
Abstract
Introduction
Cochlear implantation (CI) is a well-established therapeutic strategy for treating individuals with severe to profound hearing loss. The accurate placement of electrodes is crucial for effective auditory rehabilitation. 1 To ensure correct electrode positioning and minimize surgical complications, intraoperative imaging is often employed. 2
Various imaging modalities are employed during CI procedures, including intraoperative plain portable X-ray, intraoperative computed tomography (CT), and intraoperative fluoroscopy. 3 Of these, intraoperative plain portable X-ray is the most commonly used modality. 3 It offers the benefits of being cost-effective, quick, and generating lower levels of radiation exposure. 2 The incidence of electrode tip fold-over has been reported to be around 2%, 1 and X-ray imaging is effective for its detection. However, it lacks the capability to provide information on intracochlear positioning. 4 Intraoperative CT offers the advantages of high image resolution and a three-dimensional view of the intracochlear structure. 5 This modality enables the intraoperative identification of array misplacements 5 into the semicircular canal or vestibule, particularly in patients with abnormal anatomical structures.6,7 Nonetheless, it exposes patients to higher levels of radiation, with a dose of 91 mGy for high-resolution CT and 12 mGy for cone-beam CT. 5 While the recommended dose threshold for cataract development used to be 0.5 Gy, current recommendations, based on epidemiological evidence, suggest lowering this dose further. 8 Intraoperative fluoroscopy, similar to intraoperative CT, is useful in cases involving complex anatomical structures.9,10 However, it presents some limitations, including higher patient radiation doses ranging from 4.6 to 15.8 mSv—compared to 0.02 to 0.09 mSv for intraoperative portable X-ray—and the risk of radiation scatter affecting the surgeon. 11
Throughout this article, the term “handheld digital X-ray” is used. In this context, “handheld” refers to a battery-powered device designed for handheld operation by the user during image exposure. 12 The first handheld X-ray device originated in the United States in 1993 for military applications, and since then, nearly 95% of such devices have been utilized for dental radiography. 13 These handheld devices facilitate image capture, particularly when patients are sedated or anesthetized in the operating room—most notably during intraoperative implant placement. 14 The term “digital” in handheld digital X-ray signifies digital radiography. Over the past 2 decades, flat panel detectors (FPD) have largely replaced screen-film detectors. Integrated post-processing functions and image acquisition technologies have enabled the production of high-quality images while minimizing radiation exposure. 15 Currently, the application of handheld X-rays has expanded to include chest radiography, in addition to dental uses. 16 The potential for deploying these devices in environments where traditional stationary X-ray equipment is impractical is under active discussion. 15
To date, a range of imaging modalities has been employed to verify accurate electrode placement during cochlear implant surgery. However, handheld digital X-rays have not been among them. The objective of this report is to introduce a specialized intraoperative portable digital X-ray device as a viable imaging modality for cochlear implant surgeries and to share the findings associated with its use.
Materials and Methods
Patients
This retrospective study involved 11 patients, corresponding to 12 ears, who underwent CI between December 2021 and January 2023. A single surgeon performed all surgeries, using the implant models CI632 and CI612 (Cochlear, Sydney, Australia), as well as Flex26 (MED-EL, Innsbruck, Austria). Following the CI procedures, intraoperative imaging was carried out with the MINE ALNU® (OTOM, Gwangju, South Korea) handheld X-ray device. This device comprises 3 main components: an X-ray generator, a 17 × 17-in FPD and laptop with a built-in router for receiving images from the detector [Figure 1]. The study was sanctioned by the Institutional Review Board of Chonnam National University Hospital (IRB No. CNUH-2023-155).
