
Abstract
Background:
Hearing loss is a significant public health issue in the United States, affecting an estimated 72.9 million people, or 22% of the population. Despite its prevalence and clinical impact, insurance coverage for hearing-related interventions remains inconsistent. Given these factors, particularly in the Medicare population, examining trends in hearing loss, co-occurring conditions, and utilization of audiologic services is essential to understand the burden of hearing impairment and identify gaps in care.
Objective:
To examine 10-year trends in hearing loss and cochlear implant use, along with access to audiologic services and geographic variation among Medicare beneficiaries.
Methods:
Data from the Center for Medicare and Medicaid Services were used to plot the mean prevalence of deafness/hearing impairment overtime from 2012 to 2022, calculate the relationship between deafness/hearing impairment and common comorbidities, and determine the total number of audiometry evaluations, hearing aid assessments, hearing aid supplies and accessories, and cochlear implant surgeries for Medicare beneficiaries in the United States.
Results:
The average prevalence of hearing impairment for Medicare beneficiaries showed a significant increase from 2012 to 2022 (P < .01). The number of cochlear implant surgeries had a significant increase over this period, increasing from 1705 to 2828 procedures (R = .8, P < .01). Most chronic conditions had a statistically-significant relationship with deafness/hearing impairment (P < .001). Hyperlipidemia (R = .3, P < .001), anxiety (R = .2, P < .001), and depression (R = .3, P < .001) had the strongest relationships with deafness and hearing impairment. Urban counties (mean = 6.3%, SD = 1.7) had a statistically-significant higher prevalence of deafness/hearing impairment than rural counties (mean = 4.9%, SD = 1.7, P < .001).
Conclusion:
The significant increase in hearing impairment from 2012 to 2022 emphasizes the need for expanded screening, treatment, and management strategies for geriatric patients. Addressing hearing impairment among older individuals may improve physical, mental, and spiritual well-being.
Introduction
Hearing loss is a significant public health issue in the United States, affecting an estimated 72.9 million people, or 22% of the population, as of 2019. 1 The prevalence of hearing loss increases with age,2 -4 with nearly 96% of individuals aged 90 years and older experiencing some form of hearing loss. 3
Beyond its prevalence, hearing loss is associated with numerous chronic health conditions, including diabetes, cardiovascular disease, arthritis, and stroke.4 -8 It is also associated with cognitive decline and dementia,9,10 with one study reporting a 79% prevalence of hearing loss among individuals with dementia. 10 Moreover, hearing loss also contributes to psychosocial challenges, such as depression, anxiety, social isolation, and loneliness.11 -13
Despite its widespread effects, hearing loss is a modifiable condition for which interventions, such as hearing aids, can significantly improve hearing and quality of life. 14 However, hearing aid utilization varies widely among Americans with hearing loss, ranging from 12.7% in adults aged 20 years and older to 40.0% in adults aged 70 years and older15 -18 Factors influencing hearing aid use include stigma associated with wearing hearing aids, access to care, awareness of hearing loss, cost, and insurance coverage.19 -23 Insurance coverage for hearing aids and other interventions varies significantly by insurance plans. For example, Medicare (Parts A and B), which provides coverage to 67.3 million US adults, does not cover hearing aids or exams for fitting hearing aids.24 -26 Only 28 states provide some coverage for adults dually eligible for Medicaid and Medicare, but the coverage varies based on hearing loss severity and eligibility criteria. 27
Given the high prevalence of hearing loss among older adults, its association with multiple chronic conditions, and variability in access to hearing-relating interventions – particularly with the Medicare population – research examining longitudinal trends in hearing impairment, co-occurring conditions, and the utilization of audiologic services is critical to understand the burden of hearing impairment and gaps in care. Thus, the aim of this study was to analyze the 10-year trends in the prevalence of hearing loss and cochlear implant use, while examining data on audiologic services to explore treatment access and geographic variation among Medicare beneficiaries. We focused on Medicare beneficiaries because Medicare insures the majority of adults aged 65 years and older, the population most affected by hearing loss. Using population-level data, we assessed audiologic service use and regional disparities to better understand gaps in access to hearing care across the United States. Additionally, we examined associations between hearing loss and common comorbidities to identify high-risk populations.
