
Abstract
Objective:
To determine whether the presence of vocal cord paralysis (VCP) has an impact on overall survival (OS) and quality of life in patients diagnosed with extralaryngeal malignancies.
Methods:
This was a retrospective chart review of patients at a quaternary medical center from 2007 to 2022. Information on demographics, cancer diagnosis, treatment, and intervention for VCP was collected. Patients were identified using International Classification of Diseases (ICD)-9 and ICD-10 codes for various malignancies and VCP and cross-referenced. Patients with both VCP and extralaryngeal malignancy were included, while those without malignancy, with laryngeal cancer, VCP unrelated to cancer, or without laryngoscopy-confirmed VCP were excluded. No validated instruments to measure quality of life were utilized.
Results:
A total of 346 patients with VCP related to 52 distinct, extralaryngeal malignancies were identified. Mean OS was 97.35 months. Mean OS for those diagnosed with early (stage 1 or 2) cancers was 101.48 months and 79.88 months for late (stage 3 or 4) cancers (P = <.0001). Many of our patients (56.6%) did not receive VCP treatment.
Conclusion:
Treatment for cancer patients with VCP poses a unique challenge with a multitude of factors affecting management. However, given that patients survive months after VCP diagnosis, they should be offered treatments that carry low morbidity and increase their quality of life.
Introduction
Vocal cord paralysis (VCP) can significantly impact quality of life, resulting in dysphonia, aspiration, poor airway protection, and decreased exercise tolerance.1,2 It can be caused by a variety of pathologies, with malignancy accounting for around 30% of all causes.3-5 In the oncologic population, the morbidity from VCP can be especially detrimental, compromising the ability to eat, limiting social interactions, and increasing the risk of aspiration-related complications. However, many VCP-related symptoms are not captured by standard quality-of-life measures in cancer patients.6-8
Despite its impact, treatment for VCP in cancer patients frequently faces substantial barriers. Often, these patients are actively undergoing oncologic therapy, and both physicians and patients may be reluctant to pursue interventions that could pause or delay cancer treatment. In the later stages of disease, patients are frequently deconditioned, and management may shift toward palliative care, limiting candidacy for additional procedures.
In addition, treatment of VCP in this population has received little attention in recent literature. Current publications have small sample sizes, limited follow-up, and typically focus on specific procedures.9-12 We hypothesize that due to advancements in cancer treatment, these patients are living longer 13,14 and therefore are more likely to benefit from durable VCP interventions that address laryngeal dysfunction and improve quality of life.
Materials and Methods
This retrospective study was approved by the Institutional Review Board at Loyola University Medical Center (LUMC). We reviewed the medical records of all patients with both a diagnosis of VCP and any extralaryngeal malignancy treated at LUMC between 2007 and 2022. Patients were identified using International Classification of Diseases (ICD)-9 and ICD-10 codes for malignancies and cross-referenced with codes for VCP.
Chart review was performed by 2 independent reviewers (VD and SC), with discrepancies resolved collaboratively. Data were collected from the time of cancer diagnosis until either the date of last documented follow-up with any healthcare provider or death. VCP was defined to include both paralysis and paresis, as the retrospective nature of the study made it difficult to distinguish between the 2 in the medical record.
Exclusion criteria were patients without a confirmed malignancy, those with laryngeal cancer, VCP unrelated to cancer, and those without VCP or documented laryngoscopy confirming VCP. Although laryngeal cancer was excluded, other head and neck cancers were included.