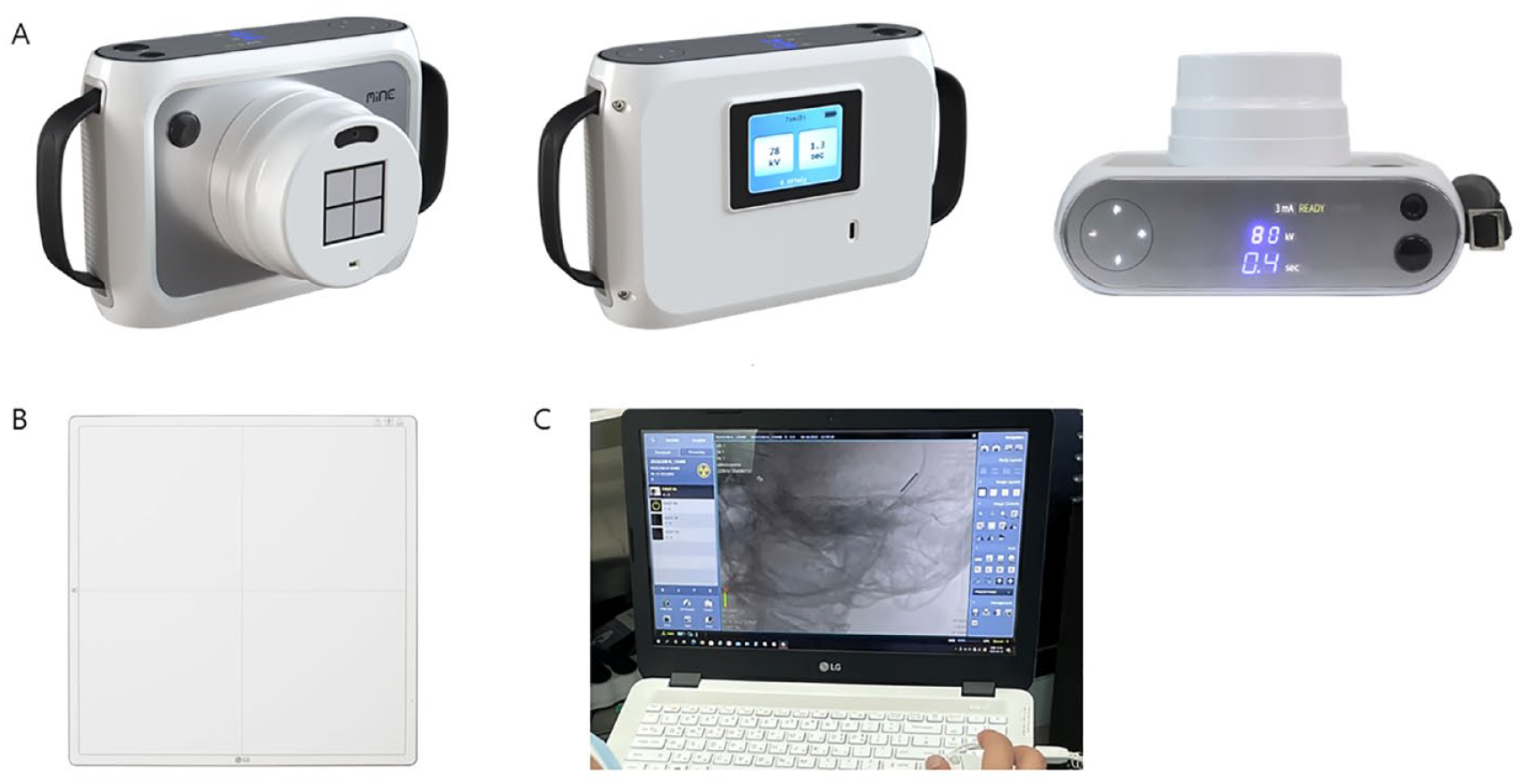
Components of the handheld digital X-ray. (A) X-ray generator. (B) 17 × 17-in. flat panel detector. (C) laptop with a built-in router for receiving image transfer from the detector.
