
Abstract
Cholesteatomas can grow aggressively within the temporal bone due to the accumulation of keratin. If not treated, they can destroy surrounding structures and, therefore, cause many comorbidities. Surgery is the mainstay of treatment. We present a case of massive cholesteatoma involving the facial nerve (FN) with extension into the neck around the FN. The patient underwent a planned multidisciplinary resection of the cholesteatoma without postoperative morbidity.
Introduction
Cholesteatomas are the pathological growth of the keratinizing squamous epithelium in the temporal bone, characterized by accumulation of keratin debris. 1 In the absence of appropriate interventions, its progression beyond the boundaries of the mastoid and temporal bone may lead to intracranial complications. 2 In addition, cholesteatomas can expand and involve the facial nerve (FN). 3 Facial weakness from cholesteatoma can be sudden, necessitating urgent intervention. We present a complicated case of massive cholesteatoma with dehiscence of the middle and posterior fossa dura and involving the FN with extension into the neck around the FN.
Case Report
A 51-year-old man came to our tertiary care neurotology clinic after a recent surgical procedure at an outside facility. Before coming to our clinic, he had undergone an attempted resection in November 2019 at an outside hospital complicated by a canal mastoid fistula. The initial operative findings included a pars flaccida cholesteatoma with dehiscence of the posterior and middle cranial fossa (Figure 1A and B). The distal mastoid FN was exposed 360° and covered with cholesteatoma (Figure 1C and D). There were 2 cholesteatoma sacs in the medial area of the temporal muscle.
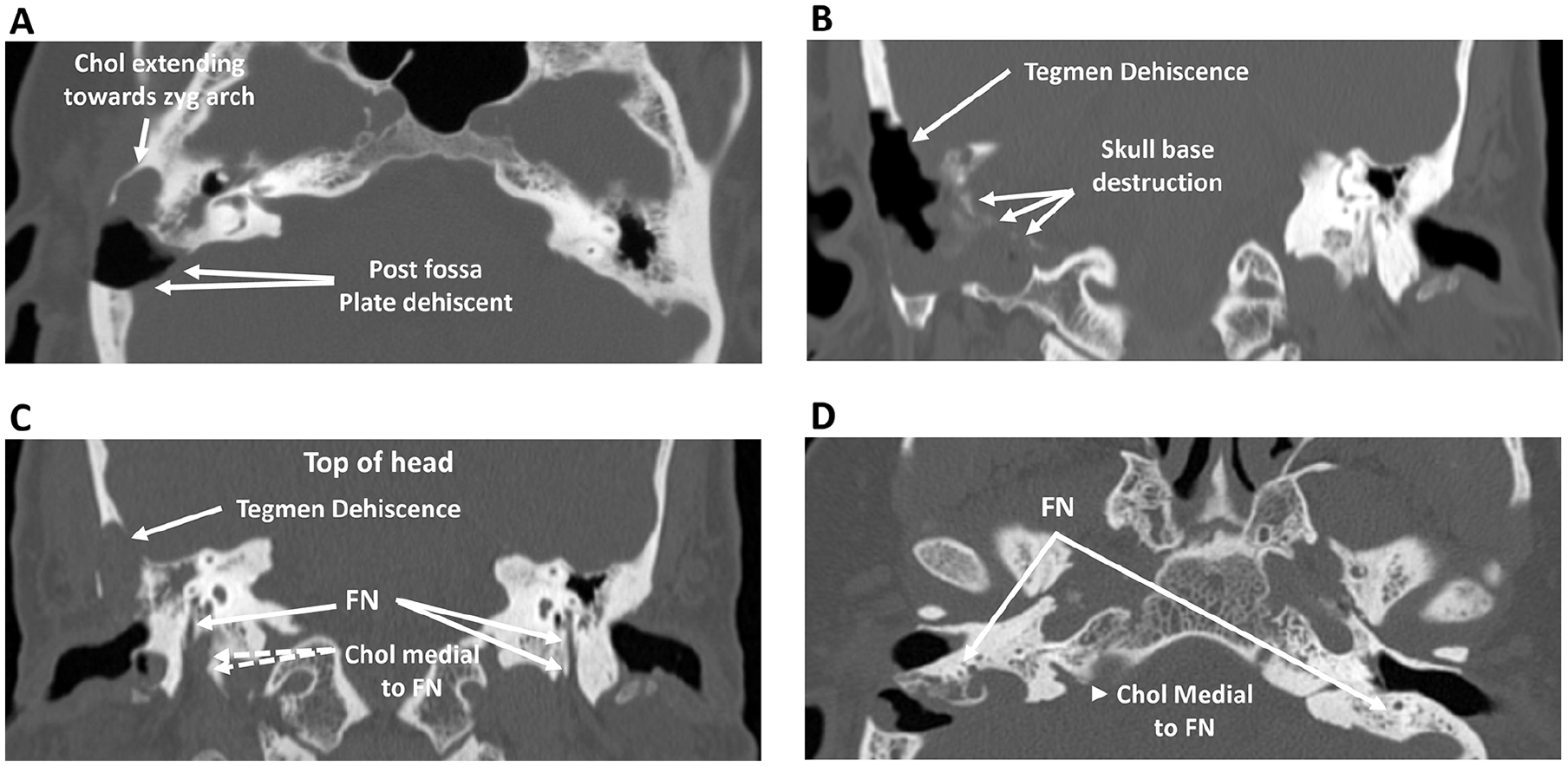
Preoperative CT scan of the cholesteatoma with posterior and middle fossa dehiscence with the involvement of FN. (A) Axial CT of right ear cholesteatoma (chol) with posterior fossa dehiscence and extending toward the zygomatic (zyg) arch. (B) Coronal CT of the right temporal bone demonstrating middle fossa dehiscence and skull base destruction. (C) Coronal CT of right temporal bone with tegmen dehiscence and cholesteatoma medial to FN. (D) Axial CT of temporal bone indicating cholesteatoma medial to FN. CT, computed tomography; FN, facial nerve.