Results
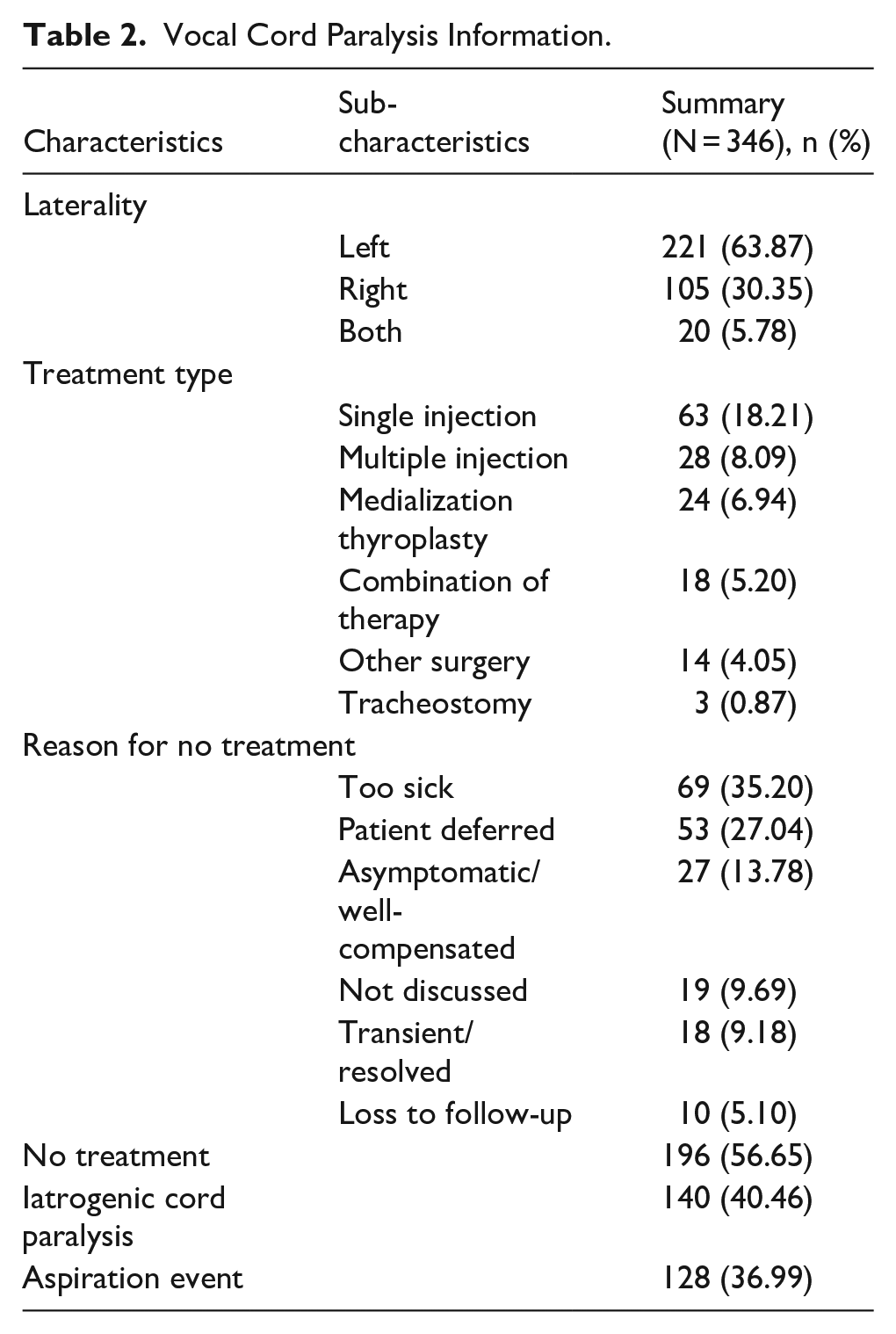
We identified 346 patients who had VCP related to 52 distinct malignancies (Supplemental Table 1). The most common cancer types in our patient population were lung (107/346, 30.9%), thyroid (105/346, 30.3%), and esophageal (42/346, 12.1%; Table 1). Medical comorbidities were assessed using the Charlson comorbidity index. 15 VCP predominantly affected the left vocal cord (221/346, 63.9%), and bilateral dysfunction was noted in 20 patients (5.8%). Iatrogenic VCP cases were included if the paralysis resulted from surgical sacrifice of the recurrent laryngeal nerve during oncologic resection, as confirmed in the operative report.
Patient Demographics.