Imaging Technique
The positioning of the inserted electrodes was verified using 2 specific radiographic views: the transorbital anterior–posterior (AP) view 17 and the anti-Stenver’s view (45° side view) [Figure 2(A) and (B)]. Both views were aligned with the central beam oriented perpendicular to the film. 18 These techniques have been previously established as offering optimal orientation for visualizing the cochlea, either intraoperatively or postoperatively.2,17-21 Adjustments were made to both methodologies to enable X-ray acquisition while the patient remained in a supine position on the surgical table. During this process, the FPD was positioned under the bed sheet behind the patient’s head. The X-ray generator was situated at a distance of 40 cm from the patient,19,22 a measurement verified by an integrated sensor and displayed in real-time. Acquired images were immediately available for review on a laptop [Figure 1(C)]. The study employed a handheld digital X-ray exposure set at 80 kVp and a photocurrent of 3 mA, with exposure times ranging from 0.6 to 1.3 seconds (optimal duration: 1.0 s). The approximate radiation dose ranged from 0.001 to 0.002 mSv. For all patients, both intraoperative handheld digital X-rays and postoperative plain X-rays were performed as part of standard procedures. Additionally, intraoperative C-arm imaging was selectively employed, specifically for cases involving the slim modiolar electrode (CI 632), which had a higher likelihood of tip fold-over. 23 In these instances, the C-arm was used in radiography mode (single shot), rather than fluoroscopy mode. Postoperative plain X-rays were captured using the transorbital AP view.
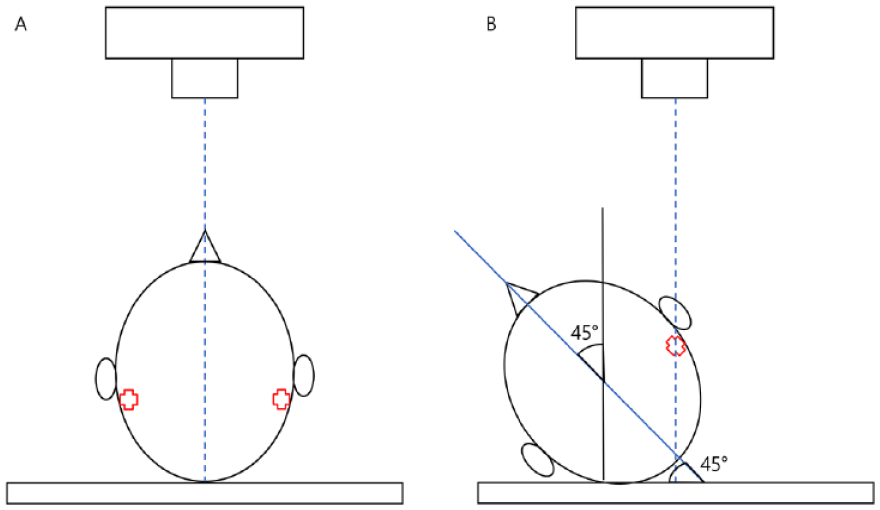
Diagrams illustrating handheld digital X-ray imaging orientation. (A) Transorbital anterior–posterior view. (B) Anti-Stenver’s view (45° side oblique view).
Electrically Evoked Compound Action Potential (ECAP)
ECAP serves as a measure of the auditory nerve’s neural responsiveness. 24 It is instrumental in intraoperative assessments for device functionality and optimal electrode positioning. 25 Various manufacturers provide software for intraoperative ECAP measurement, including neural response telemetry (NRT) from Cochlear (Sydney, Australia) and auditory nerve response telemetry (ART) from MED-EL (Innsbruck, Austria). Measurements of ECAP were conducted under sterile conditions, carried out during the surgical incision closure subsequent to electrode insertion into the cochlea. For this study, ECAP thresholds were quantified in all channels for each subject using either AutoNRT or AutoART.26,27 Specifically, AutoNRT was employed for CI632 and CI612, while AutoART was utilized for Flex26.
Results
The evaluation of intracochlear electrode array placement was conducted in 11 cochlear implant recipients using intraoperative handheld digital X-ray. In total, 12 surgeries were conducted: 10 were unilateral implants and one was bilateral. Among the patients, 9 received CI632 implants, 2 were implanted with Flex 26, and 1 received a CI612 implant. Imaging analysis revealed malpositioned electrode array in one patient implanted with a CI632. Consequently, the initial CI632 was replaced with a CI612. ECAP thresholds were evaluated for all patients, and an absence of response was observed in channel 9 for one individual. Detailed patient characteristics can be found in Table 1.
Patient Characteristics and Intraoperative Handheld Digital X-ray Imaging Results in Cochlear Implant Procedures.