Methods
Ethics Approval
This research is exempt from institutional review board (IRB) review and does not qualify as human subject research under federal regulations, as it used de-identified, publicly-available data. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were followed in this study. 28
Data Source
The data utilized in this research study were sourced from the Center for Medicare and Medicaid Services (CMS).29,30 The CMS provided variables that included the prevalence of various chronic conditions and Physician/Supplier Procedure Summary (PSPS) counts for Medicare beneficiaries through the Mapping Medicare Disparities tool and PSPS dataset.29,30
Variables
The following variables are chosen because of their connections to hearing impairment and common diagnostic tests and treatments for hearing impairment. Data for deafness/hearing impairment were examined longitudinally from 2012 to 2022. All remaining variables were selected from the year 2022 to ensure consistency across data sources and to reflect the most recent complete year of available data. This decision allowed for temporal alignment among variables such as the number of chronic conditions, audiometry evaluations, hearing aid assessments, hearing aid supplies/accessories, and cochlear implants. Although more recent data were available for some variables, we used data from 2022 to maintain uniformity in the analytic timeframe. The complete list of the variables and how they were defined is as follows:
Deafness/Hearing Impairment
The percentage of Medicare beneficiaries who were diagnosed with hearing impairment and deafness from 2012 to 2022. 29 Diagnosis of hearing impairment and deafness was determined based on ICD-10/HCPCS codes H90 and H91, which include conductive, sensorineural, mixed, and unspecified types of hearing loss. 31 Diagnosis was determined by the provider’s clinical judgment as documented in the medical records, unknown of the use of formal audiometry. 32
Chronic Conditions
The percentage of Medicare beneficiaries who have a specified illness, disease, disorder, or injury in 2022. 29 We used data from 2022 to focus on recent health trends. Additional information on the definition and how each of the conditions were diagnosed is available on the CMS website. 33
Comprehensive Audiometry Evaluation
The number of binaural hearing tests (CPT/HCPCS code 92557). 30
Hearing Aid Assessment
The number of hearing aid assessments (CPT/HCPCS code V5010). 30
Hearing Aid Supplies and Accessories
The number of hearing aid supplies and accessories necessary to meet a recipient’s specific hearing aid needs (CPT/HCPCS code V5267). 30
Cochlear Implant Surgery
The number of cochlear implant procedures, an electronic device that provides a sense of hearing to people with profound sensorineural hearing loss (CPT/HCPCS code 69930). 30
Statistical Analysis
This study investigated the prevalence of hearing impairment and other chronic conditions, and how that related to the frequency of audiometry evaluations and interventions for deafness/hearing impairment.
The mean prevalence of deafness/hearing impairment across counties in the United States was plotted over time from 2012 to 2022. The mean county prevalence of various chronic conditions was calculated for the year 2022 by dividing the number of people diagnosed with each condition by county population. The relationship between deafness/hearing impairment and common comorbidities was calculated using Pearson correlation tests to determine statistical significance.
The total number of audiometry evaluations, hearing aid assessments, hearing aid supplies and accessories, and cochlear implant surgeries for Medicare beneficiaries in the United States were summed and plotted from 2012 to 2022. The total number of procedures were then broken down by state/jurisdiction based on the carrier number. The approximate number of procedures per 100 000 persons was used to calculate the mean rate of each procedure performed for hearing impairment in 2022.
The mean rate of each procedure performed for hearing impairment was regressed with the average prevalence of deafness/hearing impairment for each state/jurisdiction using Pearson correlation tests to determine statistical significance. Values that were percentages were not weighted, such as the prevalence of various chronic conditions. However, values measuring rates, such as the number of procedures performed for hearing impairment per 100 000 beneficiaries, were weighted.
Geospatial analysis calculated the prevalence of deafness/hearing impairment for rural and urban counties in the United States and compared them via t-test. Rural and urban county classification was determined by the Centers for Medicare and Medicaid Services and the Mapping Medicare Disparities tool. The categorization of urban and rural counties stems from the United States Office of Management and Budget, which designates counties as metropolitan (population of at least 50 000), micropolitan (population of at least 10 000), or neither. CMS designated counties with an urban core of at least 10 000 people as urban and all other counties as rural. 34
All statistical tests were conducted with a significance level of α = .05 unless otherwise specified. This project used RStudio (Boston, MA), version 2023.03.1+446, for statistical tests and figures.
Results
This project analyzed a total of 3218 counties across the United States and territories. The mean prevalence of deafness/hearing impairment was calculated across 10 years for counties in the United States (Figure 1). The average prevalence of hearing impairment for Medicare beneficiaries showed a significant increase from 2012 to 2022 (P < .01). Every year showed an average of 0.2% increase in the prevalence of hearing impairment. In 2012, the mean county prevalence of hearing impairment in the United States was 3.2% (SD = 1.3). This rose to 5.5% (SD = 1.8) in 2022. Therefore, there was a 70.4% increase in the overall prevalence of hearing impairment from 2012 to 2022.