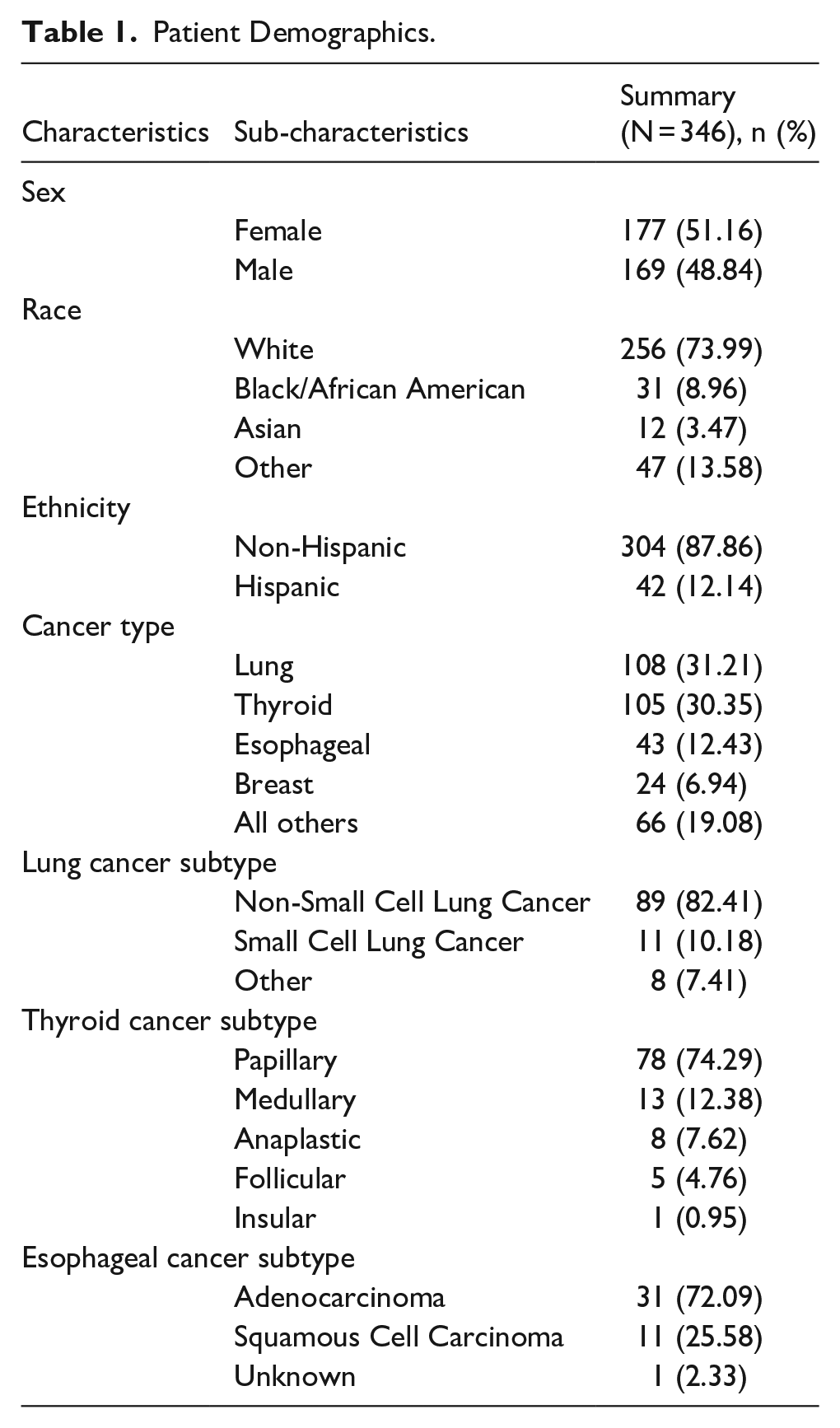
The majority of patients did not receive any intervention for their VCP (196/346, 56.6%). The most common reasons for deferral were poor interventional candidacy (69/196, 35.2%) and patient preference (53/196, 27.0%). Of the 150 patients who did receive treatment, the most common intervention was a single injection laryngoplasty (63/150, 18.2%; Table 2).
Vocal Cord Paralysis Information.