Abbreviations: ECAP, Electrically evoked compound action.
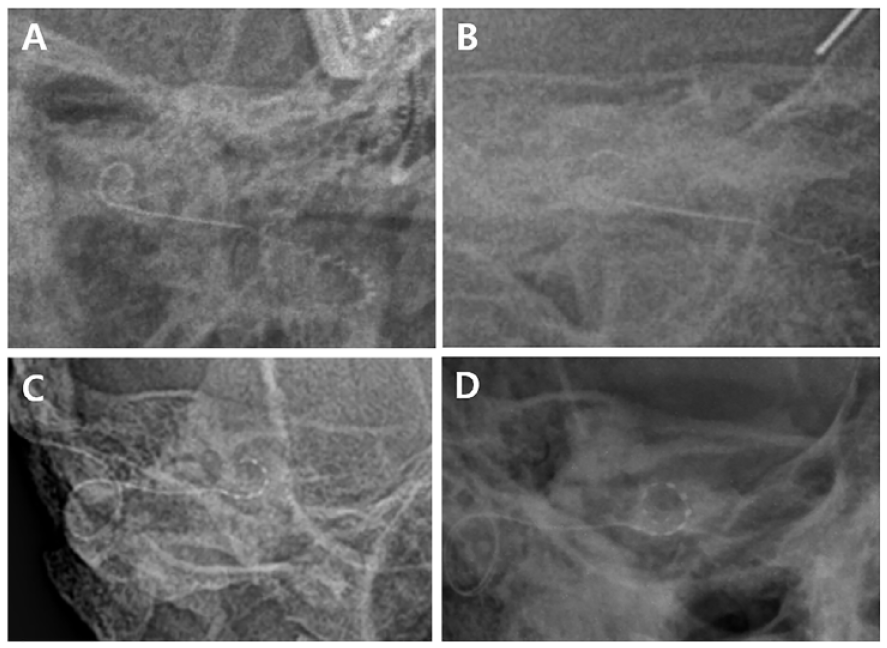
Our initial observations included intraoperative handheld digital X-ray and postoperative plain X-ray images of a 2-year-old child [Figure 3(A) and (B)] and an adult [Figure 3(C) and (D)], both with properly inserted CI632 electrodes. Although the image quality may be suboptimal compared to postoperative radiographs, it offers sufficient resolution to confirm appropriate electrode array insertion during surgery. Additionally, we assessed the intraoperative transorbital AP and oblique images of a patient with a CI632 implant [Figure 4(A) and (B)]. The electrode array for the Flex 26 implant was clearly visualized using the intraoperative handheld digital X-ray [Figure 4(C) and (D)]. A malpositioned electrode array was identified both in handheld digital X-ray and C-arm images [Figure 5]. A malpositioned electrode array was identified in C-arm images [Figure 5(C)]. While the image quality of the handheld digital X-ray was comparatively lower than that of C-arm X-ray images [Figure 5(A)], making it challenging to confirm malpositioned electrode array definitively, but we could recognize that the electrode array was not normal.
