
Abstract
This is the case of a healthy 10-year-old girl presenting to the pediatric otolaryngology clinic for an incidental finding of a 20 mm dilatation within the left posterior fossa on brain computed tomography done for evaluation of left retro-auricular pain. Comprehensive audiometry showed left sensorineural hearing loss at low frequencies. Magnetic resonance imaging revealed a cystic lesion along the posterior aspect of the left temporal bone with normal inner ear anatomy consistent with an enlarged endolymphatic sac anomaly. This pathology is a rare entity with only one previously reported case in the literature.
Introduction
Nearly 80% of congenital sensorineural hearing loss originates from genetic factors, while the remaining 20% is due to acquired factors, typically stemming from prenatal infections. Hereditary causes primarily include autosomal recessive non-syndromic hearing loss, accounting for 80% of cases, with over 110 gene mutations linked to hearing loss. 1 Among these congenital conditions is the enlarged vestibular aqueduct (EVA), first identified by Mondini in 1791. In most cases, EVA is associated with other vestibulocochlear anomalies such as an enlarged vestibule, enlarged semicircular canals, or a hypoplastic cochlea. 2 Enlargement of the vestibular aqueduct can also lead to an enlarged endolymphatic duct and sac, either in isolation or as part of Pendred syndrome, causing progressive sensorineural hearing loss. However, isolated enlargement of the endolymphatic sac (ES) is an extremely rare condition, with only 1 case reported in the literature. 3 The authors aim to present the case of a pediatric patient with sensorineural hearing loss caused by an enlarged ES.
Case Presentation