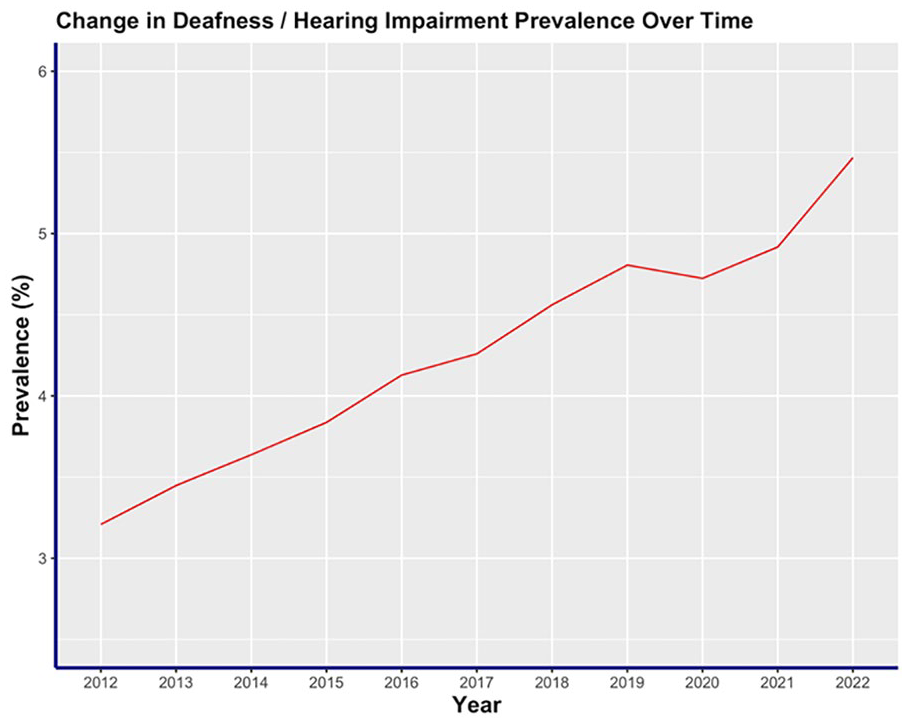
Time plot of the mean prevalence of deafness and hearing impairment across counties in the United States from 2012 to 2022.
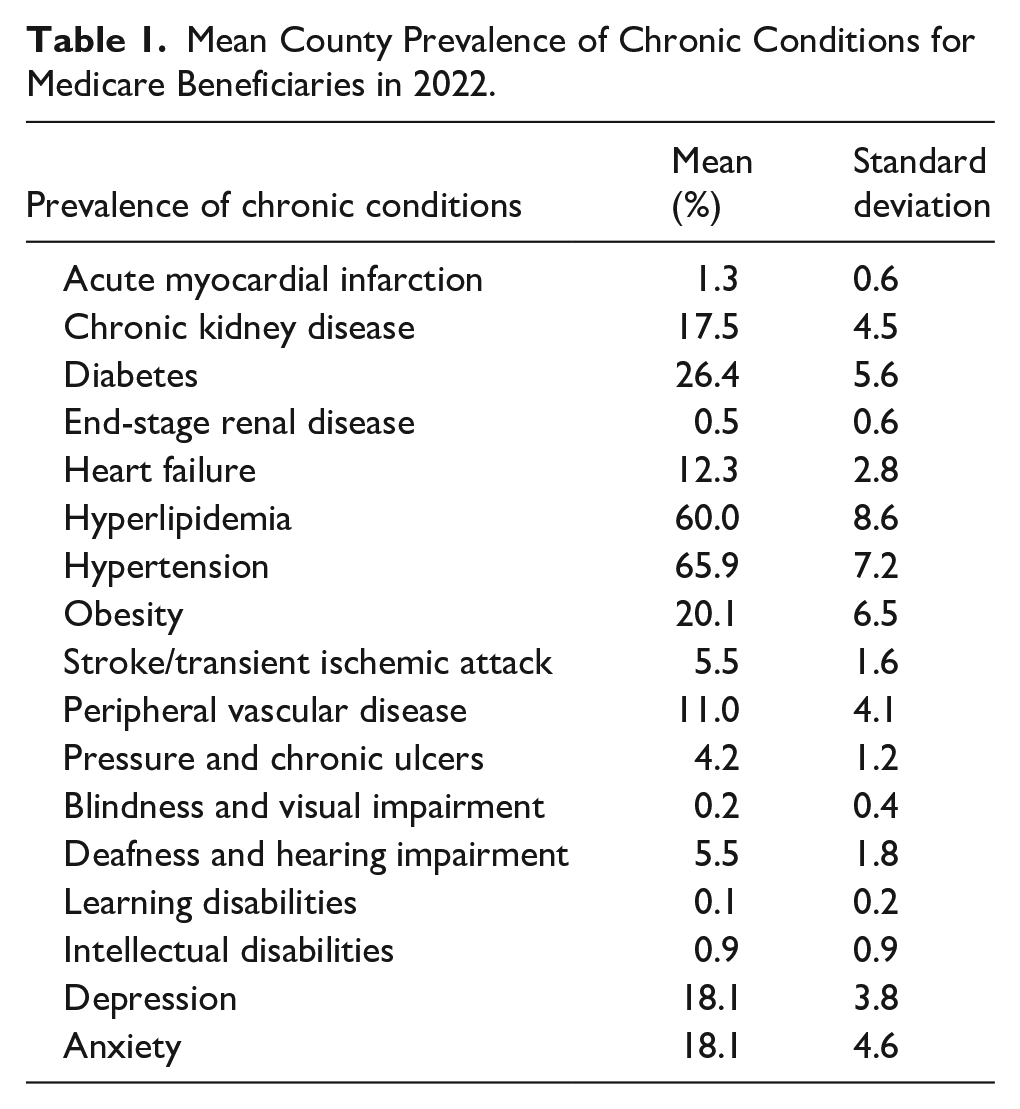
The mean prevalence of various chronic conditions for counties in the United States was calculated (Table 1). Of the chronic condition selected, hypertension (mean = 65.9%, SD = 7.2), diabetes (mean = 26.4%, SD = 5.6), and obesity (mean = 20.1%, SD = 6.5) showed the highest prevalence among Medicare beneficiaries. Learning disabilities (mean = 0.1%, SD = 0.2) and intellectual disabilities (mean = 0.9%, SD = 0.9) had the lowest prevalence among Medicare beneficiaries.
