
Abstract
Background and objective:
In many medical centers, intraoperative imaging to determine the precise location of electrodes is part of the routine surgical program. However, the importance of this procedure has not yet been clearly established. This study aims to review the importance of intraoperative imaging in cochlear surgery and management measures.
Methods:
Keyword searches were conducted in CINAHL, EMBASE, PubMed, and Cochrane databases from 2024. Abstracts and full texts of articles were reviewed by independent evaluators.
Results:
The initial review identified 267 articles, of which 17 were eligible for inclusion in our study. There were no randomized controlled trials. Intraoperative imaging was performed in 917 cochlear implants. Nineteen implants were unsatisfactory (5.3%), and the management protocol was changed in 18 (94.7%). Sixty-nine cochlear implants underwent computed tomography (CT; 7 studies). CT was unsatisfactory in 2 implants, and the management was changed in both (1000%). Two studies evaluated fluoroscopy in patients undergoing cochlear implant.
Conclusion:
Intraoperative imaging can be useful in determining electrode placement in cochlear implant surgery. This method is not yet considered routine, but it appears useful in cases where the surgeon is uncertain about electrode placement or in cases of abnormal cochlear anatomy.
Introduction
Cochlear implantation is a treatment option for patients with hearing loss who do not have access to or are unwilling to use conventional hearing aids. Optimal function of the implanted cochlear implant depends on accurate electrode placement. Studies have shown that extracochlear electrode placement, inadequate electrode placement, and scala vestibular electrode placement are among the factors that impair the proper performance of the therapeutic procedure.1-7 Lassig et al, in a study of 58 patients undergoing cochlear implant surgery, showed that 13% of patients required correct electrode repositioning. 8
Accurate electrode placement with various available methods can reduce the need for revision surgery and optimize the treatment process. Methods for determining electrode placement include computed tomography (CT), fluoroscopy, 3D X-ray, and electrical stimulation.9-12 Despite these well-known methods, the importance of imaging in various medical centers is still challenging. On the other hand, this method is not very desirable due to the risk of complications from radiation exposure, especially in children or at-risk individuals, such as malignancies.13,14
Given the different imaging modalities and their different applications in different medical centers, the present study aimed to investigate the importance of intraoperative imaging in cochlear implantation cases. We hypothesized that imaging would be particularly beneficial in cases where the surgeon is uncertain about the exact location of the electrodes or in cases of abnormal cochlear.
Materials and Methods
Protocol
This study strictly follows the guidelines established by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.
Eligibility Criteria
We systematically reviewed all peer-reviewed articles related to intraoperative X-ray images in cochlear implants. To ensure our findings’ rigor and reliability, we assessed each article’s quality using 2 independent reviewers who carefully categorized the abstracts and titles of the articles. The inclusion and exclusion criteria for selecting articles were carefully defined, and all authors involved in the study reached a consensus on these criteria to maintain objectivity and transparency in our research process.
Database Search (Search Method, Inclusion and Exclusion Criteria)
We conducted our search using keywords in PubMed, Cochrane, CINAHL, Medline, and EMBASE from 2024. This search, with the restriction of the English language, examined all electronic and printed articles, considering the year of publication. The MeSH and terms cochlear implantation, intraoperative management, postoperative management, and imaging were used for the search. The search was also completed with the terms imaging, X-ray, tomography, and radiography. The next stage of the search was performed with the keywords electrode and electrode implantation. The articles were compared with each other, and duplicate articles were removed. Abstracts were reviewed for initial assessment and eligibility of the included studies. Studies conducted in the field of intraoperative imaging in cochlear implantation were selected. Studies outside this topic, studies in a non-English language, and non-human studies were excluded.
Two independent reviewers carefully categorized the abstracts and titles of the articles. Articles that did not meet the inclusion criteria or some articles were excluded on the advice of other authors. The remaining articles were then collected and categorized based on thematic similarity. After completing a complete list of eligible articles, patients in each study were categorized by age group, gender, number of implants, type of implant, cochlear anatomy, electrode type and number, and type of imaging procedure. Study outcomes such as patient satisfaction, need for corrective surgery, and imaging outcomes were assessed.