A previously healthy 10-year-old girl presented to the pediatric otorhinolaryngology clinic due to an incidental finding of sinusitis on computed tomography (CT) scan, which also revealed a 20 mm dilation within the left posterior fossa. Imaging was initially requested by another physician because the patient complained of left retro-auricular pain during a viral illness. At the time of presentation, the patient reported no subjective hearing loss, tinnitus, or vertigo. Otoscopy showed normal ear canals with clear tympanic membranes. The nose and oral cavity were unremarkable and no retroauricular mass was palpated. Comprehensive audiometry was performed to rule out any hearing loss given the location of the left posterior fossa dilation in proximity to the cochlea. It revealed mild sensorineural hearing loss at low frequencies in the left ear (Figure 1a).
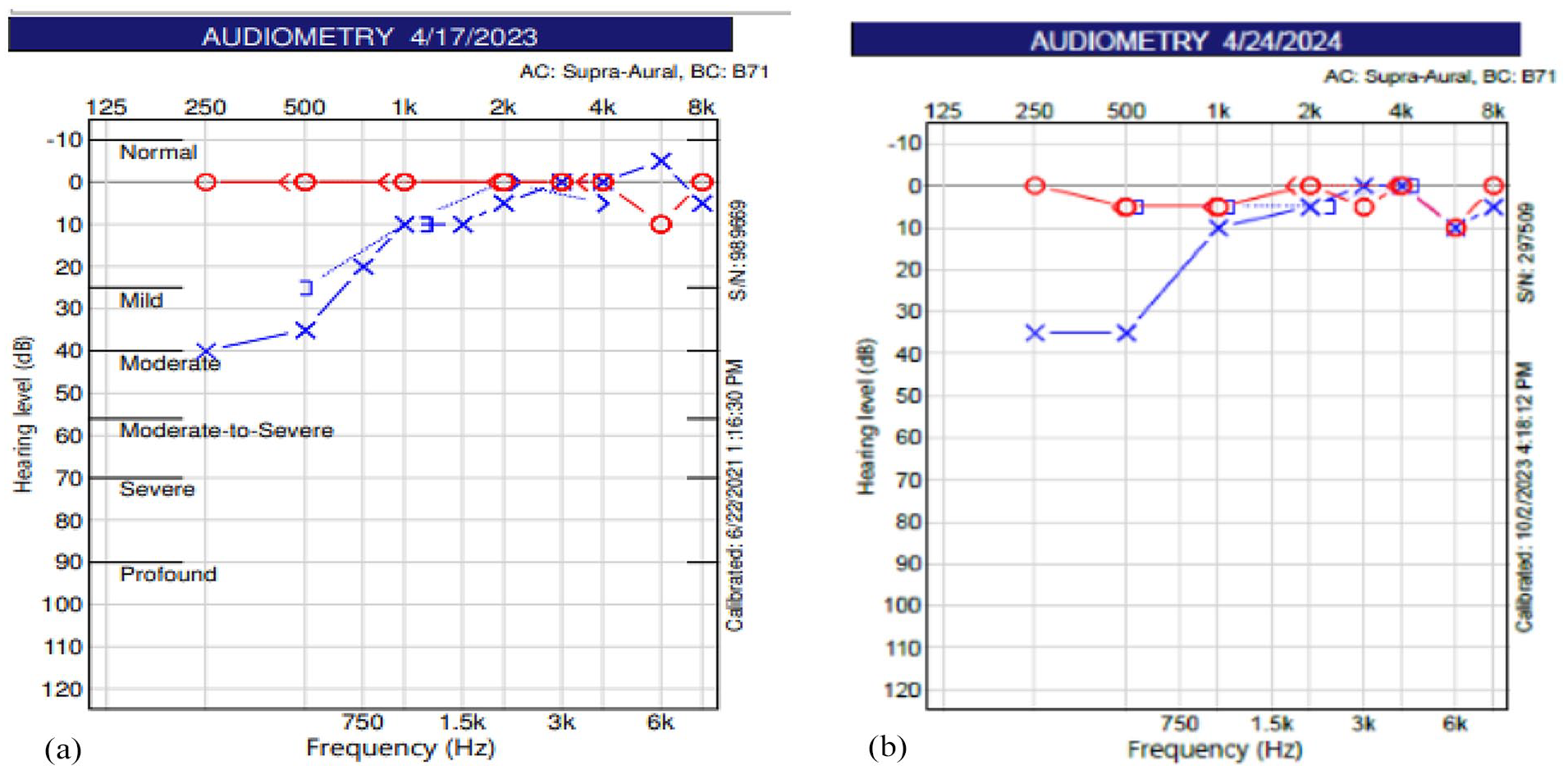
(a) Comprehensive audiogram showing mild sensorineural hearing loss at low frequencies in the left ear. (b) Same findings were observed at 1-year follow-up.
Brain magnetic resonance imaging (MRI) with gadolinium was requested for further evaluation and revealed an enlarged, oblong cystic lesion along the posterior aspect of the left temporal bone at the expected level of the ES, measuring 15 × 4 mm in its largest axial diameter. The inner ear anatomy was normal with no associated anomalies (Figure 2a). The patient was advised to avoid any head trauma and to follow-up in 1 year or earlier if any hearing deterioration. Imaging at a 1-year follow-up showed a stable enlarged ES with unchanged size (Figure 2b) and stable hearing loss on comprehensive audiogram (Figure 1b).
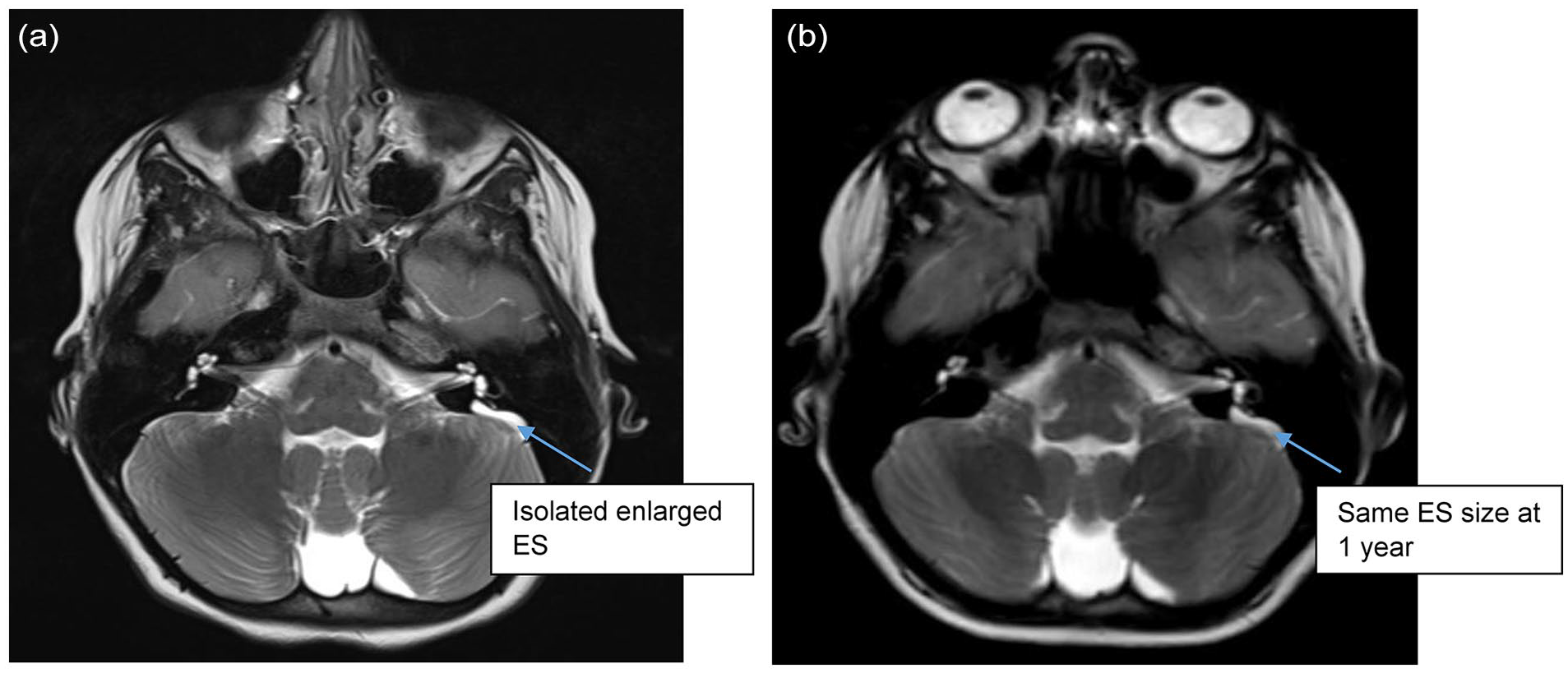
(a) T2-weighted MRI image in axial plane showing a left enlarged endolymphatic sac. Inner ear anatomy is normal. (b) Same findings were observed at 1-year follow-up. MRI, magnetic resonance imaging.