Mean County Prevalence of Chronic Conditions for Medicare Beneficiaries in 2022.
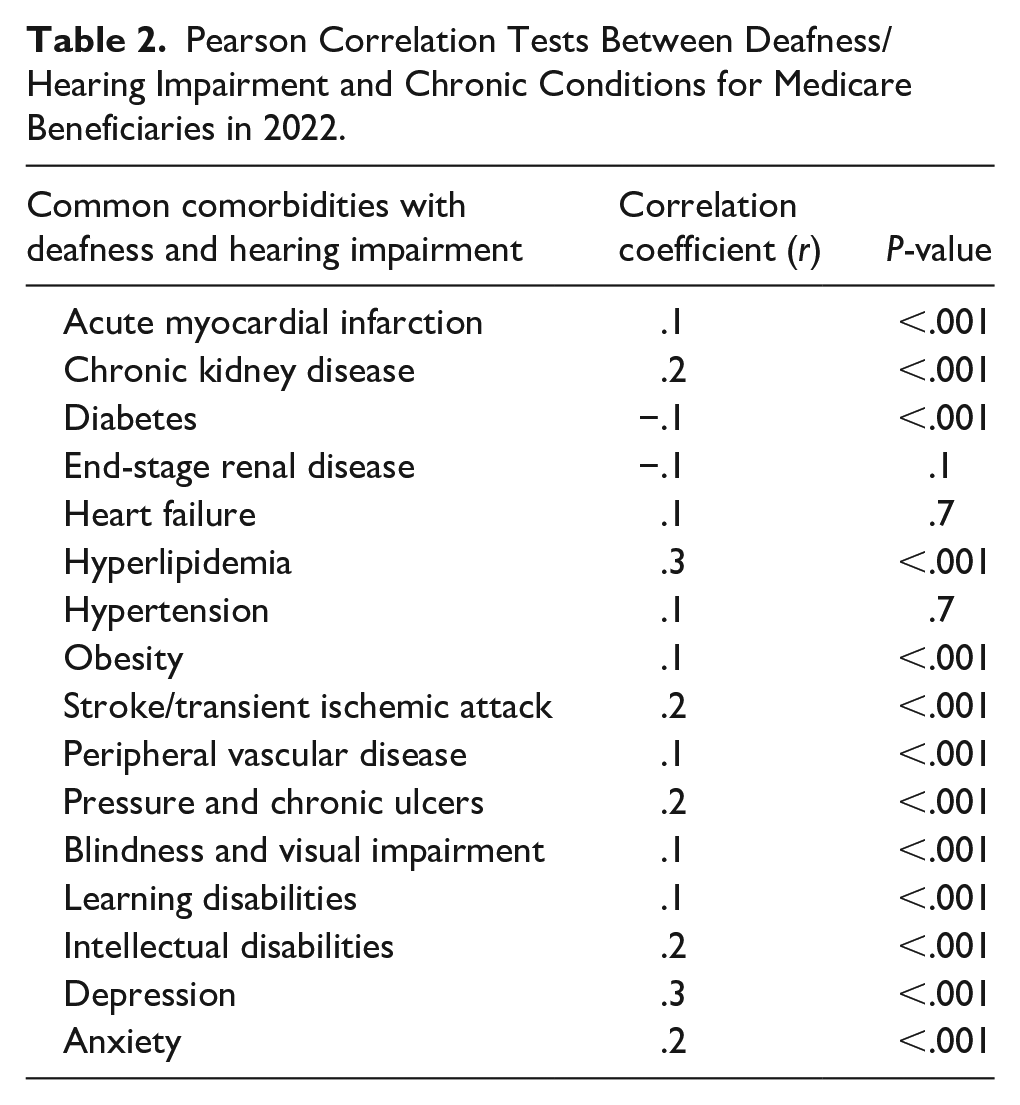
The relationship between deafness/hearing impairment and common chronic conditions was analyzed (Table 2). Most chronic conditions had a statistically-significant relationship with deafness/hearing impairment (P < .001). Hyperlipidemia (R = .3, P < .001), anxiety (R = .2, P < .001), and depression (R = .3, P < .001) had the strongest relationships with deafness and hearing impairment. Interestingly, diabetes had a statistically-significant negative relationship (R = −.1, P < .001).
