parents of allergic children often restrict their intake of cariogenic snacks, candy, and soda—thereby reducing caries risk. However, contrasting evidence indicates AR patients experience 13% to 25% more caries-related clinical visits, with AR medications also contributing to caries formation. 31 Asthma doubles caries risk in both primary and permanent dentition, 32 through multiple mechanisms: xerostomia (extreme dry mouth), chronic use of carbohydrate-rich nebulizers, frequent medication intake, 33 and asthma medications that reduce salivary flow and secretory immunoglobulin A levels. 34 The precise pathophysiological mechanisms remain incompletely understood.
Apart from that, the relationship between allergic sensitization and caries remains underexplored; thus, we advocate for prospective cohort studies to elucidate potential immunological mechanisms. Our study identified modifiable risk factors for caries in MB children (eg, delayed toothbrushing initiation). Subsequent economic burden analysis revealed that prolonged clinical history, elevated maternal education, greater AH severity, and preterm birth significantly predicted elevated health care expenditures (Table 4). Addressing these factors may mitigate caries-related economic burdens in this population. Additionally, a multiple regression analysis (Table 5) revealed that 4 risk factors collectively explained 38.9% of medical expense variance in MB children, with no significant multicollinearity. Preterm birth exerted the strongest influence on costs, followed by adenoid obstruction. Notably, higher maternal education correlated with increased expenditures (Table 4), though no association with caries prevalence was observed (Table 2).
Our analysis revealed a positive correlation between delayed toothbrushing initiation and caries severity, highlighting early oral hygiene practices as critical for prevention. Conversely, breastfeeding ≥1 year conferred protection, whereas formula feeding increased caries risk. Mechanistically, breastfeeding directs milk posteriorly, minimizing tooth exposure, while bottle-feeding pools milk anteriorly, prolonging enamel contact. Although breast milk alone is minimally cariogenic, its combination with sucrose (eg, in complementary foods) accelerates caries progression. Experimental models demonstrate that human milk supplemented with 10% sucrose induces dentinal caries within 3.2 weeks, underscoring the synergistic role of dietary sugars. 35 Our analysis revealed a positive correlation between delayed toothbrushing initiation and caries severity, highlighting early oral hygiene practices as critical for prevention. Conversely, breastfeeding ≥1 year conferred protection, whereas formula feeding increased caries risk. Mechanistically, breastfeeding directs milk posteriorly, minimizing tooth exposure, while bottle-feeding pools milk anteriorly, prolonging enamel contact.
Although prolonged breastfeeding (>6 months) has been associated with elevated caries risk, breast milk inherently contains anticariogenic components (eg, immunoglobulins, lactoferrin) that inhibit S. mutans colonization 36 and enhance enamel remineralization via calcium/phosphorus deposition. 35 By contrast, formula feeding introduces cariogenic risks due to sucrose content and lower pH, 37 promoting enamel demineralization. Recent studies, however, suggest that breast milk may paradoxically lower plaque pH more than bovine milk under specific conditions (eg, when combined with dietary sugars), accelerating enamel dissolution. 38 This underscores the need to contextualize breastfeeding’s cariogenic potential within broader dietary and behavioral practices.
However, this study did not assess pH differences between breast milk and formula. Including bovine milk as a variable in infant feeding practices might produce different outcomes, highlighting the need for future research to evaluate how milk composition (eg, pH profiles, carbohydrate content) influences childhood caries risk. Although no association emerged between dietary patterns and caries incidence/severity in MB children here, established evidence confirms healthy diets prevent caries. This discrepancy might reflect unmeasured variables (eg, frequency of sugary beverage consumption, as noted in limitations). Key modifiable risk factors identified including delayed toothbrushing initiation, higher maternal education, non-breastfeeding practices, and AH severity. Targeted interventions addressing these factors could significantly reduce caries-related economic burdens in MB populations.
Conclusions
MB-associated early-childhood caries represents a globally-prevalent public health concern with substantial societal costs. Multiple risk factors contribute to caries development in MB-affected children. Evidence-based preventive strategies emerging from our research include the following: (a) Prioritizing breastfeeding over formula feeding for infants under 12 months 14 ; (b) initiating twice-daily toothbrushing with fluoridated toothpaste under parental supervision upon the eruption of the first deciduous tooth 6 (≈6 months of age); and (c) early referral to pediatric dentists for high-risk children (eg, prolonged MB, formula-fed infants) to implement targeted preventive regimens (eg, fluoride varnish 39 ).
Strengths and Limitations
This represents the first study investigating dental caries prevalence and medical costs in MB children. However, as a single-center investigation with limited sample size, future multicenter studies utilizing larger cohorts are warranted. Moreover, the cross-sectional design precludes causal inference; longitudinal analyses are required to assess long-term impacts of MB. Third, unmeasured variables including fluoride exposure (eg, toothpaste concentration, community water fluoridation), detailed dietary habits (eg, frequency of sugary beverage/snack consumption), and toothpaste dosage may introduce residual confounding. Finally, while we observed that higher maternal education correlated with increased medical expenditures, possibly reflecting greater health care-seeking behavior or access to specialized services, we did not collect granular socioeconomic data (eg, household income, insurance coverage, or geographic accessibility to care). These unmeasured factors may confound the association between education and costs. Future studies should incorporate standardized socioeconomic metrics to better isolate the drivers of health care utilization in this population.
Footnotes
Acknowledgements
The authors would like to thank all parents and children who have contributed to the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (82000957 and 82071079) and General Program of Natural Science Foundation of Guangdong Province (2021A1515011764).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All the data have been included in the main text.