The risk of bias of the authors of the articles was assessed. The Newcastle–Ottawa criteria were used to assess the quality of non-randomized studies. This scale was evaluated by considering the selection of patients, the review and comparison of cases, and the assurance of exposure. The type and number of electrode placement, the type of surgical procedure or its modification, and the type of imaging were examined.
Results
After the initial review, 267 studies were considered for review. Of these, 6 were duplicated and 166 were irrelevant or non-human. A total of 39 articles remained for evaluation, of which 1 was excluded due to unavailability of full text and 2 were non-English. Nineteen articles examined postoperative imaging and were excluded. Finally, data from 17 articles, including 1006 cochlear implant cases, were reviewed (Figure 1).
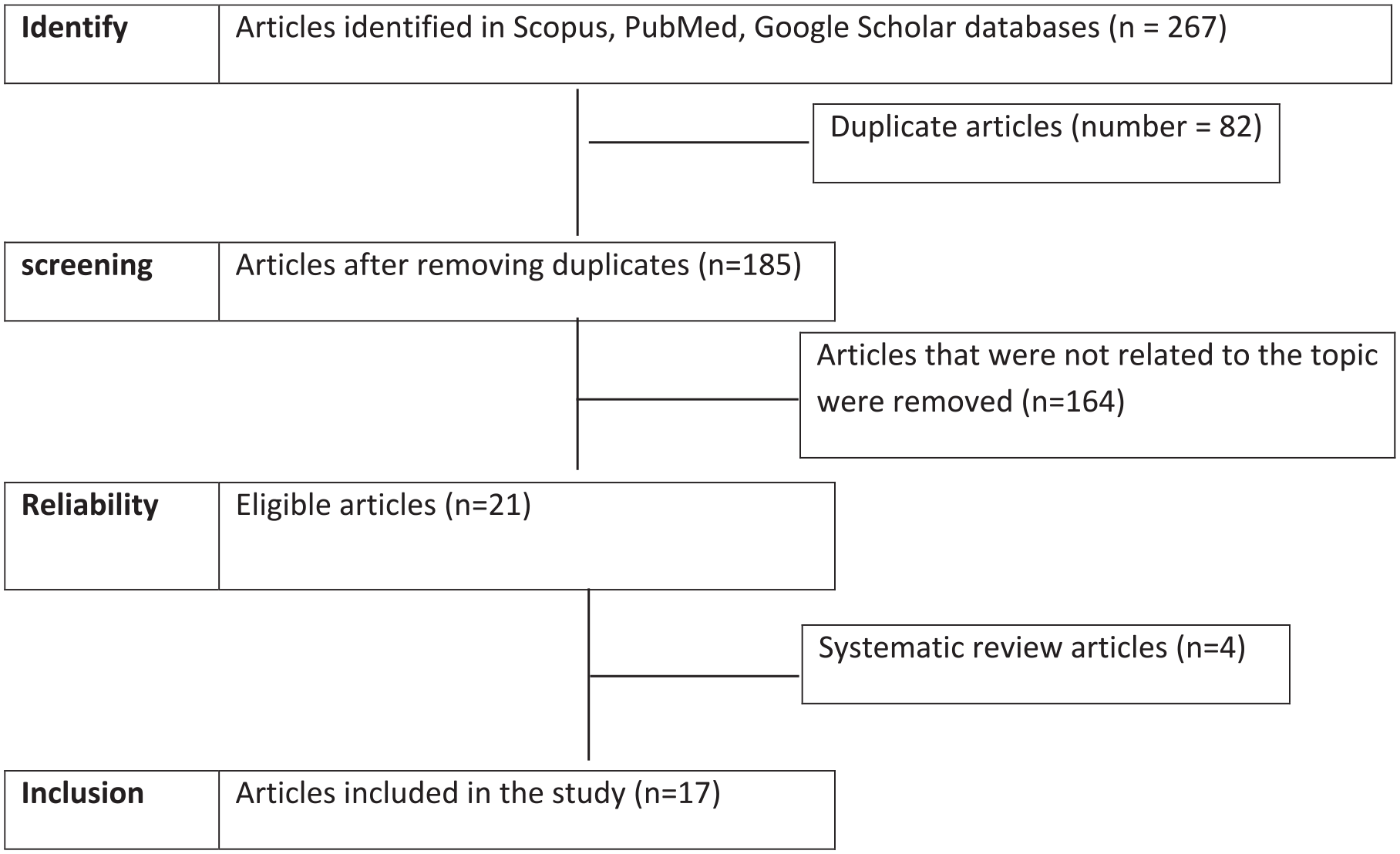
PRISMA Flow Diagram for the systematic and unbiased selection of articles.