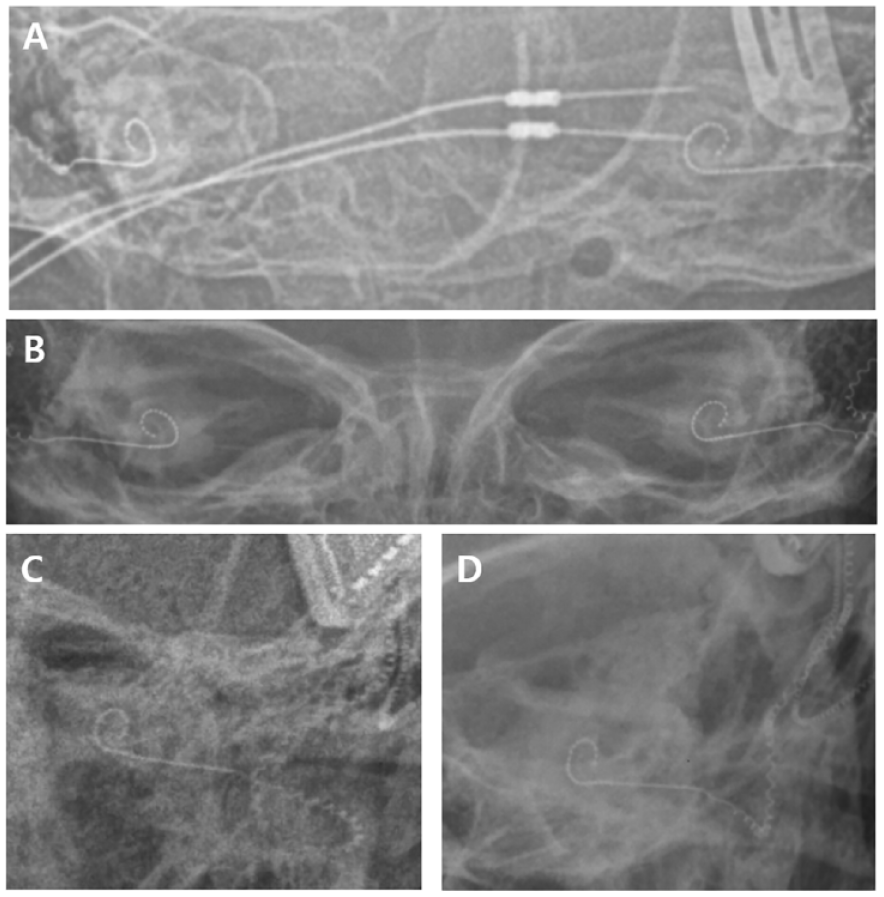
Comparison of intraoperative and postoperative transorbital anterior–posterior (AP) images following CI632 electrode implantation. (A) Intraoperative transorbital AP image of a 2-year-old infant captured using handheld digital X-ray postimplantation. (B) Postoperative transorbital X-ray image of the same infant taken outside the operating room. (C) Intraoperative transorbital AP image postimplantation in an adult captured using handheld digital X-ray. (D) Postoperative transorbital X-ray image of the same adult taken outside the operating room.
Comparison of intraoperative transorbital anterior–posterior (AP) and oblique images captured using handheld digital X-ray. (A) Intraoperative transorbital AP image following CI632 implantation. (B) Intraoperative oblique image post-CI632 implantation. (C) Intraoperative transorbital AP image following Medel Flex 26 implantation. (D) Intraoperative oblique image post-Medel Flex 26 implantation.
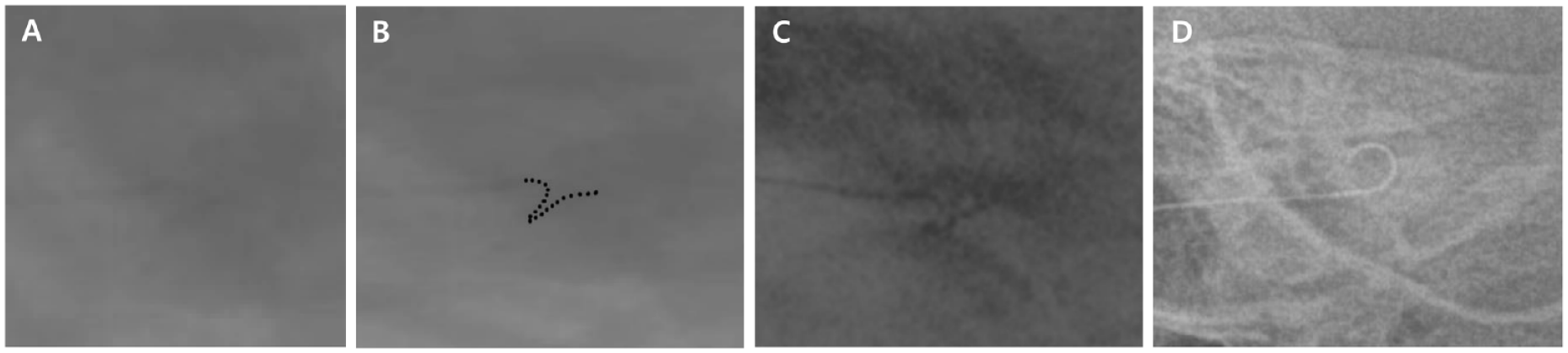
Malpositioned electrode array image in a 77-year-old female patient post-CI632 implantation. (A) Intraoperative oblique image captured using handheld digital X-ray. (B) Image with highlighted electrodes for enhanced clarity. (C) Image captured using intraoperative C-arm X-ray, (D) Intraoperative oblique image captured using handheld digital X-ray after changing CI 612 implantation.