Nine months after the initial surgery, the patient underwent a second surgery. Findings included a narrow cholesteatoma sac that extended deeply towards the neck through the stylomastoid foramen (Figure 2A) and was found to be adherent to the dura (Figure 2B). Due to the dural and neck involvement, the surgery was aborted. The patient was told that cholesteatoma resection would require FN and dural resection with graft. Subsequently, the patient presented to our center, and surgery was performed in April 2021. During surgery, the cholesteatoma was separated from the middle and posterior fossa dura, and no dural resection was needed. There was a second site of cholesteatoma in the mastoid antrum. The distal mastoid FN was completely surrounded by cholesteatoma (360°), tracking into the neck. The mastoid tip was removed to open the stylomastoid foramen, the neck was explored by the head and neck team, and the cholesteatoma was removed from the neck. After surgery, the patient was scheduled for an annual magnetic resonance evaluation to facilitate early identification of recurrence and prompt initiation of appropriate treatment. The 1 year postoperative magnetic resonance imaging (MRI) of the patient did not show evidence of recurrence (Figure 2C). The patient has not followed up with subsequent MRIs.
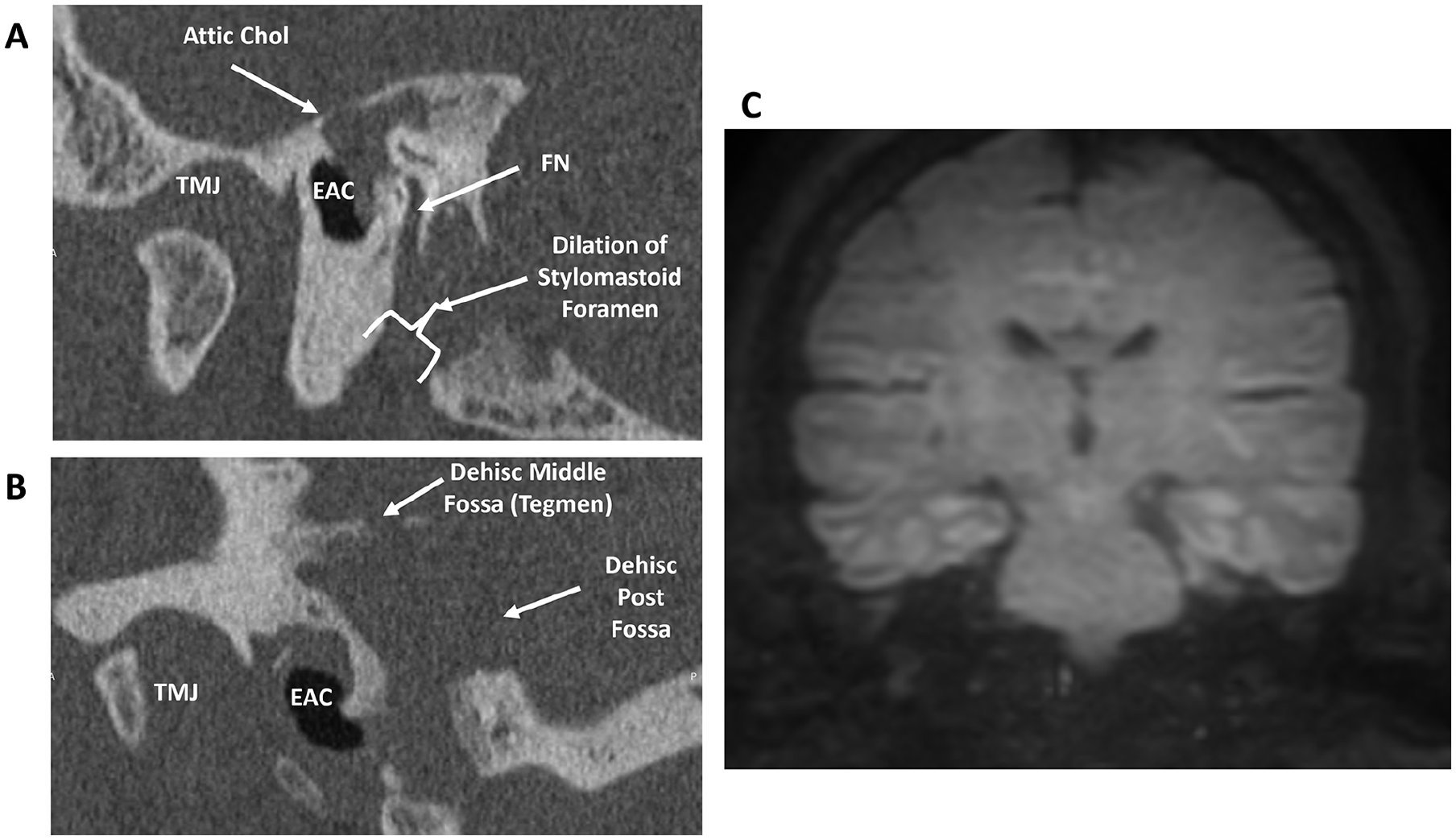
Preoperative and postoperative imaging of cholesteatoma. (A) Coronal CT of cholesteatoma with neck extension. (B) Coronal CT of cholesteatoma with dura adhesion. (C) Non-echoplanar diffusion-weighted image MRI (HASTE sequence) of the patient at 1 year postoperatively, showing no evidence of cholesteatoma recurrence. CT, computed tomography; MRI, magnetic resonance imaging.