Application of Intraoperative X-Ray
A review of the included studies showed that intraoperative X-rays were used in 917 studies. These studies included patients aged 2 to 92 years, and 174 implants were performed in children. In 14 of the patients, the cochlea had an abnormal anatomy. In 6 studies, intraoperative X-rays were part of the routine treatment of patients referred to medical centers. In 19 implants, 7 studies had unsatisfactory results. In 2 studies, the use of X-rays was based on the surgeon’s opinion and was not part of the routine treatment. In cases where the electrode placement was not carefully selected, corrective re-surgery was performed. The surgeon’s decision to perform imaging was seen in 2.0% of cases. In 6 studies, intraoperative imaging was shown to be beneficial, but such evidence was not seen in other studies (Table 1).
Main outcomes of included studies.
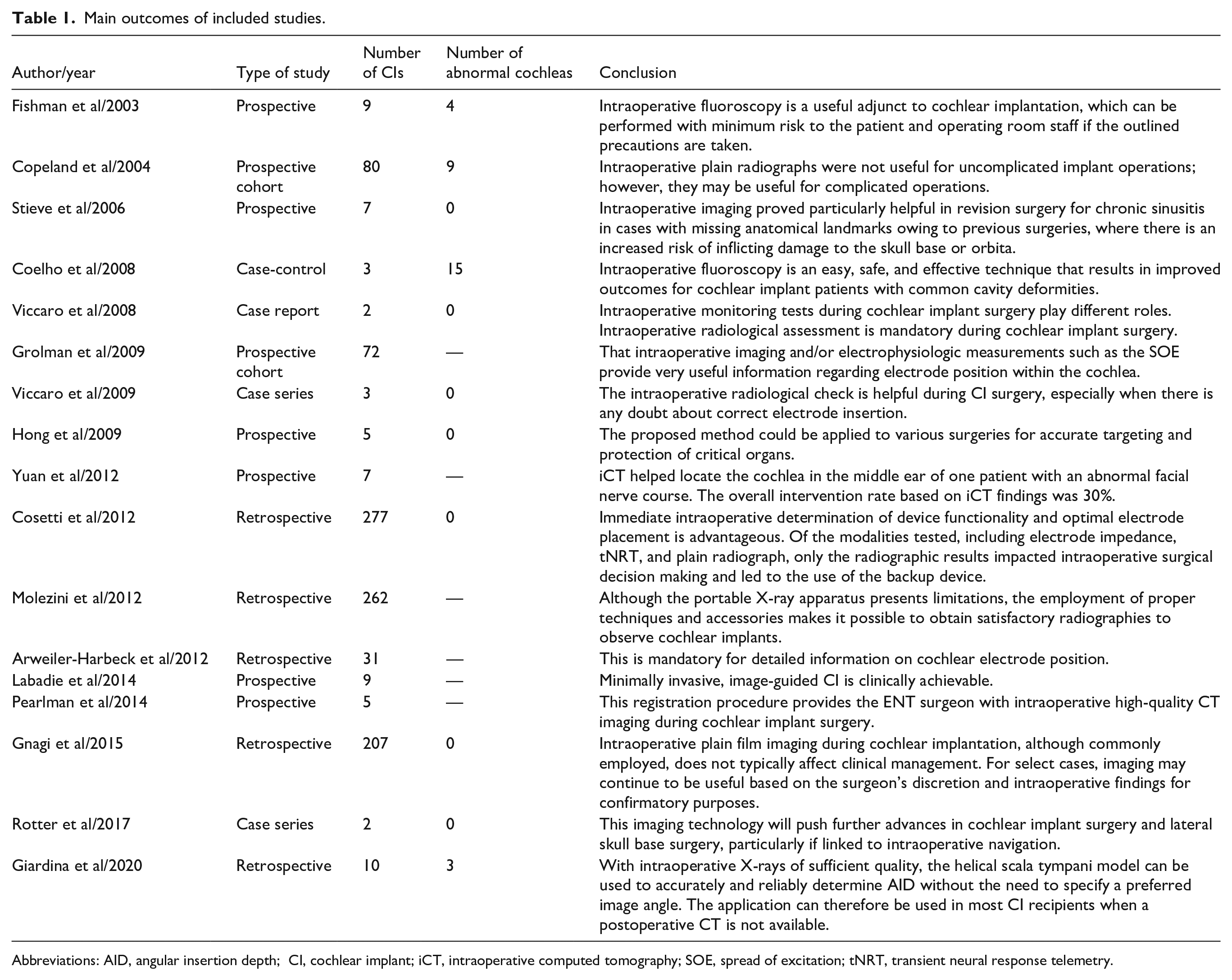
Abbreviations: AID, angular insertion depth; CI, cochlear implant; iCT, intraoperative computed tomography; SOE, spread of excitation; tNRT, transient neural response telemetry.