Pearson Correlation Tests Between Deafness/Hearing Impairment and Chronic Conditions for Medicare Beneficiaries in 2022.
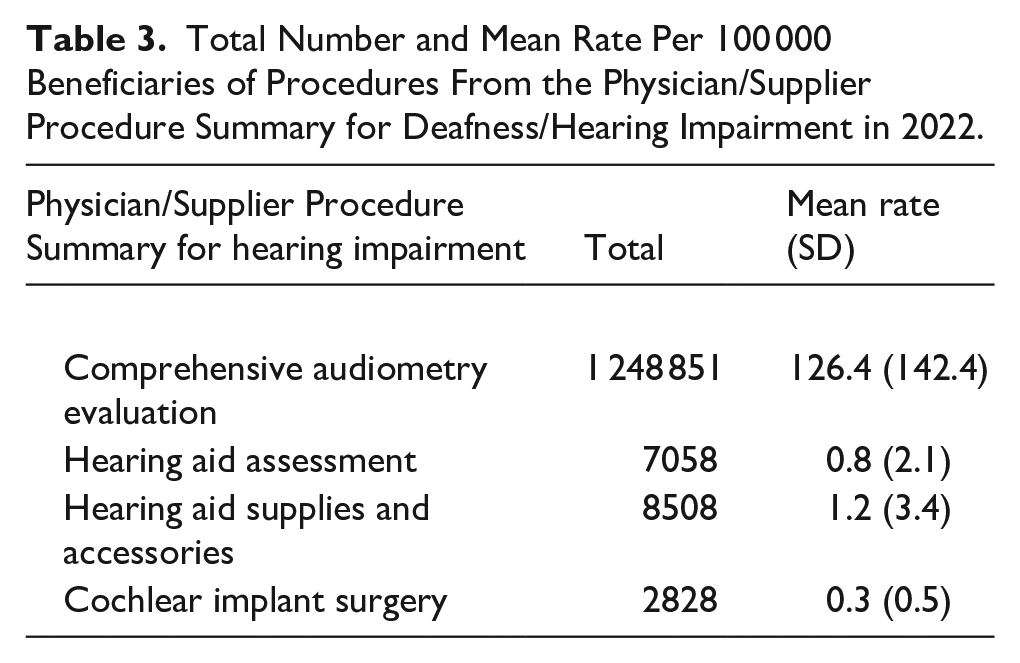
The frequency of audiometry evaluations, hearing aid assessments, hearing aid supplies and accessories, and cochlear implant surgeries for Medicare beneficiaries in the United States was calculated for 2022 (Table 3). There was a total of 1 248 851 audiometry evaluations, which had a mean rate of 126.4 (SD = 142.4) per 100 000 beneficiaries. Cochlear implant surgery was the least common procedure performed, with a total of 2828 surgeries.
Total Number and Mean Rate Per 100 000 Beneficiaries of Procedures From the Physician/Supplier Procedure Summary for Deafness/Hearing Impairment in 2022.
Pearson correlation tests between hearing impairment and performed procedure rates across states/jurisdictions were not found to be statistically significant for comprehensive audiometry evaluation (R = .1, P = .9), hearing aid assessment (R = .1, P = .7), hearing aid supplies and accessories (R = .2, P = .2), or cochlear implant surgery (R = .1, P = .5).
The number of procedures and interventions for deafness/hearing impairment were plotted over time from 2012 to 2022 (Figure 2). The number of cochlear implant surgeries had a significant increase over this period, increasing from 1705 to 2828 procedures (R = .8, P < .01). This equates to a 65.9% increase in the number of cochlear implant surgeries. Additionally, hearing aid supplies and accessories had a statistically-significant increase in the number of procedures performed (R = .6, P < .03). The number of hearing aid assessments (R = .1, P = .7) and comprehensive audiometry evaluations (R = .3, P = .3) did not have a significant increase over the ten years examined. All four procedures analyzed in this study decreased in response to the COVID-19 pandemic in 2020.