Data on cancer stage were available for 250 patients diagnosed with lung, thyroid, esophageal, and breast cancers. All stages were updated to reflect the most recent American Joint Commission on Cancer (AJCC) Cancer Staging Manual, Eighth Edition (2017), per National Cancer Center Network guidelines. Patients were then divided into quartiles according to AJCC prognostic groups (stage I-IV) and grouped into early-stage (stage I-II; n = 99) and late-stage (stage III-IV; n = 151) categories. At the time of chart review, 65.9% (n = 228) of patients were deceased.
Survival data were obtained looking at the overall survival (OS) from the time of VCP diagnosis. The mean OS for the entire cohort was 97.35 months (Figure 1). Those with early-stage cancers had a mean OS of 101.48 months, compared to 79.88 months in late-stage disease (P < .0001; Figure 2). Given that different types of cancers have varying prognoses, we then proceeded with subgroup analysis for the 3 most commonly identified cancers in our study group (lung, thyroid, and esophageal; Figures 3–5). Lung cancer was associated with the lowest OS, with a 44% 1-year survival rate following VCP diagnosis. Esophageal cancer had a moderate prognosis at 61%, while thyroid cancer had the most favorable outcome, with 91% of patients surviving at 1 year.
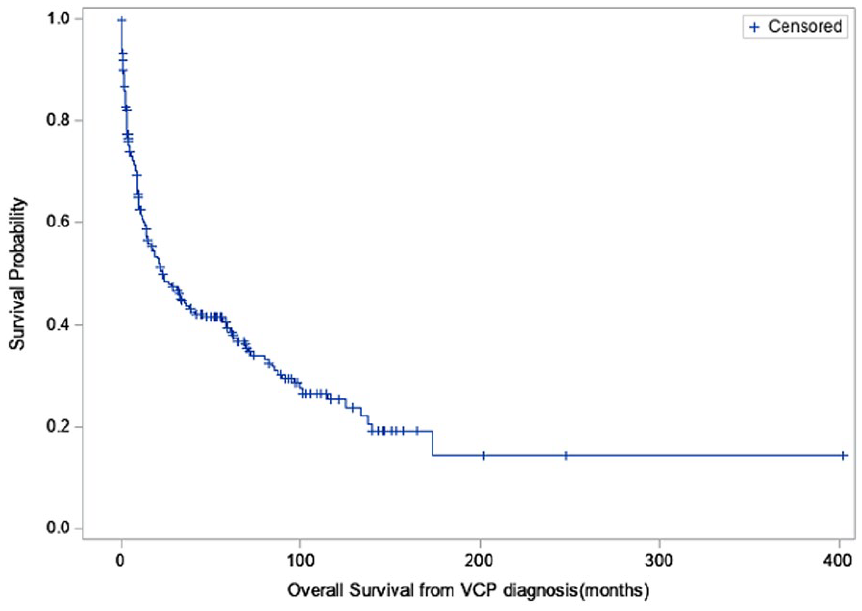
Overall survival from the time of VCP diagnosis. VCP, vocal cord paralysis.
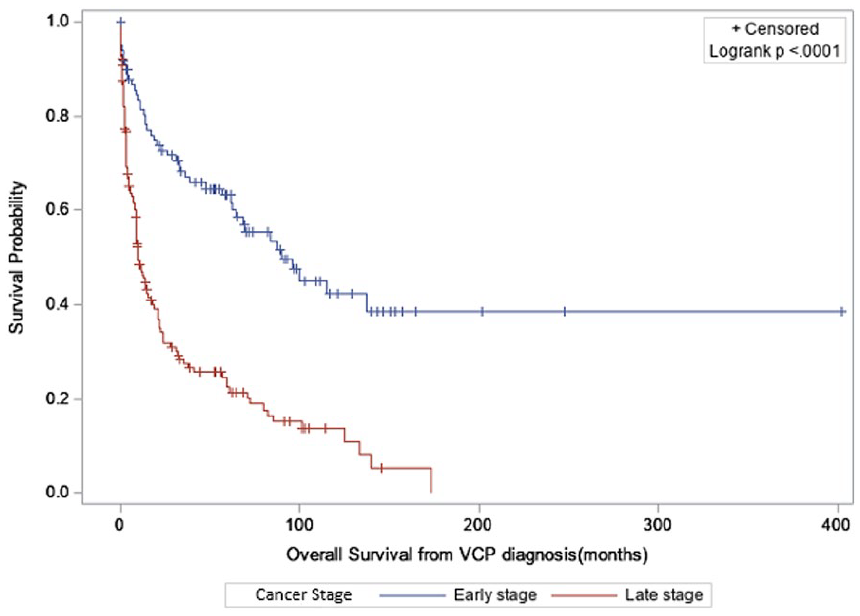
Overall survival early versus late stage.
