
Abstract
Pott’s puffy tumor (PPT) is a nonneoplastic complication of acute frontal sinusitis characterized by subperiosteal abscess (SPOA) formation and osteomyelitis. Although various clinical conditions are associated with frontal SPOA, cases associated with odontogenic sinusitis are rare. We report a recurrent case of frontal SPOA who had a previous history of craniotomy due to head trauma. The patient was presented with headache, facial swelling and diagnosed as frontal, ethmoid, and maxillary sinusitis with frontal SPOA, which is PPT. The patient was surgically managed by endoscopic sinus surgery and external drainage of the abscess. Although the symptoms had been relieved soon after the surgery, they were recurred after 1 week. By paranasal sinus computed tomography scans, it was suspected that severe carious teeth, which were missed before surgery, induced maxillary sinusitis which spread into the frontal sinus and subperiosteal areas inducing recurrence of disease. Our experience suggests that frontal SPOA may originate from odontogenic maxillary sinusitis caused by severe dental caries, which should be actively managed, especially in patients with the risk of spread of inflammation, such as those who have discontinuity in frontal bone.
Introduction
Pott’s puffy tumor is a nonneoplastic complication of acute frontal sinusitis characterized by subperiosteal abscess (SPOA) formation and osteomyelitis. 1 It was first described by Sir Percival Pott in 1760, and its symptoms include headache, mild to no fever, facial pressure, pain, and purulent nasal discharge. The fontal SPOA usually develops after sinusitis or in some cases, trauma, which is less likely.1,2 Odontogenic sinusitis results from dental pathologies and usually involves the maxillary sinus. Recently, we experienced a case of frontal SPOA complicated by severe carious teeth-related maxillary sinusitis in a patient with a history of craniotomy due to head trauma. Odontogenic sinusitis-associated frontal SPOA are rare and only 3 cases have been reported previously.2,3,4 Here, we present our case, and try to review the previously reported cases of frontal SPOA caused by odontogenic maxillary sinusitis.
Case Report
A 37-year-old woman presented to the department of Neurosurgery with a large midline swelling of the forehead and bilateral eyelid swelling (Figure 1A). The lump on her forehead had appeared suddenly 2 weeks prior. She had no specific medical history except a craniotomy due to head trauma 13 years ago. A brain computed tomography (CT) revealed a 6.5-cm low-density lesion with irregularly peripheral enhancement in the forehead region and diffuse periorbital inflammation in both eyes. Multiple defects in the anterior wall of the frontal sinus, which caused by the previous craniotomy, and left frontal, ethmoid, and maxillary sinusitis were noted. However, there was no evidence of intracranial extension (Figure 1B). She was referred to our department for proper management. Paranasal sinus CT images performed for surgical plan, showed frontal, ethmoid, and maxillary sinusitis and frontal SPOA (Figure 1C). An emergency endoscopic sinus surgery (ESS; including frontal [Draf IIA], ethmoid, and maxillary sinuses) was performed with drainage of the frontal abscess via an external midline incision. Subsequently, 150 mL of pus was drained. A bacterial culture test was performed, but no bacterial growth was observed. Histopathological results of the surgically removed tissue from the lump revealed severe inflammation and tissue necrosis. After the surgery, her symptoms rapidly improved. However, at 1 week after the surgery, the foreheads welling recurred and pus discharge was observed on the incision site of the forehead. Paranasal sinus CT was retaken, and swelling and fluid collection in frontal subperiosteal area (Figure 2A) with mild sinusitis of frontal, ethmoid, and maxillary sinuses were identified (Figure 2B). By reviewing the CT images, we hypothesized that recurred inflammation in frontal subperiosteal area might be spread from maxillary sinus which was suspected to be associated with dental problem (Figure 2B, marked). And we found that dental problem, which had been missed at preoperatively, was also noted in preoperative paranasal sinus CT images (Figure 1C, marked). We carefully examined the oral cavity and found severe dental caries in left upper teeth with suspected oroantral fistula (Figure 2C). She was referred to the dental clinic and severe carious teeth were removed. Revision ESS was performed to remove the inflamed tissues in the maxillary, ethmoid, and frontal sinuses. During the operation, we found that frontal outflow tract was still patent but narrowed and revision frontal procedure of a Draf IIB with maxillary sinus surgery was performed. After the operation, intravenous antibiotics was continued for 3 weeks. The patient was free of disease at the 6-month follow-up.