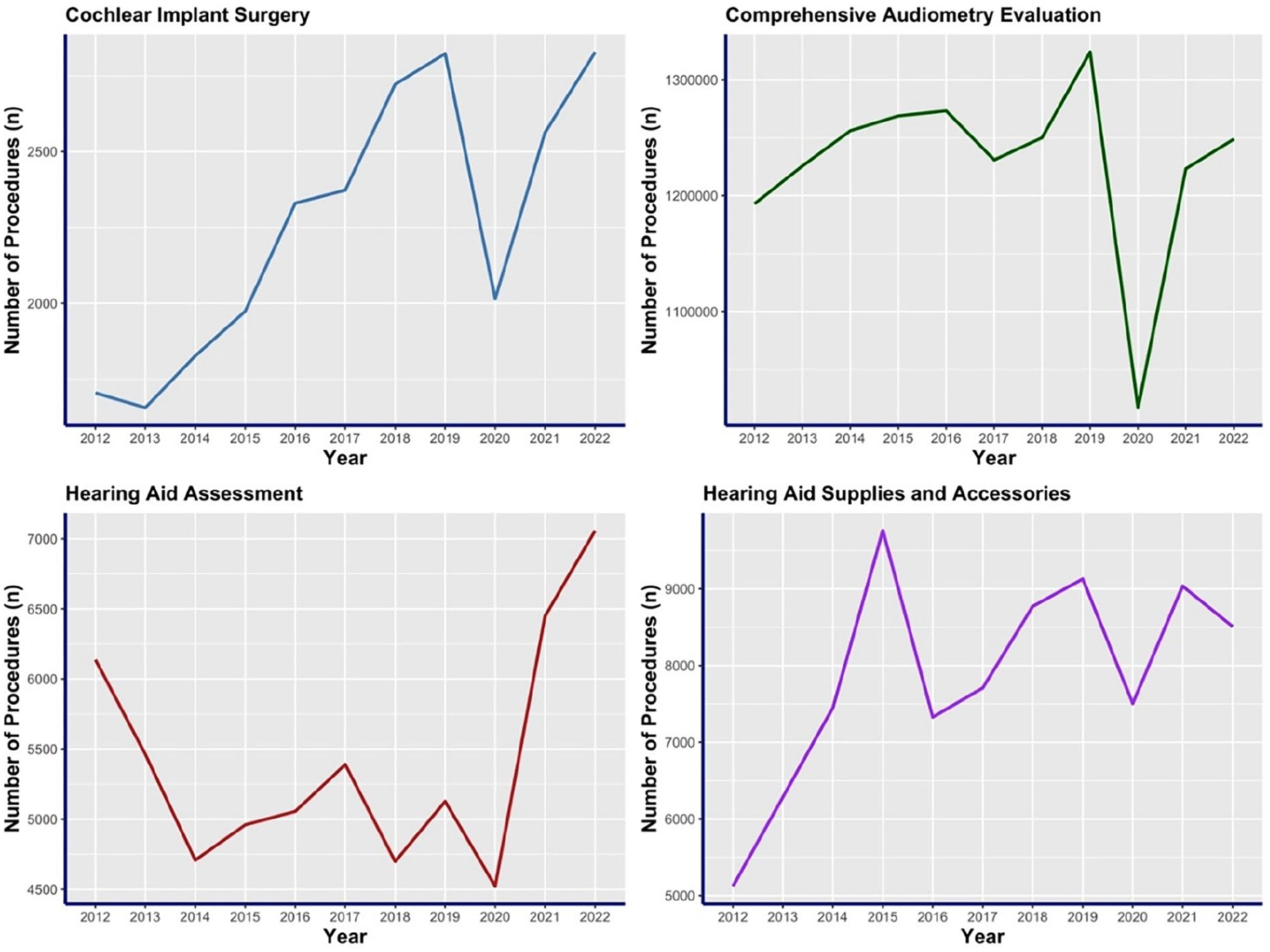
The number of procedures and interventions from the Physician/Supplier Procedure Summary for deafness/hearing impairment for Medicare beneficiaries in the United States from 2012 to 2022.
The mean prevalence of hearing impairment for Medicare beneficiaries in 2022 was compared between rural and urban counties in the United States (Figure 3). Urban counties (mean = 6.3%, SD = 1.7) had a statistically-significant higher prevalence of deafness/hearing impairment than rural counties (mean = 4.9%, SD = 1.7, P < .001). On average, urban counties had 1.4 more patients with hearing impairment than rural counties per 100 people.
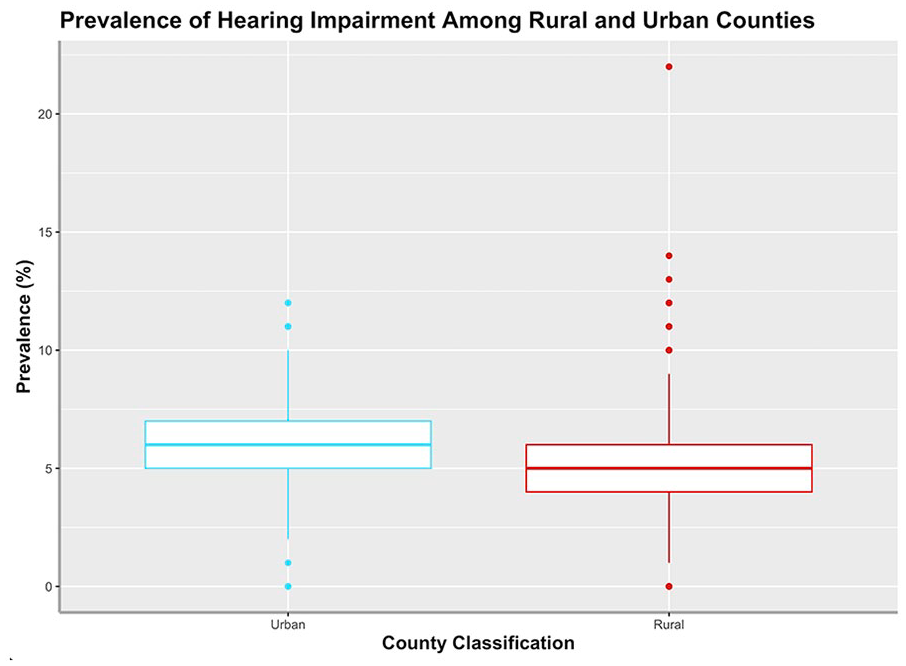
Prevalence of hearing impairment/deafness among rural and urban counties in the United States in 2022.