Discussion
This case emphasizes the importance of carefully and thoroughly assessing the possible extension of large cholesteatomas during surgery. Extension of the cholesteatoma to the neck is rare. Previous studies have suggested 2 main explanations for the formation of cholesteatoma in the neck: iatrogenic implantation and direct spread through the mastoid tip. 4 Evidence from the iatrogenic implantation during radical mastoidectomy indicates that masses developed several years after surgery, although the mastoid cavity and cortex remained free of cholesteatoma. 5 Iatrogenic implantation of cholesteatoma is unlikely in our patient, as the patient underwent their last surgery only a year before the current. Furthermore, the presence of cholesteatoma in the mastoid and surrounding the FN, as well as erosion of the mastoid tip, suggests that the cholesteatoma extended from the mastoid into the neck.
Direct extension from the mastoid generally follows a predictable path, often characterized by the erosion of cells at the tip of the mastoid that allows the invasion of the cholesteatoma into the neck. The complex nature of these cases requires careful consideration of imaging with computed tomography (CT) and MRI, and multidisciplinary surgical planning. 6 CT scan of the temporal bone can demonstrate bony anatomy and destruction, and MRI can identify the areas of cholesteatoma on diffusion weighted imaging.2,7,8 The surgical approach must include both mastoid and neck disease resection. In our institution, the head and neck team explored the neck and cleared the neck after the neurotology team resected the mastoid and skull base portions of the disease, as well as removed the mastoid tip. In some cases, the sternocleidomastoid muscle may require partial excision to allow thorough disease clearance. 9
Dural adherence is a serious potential complication in cholesteatoma surgery, making it essential for surgeons to understand its management and consequences. 10 Resection of the dura is rarely required, except in cases where biomaterials or dural grafts have been placed over the cholesteatoma during a previous resection, leading to entrapment of the cholesteatoma tissue between the layers of the dura. Bony dehiscences created during surgery can pose a risk for complications if left untreated. 11 Using bone pate and cartilage to close these bony defects provides a strong barrier, ensuring that the defect is securely sealed and prevents dural adhesion if a recurrence occurs. Our preference is to first place the bone pate on the dural dehiscence and then cover it with cartilage, as cartilage can adhere to the dura, and separation of it in a potential subsequent surgery may lead to a dural tear. Although residual cholesteatoma is a major factor contributing to the high recurrence rate after initial surgery, regular follow-up with MRI is essential to monitor for any signs of recurrence.12,13 Annual imaging tests, particularly MRI, be effective in early detection of recurrences, which allows for timely intervention when necessary. 4 Managing massively extended cholesteatoma presents a complex clinical challenge that requires careful consideration of various factors. Using meticulous planning and surgical techniques, resection of the cholesteatoma can be achieved with minimal morbidity.
Conclusions
This case report highlights the challenges of treating massive cholesteatomas. Careful surgical planning, a team approach, and effective reconstruction methods and materials were key to a successful outcome. In addition, regular follow-up imaging is essential for early detection of recurrence and for reducing complications.
Footnotes
Ethical Considerations
Ethical approval was not required for this case report. The patient was treated as part of routine clinical care and no experimental interventions were performed.
Consent to Participate
Written informed consent to participate in this case report was obtained from the patient.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Djalilian has equity in NeuroMedCare LLC, Elinava Technologies, and Cactus Medical LLC. The other author(s) declared no potential conflicts of interest.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon request. The data are not publicly available due to privacy and ethical restrictions, as they contain protected health information (PHI) from UCI Health. Sharing the data could potentially violate patient privacy and HIPAA regulations.