
Abstract
Opioid-induced hearing loss has been described as a form of sudden sensorineural hearing loss that can occur with chronic or acute opioid use. Here, we report a case of a 16-year-old patient with sudden onset hearing loss after opioid overdose requiring prolonged intubation with fentanyl sedation.
Case
A 16 year old previously healthy male presented as a transfer in profound hypotensive shock and acute respiratory failure. He was found cyanotic and unresponsive after taking an unknown drug that he had purchased illicitly over the social media platform InstagramTM. He was unresponsive to Narcan, required intubation, and pressor support prior to transfer due to profound hypoxia and persistent hypotension. His urine drug screen was positive for synthetic opiates. Toxicology recommended a designer opioid panel which was positive for 4-ANPP, a precursor to fentanyl. Head CT showed no abnormal findings. There was no evidence of anoxic brain injury. He received a single dose of vancomycin for empiric coverage of aspiration before being switched to oral antibiotics. He remained intubated on sedation with dexmedetomidine and fentanyl infusions for 2 days.
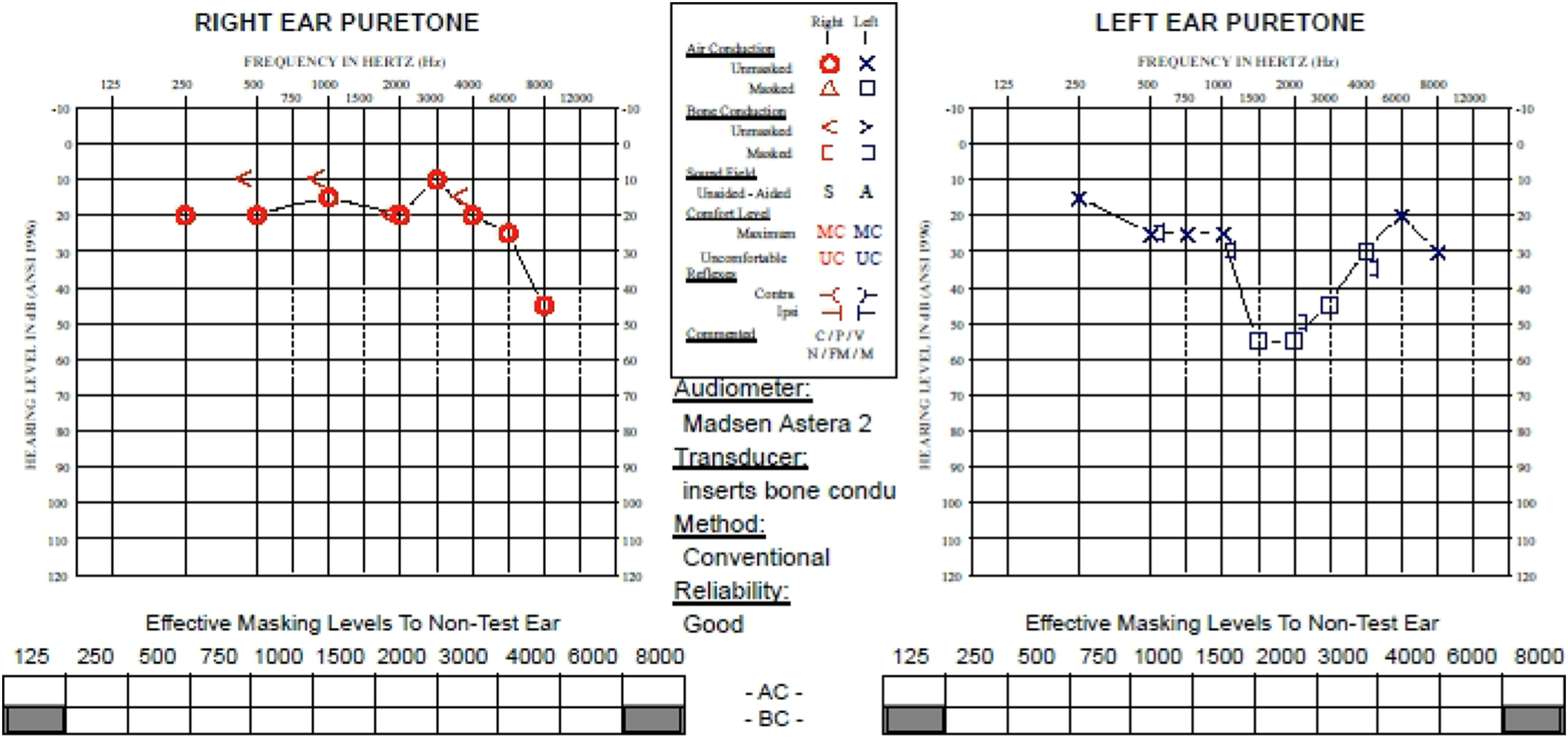
Following extubation, the patient reported bilateral hearing loss with associated intermittent, high-pitched tinnitus. He denied ear pain, fullness, or otorrhea. His ear exam was normal. There was no prior diagnosis or evidence of an existing hearing loss. On exam, there was no evidence of neurologic impairment. Audiogram demonstrated moderately severe sensorineural hearing loss bilaterally with word recognition scores of 54% at 95 dB on the right and 48% at 95 dB on the left (Figure 1). Based on these results