Use of Intraoperative Computed Tomography
Of the studies reviewed, 69 cochlear implant cases, aged 1 to 73 years, were reported in 7 articles using intraoperative CT. Seventeen of the patients had an abnormal cochlea, and 9 implants were performed in children. In 1 study, CT was performed based on the physician’s decision, and in 5 studies, the use of specific CT was evaluated. In 1 study, CT was performed to evaluate specific cochlear anatomy. Two patients undergoing cochlear implant in 2 studies did not communicate satisfactorily with intraoperative CT, and intraoperative treatment and management policies were changed. Intraoperative management changes with CT were observed in 3.0% of cases. The authors were satisfied with the use of intraoperative CT in cochlear implantation.
Use of Intraoperative Fluoroscopy
Two studies have investigated the importance of intraoperative fluoroscopy in accurately determining the placement of cochlear implants in pediatric and adult patients. Examination of the cochlear anatomy revealed that 22 cases were structurally abnormal and 3 required corrective surgery. In these 2 studies, intraoperative fluoroscopy was used for patients with complex cochlear anatomy. A case-control study by Coelho et al examined the use of fluoroscopy in patients undergoing cochlear implantation with a hole anomaly. The results of this study showed that in patients who had fluoroscopy used in their treatment, all patients were satisfied with their surgical outcome. This study showed that this method can be successful, especially in patients with anomalous anatomy, with Deschat. 11 A study by Fishman et al in 4 patients with an abnormal cochlea requiring cochlear implantation showed that the use of fluoroscopy resulted in accurate electrode placement and patient satisfaction. These researchers found that this method could be particularly useful in cases where the location or outcome of cochlear electrode placement cannot be accurately predicted. 15
Checking the Bias of the Studies
Bias assessment of the studies included in our review showed that the studies were at moderate risk of bias. This finding was due to the non-randomization of the studies, small sample sizes, and lack of comparison groups.
Discussion
We evaluated 17 studies in a systematic review examining the importance of intraoperative imaging in patients with cochlear implants. Our review did not include randomized controlled trials, and although only one was a comparative study, 9 studies were prospective. 12 None of the studies compared imaging modalities. Fifteen studies showed that intraoperative imaging in patients with cochlear implants, particularly those with abnormal cochlear anatomy, can help to accurately determine implant placement.
We categorized the articles by imaging method and their use. The review found that X-rays were the most common imaging method used in a total of 917 cochlear implant cases. In these cases, the use of this method was decided by the surgeon or the treatment policy-makers of the affiliated center. In other cases, the use of imaging was made based on the patient’s condition and the surgeon’s decision. All but two of the reviewed studies found the use of X-rays during cochlear implantation to be beneficial. In these 2 articles, the researchers did not recommend the use of visual aids and did not consider them useful.16,17 Both studies showed that the risk of cataracts can be a complication after radiation exposure. The researchers also noted that multiple CT scans and radiographs can carry serious risks, especially in children.
Five other studies have shown that intraoperative X-rays can be beneficial.9,12,18-20 Incorrect electrode placement occurs in less than 2.2% of cases, which is considered a significant complication because accurate placement is so important in auditory rehabilitation. 21 On the other hand, corrective surgery is associated with increased costs and increased risk of complications. 22 Some studies have shown that reoperation reduces electrode activity and reduces speech perception.23,24 Therefore, the use of X-rays is of great importance, especially in cases with an abnormal cochlea. What is important is to pay attention to tactile feedback during electrode placement. Of course, it should be noted that new electrodes usually do not provide significant tactile feedback. Although there is no requirement to use this method, it can be used at the discretion of the surgeon to improve electrode performance.