Discussion
Cochlear implantation is a pivotal surgical intervention for individuals living with hearing loss, and the procedure’s success is largely contingent upon the accurate placement of the electrode array. 28 In certain cases, suboptimal positioning may necessitate revision surgery.1,19 To address this issue, intraoperative imaging techniques have been developed.
In our study, we employed intraoperative handheld X-ray examinations on a sample of 11 patients, accounting for a total of 12 ears. The types of electrodes utilized included CI632 in 9 instances, CI612 in 1, and Flex26 in 2. To confirm accurate electrode placement, we employed handheld portable X-ray and intraoperative C-arm X-ray during the procedure. Postoperatively, ECAP measurements and plain X-ray were utilized for verification. We identified a malpositioned electrode array in one instance, which was rectified by replacing the cochlear implant intraoperatively. In the remaining 11 cases, the placement of the electrodes was verified to be correct.
Historically, portable plain X-ray and fluoroscopy have been the modalities of choice for intraoperative imaging in cochlear implant surgeries.3,10,29 However, these conventional systems have several limitations due to their bulky size. In facilities with restricted operating room space, such equipment is generally stored outside the operating area and transported in as needed. This necessitates a considerable rearrangement of the surgical setup, including the relocation of microscopy and instrument trays. Additionally, aligning these large systems consumes valuable time. Conversely, handheld portable X-ray devices offer a more practical solution. Weighing less than 3 kg, they can be conveniently positioned within the operating room, thereby minimizing the need to rearrange other surgical equipment and reducing setup time. Additionally, the operator can immediately review the imaging results on a connected laptop.
The intraoperative handheld digital X-ray technology offers several advantages over traditional imaging modalities (Table 2). Specifically, the radiation dose is substantially lower compared to that of C-arm and portable plain X-ray. In the current study using the MINE ALNU®, the measured radiation dose ranged from 0.001 to 0.002 mSv. This is considerably lower than the effective doses reported for skull X-ray examinations (0.02-0.09 mSv) and standard C-arm fluoroscopy (4.6-15.8 mSv).3,30 Pearce et al have indicated that cumulative radiation doses exceeding 50-60 mSv in pediatric patients could triple the risk of leukemia and brain cancer. 31 The principle of As Low As Reasonably Achievable (ALARA) underscores the importance of minimizing radiation exposure while maintaining diagnostic image quality. 32 In accordance with the ALARA principle, handheld digital X-ray emerges as a preferable choice for effectively reducing radiation exposure.
Comparison of Handheld X-ray, Portable X-ray, and C-arm Based on Radiation, Equipment Size, and Cost.