Discussion
This study analyzed trends over time and treatment patterns, as well as geospatial differences in hearing impairment among Medicare beneficiaries. It also examined the association between hearing impairment or deafness and common comorbid conditions. The findings reveal several critical insights with implications for public health and health care policy.
This study found that the mean prevalence of deafness/hearing impairment for Medicare beneficiaries increased significantly from 2012 to 2022. The mean prevalence of hearing impairment rose by average of 0.2% annually. In total, the prevalence of hearing impairment in 2022 (5.5%) was 70.4% higher than in 2012 (3.2%). The growing burden of hearing-related disabilities in the aging population underscores the importance of and the need for expanded screening and management strategies. The primary cause of hearing loss in the geriatric population can be attributed to aging. However, additional causes of hearing loss are labor complications, infections, noise exposure, diabetes, and ototoxic medications. 1
While this study observed rising prevalence among Medicare beneficiaries, previous studies that tracked hearing loss among adults showed decreasing prevalence.35,36 This discrepancy emphasizes the importance of specifically researching severe hearing loss among the older population. Medicare beneficiaries are generally members of the older population, usually over the age of 65, unless they have been diagnosed with certain chronic or disabling conditions. 29 Additionally, most studies research the effects of hearing loss of all levels of severity.1,3,35,36 This project focused on severe hearing loss, which manifested as a diagnosis of deafness/hearing impairment. Therefore, the present study’s focus on a subset of the population with more severe impairment offers a distinct epidemiologic insight that may explain contrasting national trends. This insight highlights a new trend in public health for older adults with severe hearing difficulties.
Of the 17 chronic conditions analyzed in this project, deafness and hearing impairment was ranked as the tenth most prevalent. The prevalence of hearing impairment among Medicare beneficiaries indicates the need for appropriate treatment of the condition and downstream symptoms. For example, hearing impairment often correlates with people experiencing tinnitus, or a sensation of hearing a noise with no external source – affecting approximately 14.4% of adults. 37 Cochlear implants and hearing aids are potential treatments for patients with hearing loss and tinnitus.34,38 Given the rising burden of severe impairment, cochlear implants may represent an underused intervention to improve the quality of life in this population.
The broader impacts that deafness and hearing impairment have on physical, mental, and spiritual well-being cannot be understated. Hearing impairment has previously been linked to many comorbidities.4 -13 This project is consistent with previous studies and found that cardiovascular disease, chronic kidney disease, hyperlipidemia, obesity, stroke/transient ischemic attack, peripheral vascular disease, pressure and chronic ulcers, blindness and visual impairment, learning disabilities, intellectual disabilities, depression, and anxiety all significantly correlate with deafness/hearing impairment.4 -13 Interestingly, the comorbidities with the strongest relationship with deafness/hearing impairment were hyperlipidemia, anxiety, and depression. Our findings regarding hyperlipidemia align with those of Orita et al, 4 who found that hyperlipidemia increases the risk of microvascular disorders and negatively affects hearing prognosis. Hearing impairment leads to loneliness and social isolation, which can exacerbate feelings of depression.11,12 Accordingly, interventions to mitigate hearing loss are critical to mental and social well-being. Appropriate treatment and interventions that enhance the hearing of individuals with deafness may enhance their communication skills and mitigate symptoms of loneliness and depression.
An unexpected finding was the negative relationship between diabetes prevalence and deafness/hearing impairment. One explanation of this relationship is the geospatial differences between the two conditions. Diabetes tends to have the highest prevalence in the southern United States. However, deafness/hearing impairment clustered around the northeast and western counties of the United States. The differences in prevalence among these regions in the United States may be due to confounding variables such as demographic differences, racial and ethnic composition, health care access, and socioeconomic factors not examined in the current study.