Written informed consent was obtained from the patient’s legally authorized representative for the publication of this case report.
Discussion
The ES is a non-sensory structure within the inner ear that plays a key role in regulating endolymph volume and ionic composition, thereby maintaining inner ear homeostasis. It is the distal portion of the endolymphatic duct and lies along the posterior surface of the petrous temporal bone beneath the dura. Unlike other labyrinthine components, the ES contains sodium-rich, potassium-poor fluid, helping regulate pressure and ionic balance within the inner ear. Disruption of this delicate homeostasis can lead to sensorineural hearing loss and vestibular symptoms. 4
Enlargement of the ES is most commonly seen in the context of EVA syndrome, which may also involve cochlear dysplasia, enlarged semicircular canals, or be part of Pendred syndrome—an autosomal recessive disorder associated with SLC26A4 gene mutations. However, isolated enlargement of the ES without associated EVA or inner ear malformations is exceedingly rare, with only one prior case reported in the literature. 3
The mechanism by which an isolated enlarged ES contributes to sensorineural hearing loss is not fully understood, but several theories have been proposed. According to the hydrostatic pressure hypothesis an enlarged ES may lead to increased endolymphatic fluid pressure within the cochlea, resulting in mechanical damage to hair cells—similar to the pathophysiology of Ménière’s disease. When considering the ionic imbalance hypothesis, alterations in fluid resorption and ion transport within an enlarged ES can disrupt cochlear electrochemical gradients, impairing auditory transduction. The hypothesis of direct neural damage assumes that persistent endolymphatic distention may cause neuroinflammatory changes or compressive effects on cochlear nerve fibers, further contributing to hearing loss. 2
This pathology often presents with progressive or fluctuating low-frequency sensorineural hearing loss, as seen in our patient. The low-frequency predominance is thought to result from early damage to the apical cochlear turn, which encodes lower sound frequencies. Importantly, when encountering a cystic lesion at the posterior petrous bone, differential diagnosis must include EVA, diagnosed when the vestibular aqueduct midpoint diameter exceeds 1.5 mm and ES tumors which are rare, slow-growing, but locally aggressive papillary neoplasms often associated with von Hippel-Lindau syndrome. These tumors appear heterogeneous on MRI with intense post-contrast enhancement, often showing bone erosion and calcifications on CT. 5 In our case, radiologic features excluded an ES tumor and supported a benign ES anomaly.
There is currently no standardized treatment for isolated ES enlargement. Management is typically conservative, focused on hearing preservation and trauma avoidance. Follow-up with serial audiograms and imaging is prudent, especially in pediatric patients, given the potential for progressive hearing loss. Hearing aids or cochlear implantation may be considered if hearing deteriorates.
Conclusion
An enlarged ES associated with low-frequency sensorineural hearing loss is an extremely rare anomaly, with only one previously reported case in the literature. The mechanism of low-frequency hearing loss may be related to the disruption of endolymphatic fluid homeostasis and increased pressure, similar to endolymphatic hydrops. The optimal follow-up period and management options for this condition remain unclear.
Footnotes
Ethical Considerations
The Institutional Review Board of the authors’ affiliation determined that review and approval by the IRB is not required.
Consent to Participate
Written informed consent was obtained from the patient’s legally authorized representative for the publication of this case report.
Author Contributions
Anne Marie Daou: Investigation, Data curation, Writing – original draft.
Jad Hosri: Resources, Writing – original draft.
Randa Barazi: Supervision, Project administration, Writing – review & editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.