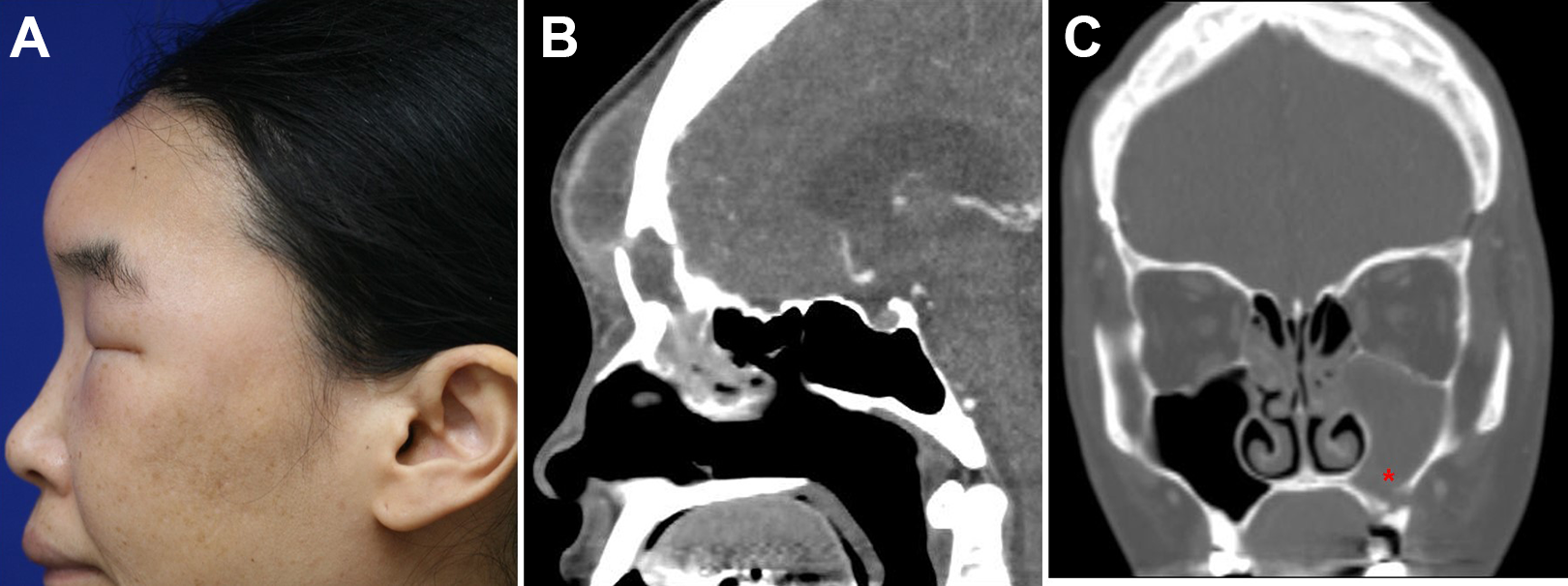
(A) Lateral view of the patient showing swelling of the forehead and periorbital area. (B) Sagittal view of the patient’s brain on a computed tomography (CT) scans showing a low-density lesion with peripheral irregular enhancement in the forehead and diffuse inflammation in both periorbital areas. (C) Coronal view of the patient’s paranasal sinuses.