Despite more people experiencing hearing impairment, the study highlights significant gaps in hearing health care. While audiometry evaluations totaled over one million services for Medicare beneficiaries in 2022, cochlear implant surgeries were rare, with just 2828 performed nationwide. Moreover, there was no significant correlation between hearing impairment and the rate of hearing-related procedures across states/jurisdictions. This could point to inequities in access to care, possibly due to financial barriers, a shortage of providers, or limited awareness about available hearing treatments among patients and health care professionals. In addition, the number of cochlear implant surgeries performed from 2012 to 2022 significantly increased. While the number of cochlear implant procedures increased, there are still approximately 1.3 million untreated audiometric cochlear implant candidates. 39 Previous studies attribute this large gap in care to financial barriers and the expensive cost of a cochlear implant.39,40
Comprehensive audiometric evaluations provide an important baseline for monitoring changes in hearing over time, especially in older populations. However, this study found that the number of comprehensive audiometric evaluations did not increase from 2012 to 2022. It should be noted that the impact of COVID-19 may have artificially lowered the number of procedures for each of the interventions examined in this study, particularly in 2020. Implementing comprehensive audiometry evaluations, along with proper usage of hearing aids, could serve as a preventative strategy for falls in geriatric patients, as hearing impairment has been found to increase the incidence of falls. 41 Therefore, these findings suggest that the condition of an individual’s hearing should be an integral component of routine care, enabling timely interventions that improve stability, reduce dizziness, and ultimately lower the risk of falls in the elderly population.
This study found that the prevalence of hearing impairment among urban counties was significantly higher than that of rural counties. Urban areas experience higher rates of noise pollution from occupational and recreational noise. 42 The noise pollution may lead to increased sensorineural hearing loss. 42 Previous research has found that rural areas experience increased barriers to accessing services for hearing loss, which may artificially decrease the reported prevalence of hearing loss.43,44 The limitation in services may further potentiate adverse health outcomes. 44 Thus, addressing both urban noise exposure and rural barriers to health care may be important in developing effective public health interventions.
Overall, this study highlights the importance of addressing hearing impairment as a multifaceted public health issue. Strategies that increase access to hearing health care services, such as audiometry evaluations and hearing aids, may remove barriers to care. Additionally, enhancing education about the relationship between hearing impairment and chronic conditions and comorbidities may improve patients’ holistic well-being. Further research could investigate the mechanisms of the associations between hearing impairment and chronic conditions and comorbidities.
Limitations
This study has several limitations. First, while the study included a 10-year time series for the prevalence of hearing impairment and implant use, variables were available cross-sectionally, limiting the ability to determine causality or assess the status of hearing impairment following certain treatments. Cross-sectional studies also limit the ability to interpret temporal relationships. Additionally, we only used 2022 data for chronic conditions to focus on recent health trends. A longitudinal study that follows a cohort of people over time could further investigate the effect of treatments, aging, and chronic conditions on hearing impairment. Second, data from the PSPS dataset and Medicare beneficiaries are limited to billing codes, which lack clinical detail such as audiometric thresholds or hearing loss severity. Further, data from Medicare beneficiaries may not be generalizable to the broader population because the dataset includes adults aged 65 and older and those with qualifying disabilities. Relatedly, Medicare data are subject to variability in coding practices and underreporting or inaccurate attribution of procedures. Additionally, the dataset lacks demographic and contextual variables, such as race, income, education, noise exposure, chemical exposure, and other social determinants of health, which are critical to understand disparities in hearing health and access to care and increase the potential for confounding variables. Future studies should incorporate experimental controls, show changes in chronic conditions over time, and adjust for confounding variables to enhance the validity and reliability of the findings.
Conclusion
This study provides insights into the growing prevalence of hearing impairment among Medicare beneficiaries and its complex relationship with chronic conditions and health care utilization. From 2012 to 2022, there was a significant increase in hearing impairment prevalence among Medicare beneficiaries. This emphasizes the need for expanded screening, treatment, and management strategies for older adults. Additionally, this study found significant correlations between hearing impairment and chronic conditions such as hyperlipidemia, anxiety, and depression. Addressing hearing impairment among older individuals may improve physical, mental, and spiritual well-being. Geospatial differences in the prevalence of hearing impairment were discovered, where urban counties had significantly higher rates of hearing impairment than rural counties.
Footnotes
Ethical Considerations
The study made use of de-identified, publicly available data. As a result, this study did not require institutional review board (IRB) review and did not qualify as human subject research under federal regulations.
Author Contributions
SB and EAB provided substantial contributions to conception and design, acquisition of data and data analysis; SB and EAB provided substantial contributions to the interpretation of data; SB and EAB drafted the article; SB and EAB revised the article critically for important intellectual content; and SB and EAB gave final approval of the version of the article to be published. SB and EAB agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The current study was funded by Osteopathic Heritage Foundation Ralph S. Licklider, D.O. Endowed Professor in Behavioral Diabetes awarded to Dr. Elizabeth A. Beverly.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available in the Centers for Medicare & Medicaid Services (CMS): https://data.cms.gov/tools/mapping-medicare-disparities-by-population; ![]() .
.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
The authors used no AI or AI-assisted technologies in the writing process.