and the acute onset of hearing loss he was treated with a high dose steroid taper. Repeat audiogram, 1 month after onset of hearing loss, revealed improvement in pure-tone audiometry on the left and near-resolution on the right. Word recognition scores improved to 96% at 80 dB on the right and 100% at 80 dB on the left (Figure 2). Audiogram obtained at time of first complaint of hearing loss. Results show bilateral moderately severe sensorineural hearing loss. Follow-up audiogram obtained one month after initial complaint of hearing loss. Results show normal hearing at 350–4000 Hz sloping to moderate hearing loss at 6000–8000 Hz on the right. On the left, results show normal hearing sloping to moderate hearing loss and rising to normal hearing in a notch configuration.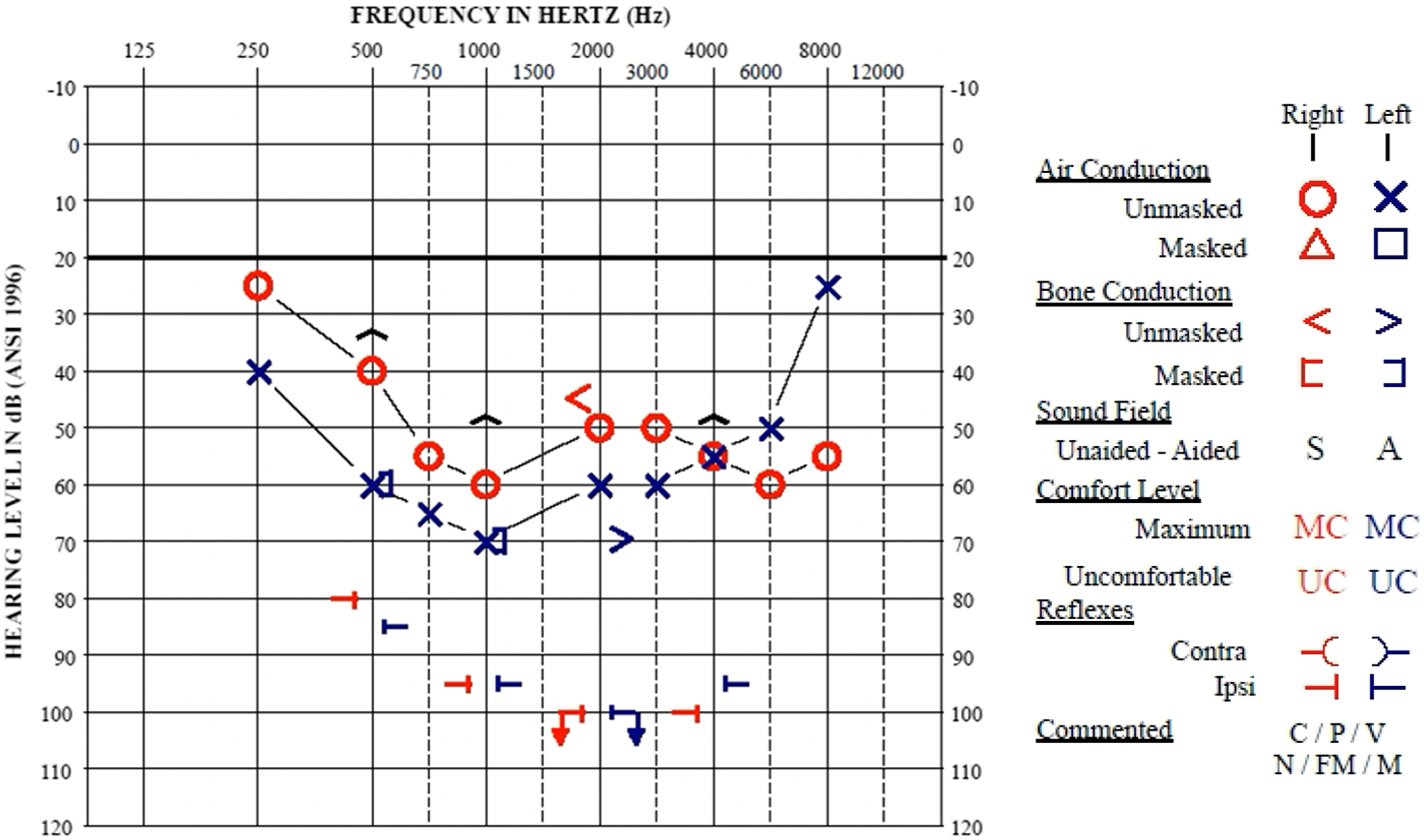
Discussion
There are several factors that may have contributed to sensorineural hearing loss in this patient, including anoxic brain injury, vancomycin administration, and opioid exposure. In this case, the patient had no other neurologic findings or changes in mental status that would be suggestive of anoxic brain injury. Vancomycin has been associated with ototoxicity. However, the risk of hearing loss is small and found primarily in patients on long term therapy. A small percentage of patients on long term vancomycin therapy were found to have hearing changes. 1 This patient only had a single dose of vancomycin. Therefore, opioids were deemed to be the most-likely causative factor leading to his hearing loss.
Opioid-induced hearing loss has been described in small retrospective reviews and case reports. One study of 41 cases over 20 years found that ototoxicity from opioids was most commonly associated with heroin (22 cases) followed by oxycodone (7 cases). 2 Hydrocodone, methadone, and morphine have also been associated with SNHL in various case reports.3-8
The mechanism behind opioid-induced hearing loss is an area of active research. One theory is that opioid receptor activation modulates the afferent response to acoustic stimuli and cochlear mechanics. 9 Another theory posits opioid-induced vasospasm leading to hypoperfusion of the vestibulocochlear system. 10
This patient with opioid-induced hearing loss improved with high dose steroid taper. According to the current clinical practice guidelines (CPG) from the American Academy of Otolaryngology, 11 treatment with high dose steroids is an option for sudden onset sensorineural hearing loss. The CPG notes that only one of three randomized control trials had patients receive benefits from oral steroids. The greatest recovery is when steroid therapy is initiated in the first two weeks. This patient initiated therapy less than 7 days from symptoms onset and had moderately severe hearing loss at a young age, making steroid therapy a recommended treatment in this case. The prognosis for opioid-induced sudden onset sensorineural hearing loss is variable. Unlike the patient presented in this case report, patients in prior case reports with opioid-induced hearing loss did not benefit from treatment with high dose steroid taper.4,5 While further research is needed to understand the pathophysiology of opioid-induced sudden sensorineural hearing loss, we believe empiric therapy with a high dose steroid taper is reasonable, in patients without contraindications, given the potential for improvement.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.