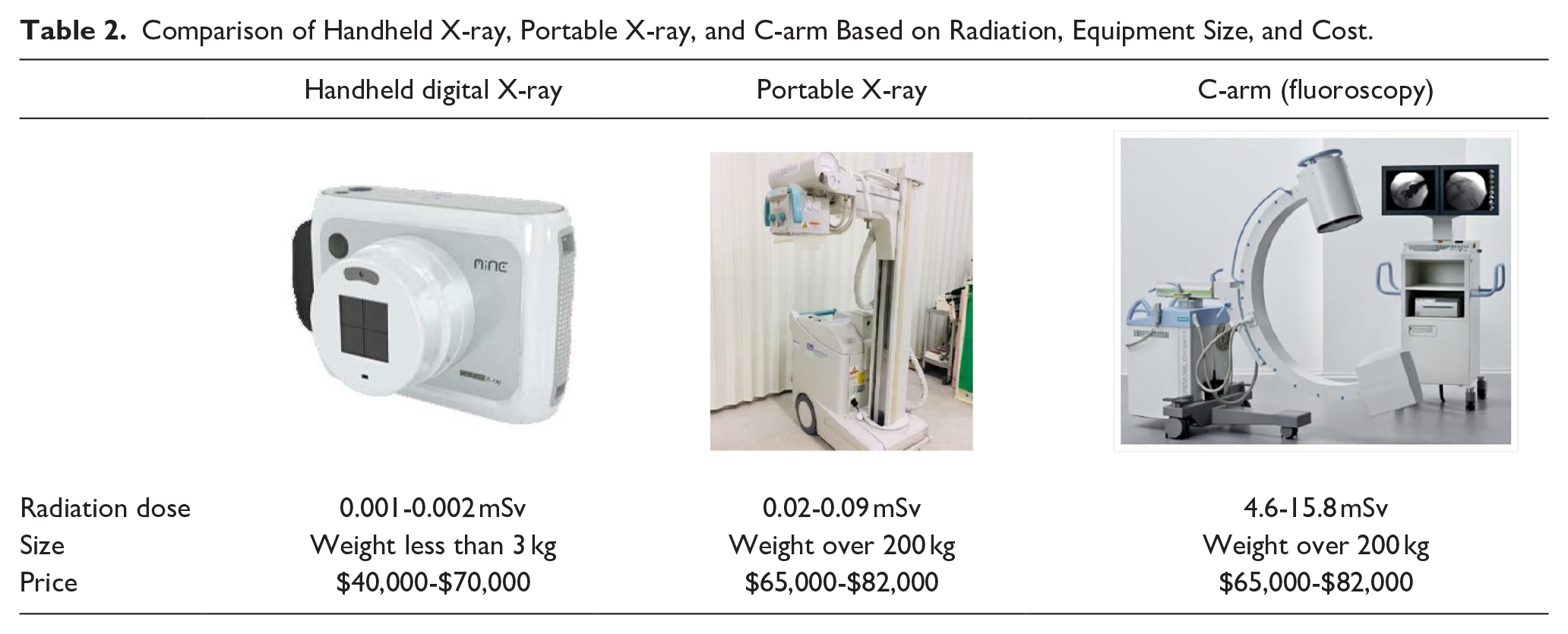
Cost-effectiveness represents another significant advantage of this technology. FDA- or CE-approved portable X-ray machines typically fall within a price range of US$65,000 to US$82,000. 33 Similarly, the cost of C-arm machines aligns with this range, averaging between US$65,000 and US$82,000. 34 In contrast, handheld digital X-ray machines are more economically priced, ranging from $40,000 to $70,000. 35 Therefore, they present a more affordable alternative to traditional portable and C-arm X-ray devices.
Nevertheless, instances in which image quality is compromised can be considered as limitation. Further investigation is warranted to explore the optimal exposure durations and imaging conditions to enhance image visualization. In our study, with the exception of malpositioned electrode array case, the image quality did not show a significant difference when compared to C-arm X-rays or postoperative plain X-rays for verifying accurate electrode placement. The reduced image quality in instances of malpositioned electrode arrays could be attributed to difficulties in managing blur caused by motion and achieving precise angle alignment during the assessment. Additional data collection in future studies is anticipated to provide a more exhaustive evaluation and potentially enhance the utilization of the MINE ALNU® intraoperative handheld digital X-ray, offering enhanced capabilities in cochlear implant surgery.
Conclusion
The MINE ALNU® intraoperative handheld digital X-ray offers a safe, efficient, straightforward, cost-effective, and reliable method for the immediate assessment of cochlear implant electrode array positioning. It has the potential to supersede other intraoperative imaging modalities in determining electrode placement within the operating room.
Footnotes
Acknowledgements
We extend our gratitude to Wordvice for their assistance with English language editing.
Authors’ Note
There are no prior publications or submissions with any overlapping information, including studies and patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (HR20C0021), and Chonnam National University Hospital Biomedical Research Institute grant (No. BCRI22084).
Ethical Approval
The research project was approved by the verification service and the ethics committee of Chonnam National University Hospital (IRB No. CNUH-2023-155).