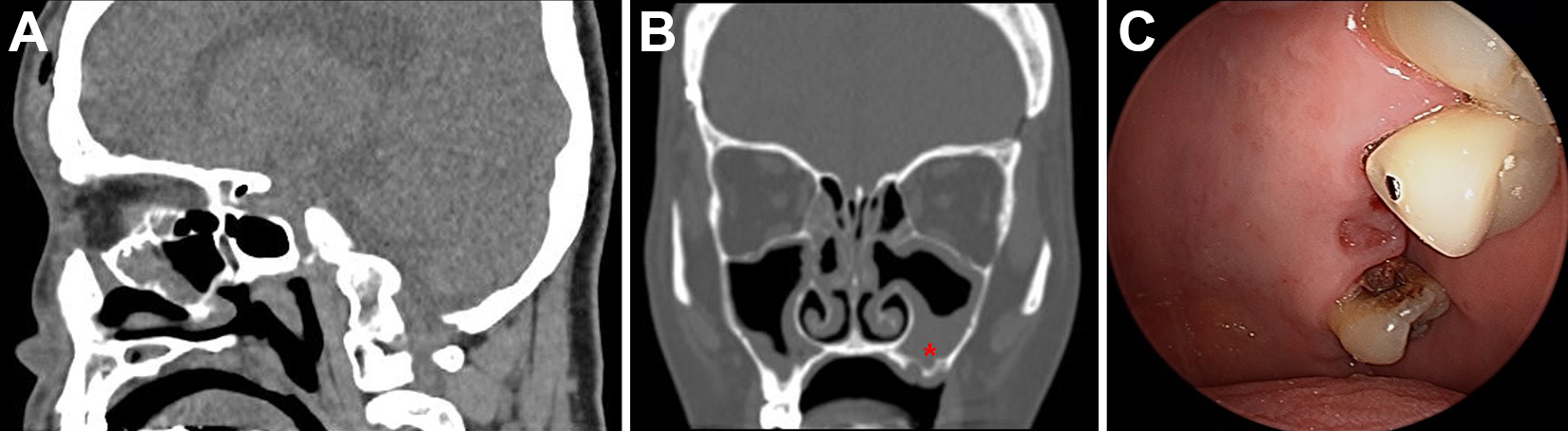
(A) Sagittal view of a computed tomography (CT) scans of the paranasal sinuses, taken 1 week after the first endoscopic sinus surgery (ESS). Swelling and fluid collection in frontal subperiosteal area is observed suggesting recurrence of diseases. (B) Recurrence of maxillary sinusitis with a bony defect in the maxillary sinus floor, suggesting a dental problem is demonstrated. (C) Severe dental caries and oroantral fistula were identified in the maxillary teeth.
Discussion
Although the incidence of frontal SPOA has been decreasing, the condition remains life-threatening. Frontal SPOA may originate from untreated frontal sinusitis as well as insect bites, acupuncture, and mastoid surgery in rare cases. 5 To our knowledge, there have been 3 other previous reports of odontogenic sinusitis-associated frontal SPOA. One case was associated with a retained root which was thought to be the cause of sinusitis and subsequent frontal SPOA. A CT scan demonstrated extensive opacification of the left maxillary, sphenoid, and ethmoidal sinuses. The patient was managed by ESS with external drainage of frontal sinus abscess and removal of retained root of tooth. 3 In other case, the patient had the history of teeth extraction before development of symptoms of frontal SPOA. A CT scan showed the sinus infection in the maxillary and frontal sinuses with intracranial extension. Dental procedure–associated oroantral fistula was also observed. He was managed through bicoronal incision, craniotomy, removal of the anterior table of frontal sinus and other infected tissues, and obliteration of frontal sinus and frontal outflow tract. Cultures from the wounds contained gram-positive and negative species, Prevotella melaninogenica, and Peptostreptococcus species. 2 The third case had a history of a tooth extraction 2 months before, and CT scans revealed mild unilateral maxillary sinusitis, complete opacification of left frontal sinus, and some ethmoid disease. 4 The subperiosteal and epidural abscesses were evacuated through a bicoronal approach. Purulent material was drained through a frontal sinus trephination. Culture was positive for Streptococcus intermedius and Bacteroides melaninogenicus. This is the fourth case report of frontal SPOA associated with odontogenic sinusitis. In present case, severe dental carious teeth-associated maxillary sinusitis may have spread upward through the frontal outflow tract to the frontal sinuses. Furthermore, a bony defect of the anterior frontal bone from a previous head trauma might have aggravated the spread of the infection, leading to recurrence of inflammation of frontal subperiosteal area.
Regarding the result of culture, the most common pathogens associated with frontal SPOA are non-enterococcal Streptococci, Staphylococci, and anaerobes that can colonize the respiratory tract. 6 However, only 50% of cases have positive cultures; in many cases, the culture can be negative, such as that in the case reported here. One of the reasons is that preoperative administration of empirical intravenous antibiotics may affect the culture results as in our case.
We cannot rule out the possibility that frontal sinus surgery was not enough during first surgery and frontal outflow tract was narrowed, or infection from the dental caries was seeded directly into the frontal sinus. However, our case gives a lesson that paranasal sinus CT and oral cavity should be carefully reviewed regarding odontogenic sinusitis, and if there is a possibility that dental problem is associated with sinusitis, it should be actively managed.
Conclusion
This is the fourth reported case of frontal SPOA associated with odontogenic sinusitis. Based on our experience, frontal SPOA may originate from odontogenic maxillary sinusitis caused by severe dental caries, which should be actively managed, especially in patients with the risk of spread of inflammation, such as those who have discontinuity in frontal bone.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.