Seven studies have examined the efficacy of CT, four of which were conducted in small patient samples. Yuan et al investigated the use of intraoperative CT in patients with abnormal cochlear anatomy. 25 Two studies investigated the role of intraoperative CT in ensuring correct electrode placement.3,26 Their study also examined the performance of imaging without direct exposure of the patient and staff to radiation. Stieve et al also used CT in cochlear implant cases in patients with abnormal cochleas. A study by Arweiler-Harbeck et al showed that flat-panel CT technology, compared with conventional CT, resulted in lower radiation exposure. They also found that this method would not result in misplaced electrodes in cochlear implants. 27 Labadie et al studied the role of intraoperative CT in reducing surgical time and the need for tissue dissection. 28 Other studies have also investigated the importance of intraoperative CT in cochlear implantation.25,26,31 Stieve et al showed that the use of intraoperative CT in patients with an abnormal cochlea is a beneficial and safe treatment option.25,29
The use of CT has its drawbacks. One of the reported complications of this method is cataracts due to radiation exposure. Since patients undergo CT for initial evaluation before surgery, repeated use of CT during surgery can increase the risk of such complications. 31 On the other hand, this method is more expensive for the patient than X-rays.
In addition, the use of this method can increase the time of surgery and general anesthesia and increase the costs imposed on the healthcare system. 32 For this reason, despite the interesting role of CT in cochlear implant surgery, its use is not recommended routinely and cannot be included in the agenda for all patients and all healthcare centers. However, this type of imaging can be used at the discretion and decision of the physician and the patient’s desire, taking into account the conditions of the healthcare center.
Fluoroscopy during cochlear implantation has been investigated in 2 small-sample studies, and the positive role of this imaging modality in patients with abnormal cochlear anatomy has been confirmed.11,15 The study of radiation-related complications in these studies showed that if the beam is focused and away from the lens and used for the shortest possible time, the risk of radiation-related complications can be expected to be reduced. 33
One of the problems with this method is its high cost. Fluoroscopy costs about $1400 for less than an hour. This cost, when combined with the costs of anesthesia, technician, and maintenance of the device, is a significant expense and therefore limits its use. Furthermore, even with the use of protective equipment by the surgeon, there is still a risk of radiation-related complications. 34 Therefore, despite its usefulness in determining the precise location of the electrodes, this method should only be used in special cases and at the discretion of the surgeon. The use of intraoperative fluoroscopy is not recommended for all patients undergoing cochlear implant surgery.35 Further evidence is needed to ensure the safety and efficacy of this procedure.
Overall, the information presented in this systematic review suggests that the use of intraoperative imaging modalities such as X-ray, CT, and fluoroscopy can be beneficial in accurately positioning electrodes in patients undergoing cochlear implant surgery. The appropriate management of the therapeutic line adopted is adjusted based on the patient’s anatomy, available conditions, the financial budget of the treatment center and the patient, and the surgeon’s decision. Despite the promising results obtained, the lack of comparative studies and the absence of specific individual or institutional standard protocols have limited the use of this method. It is still not possible to say with certainty which method is preferable to the other. Further studies are needed to investigate the minimum surgical time, radiation protection methods, selection of the most effective method, and achieving overall patient and medical staff satisfaction.
Conclusion
The use of intraoperative imaging in cochlear implantation can improve the accuracy of electrode placement; however, it is not possible to say with certainty which method is the best choice. The choice of treatment method with intraoperative imaging cannot be generalized to all patients and treatment centers; however, it can be especially beneficial for patients who do not have normal anatomy or whose electrode placement is challenging.
Footnotes
Acknowledgements
The authors wish to express they’re thanks to all who participated in the present research.
Ethical Considerations
This study is a systematic review and did not involve any experiments on human participants or animals performed by any of the authors. Therefore, ethical approval was not required.
Author Contributions
All authors contributed to the conception and design of the study, the acquisition of data, or the analysis and interpretation of the data.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article. No additional datasets were generated or used for this review.