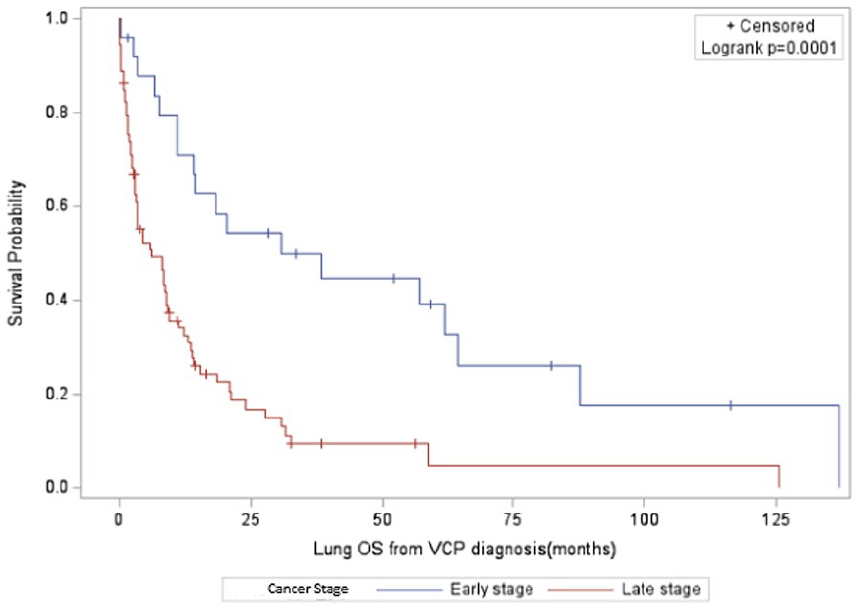
Overall survival—lung cancer.
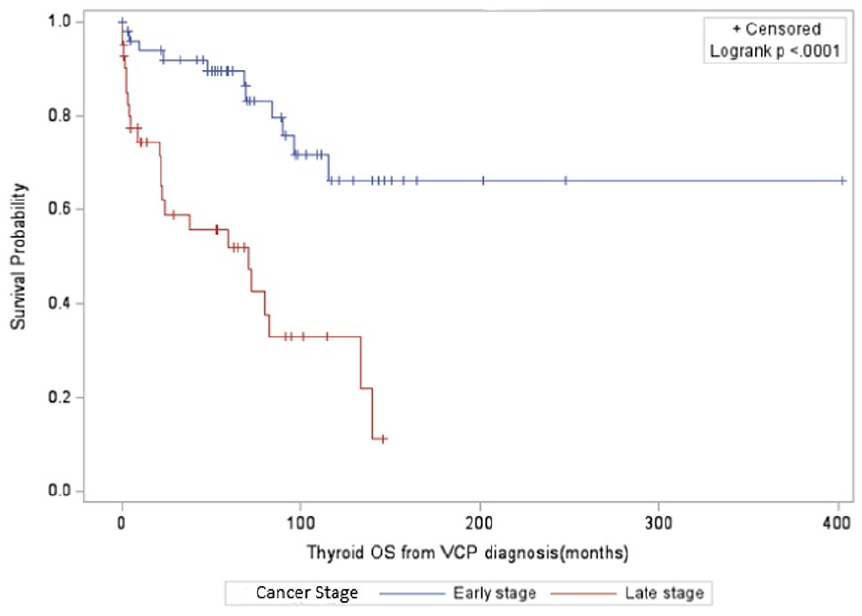
Overall survival—thyroid cancer.
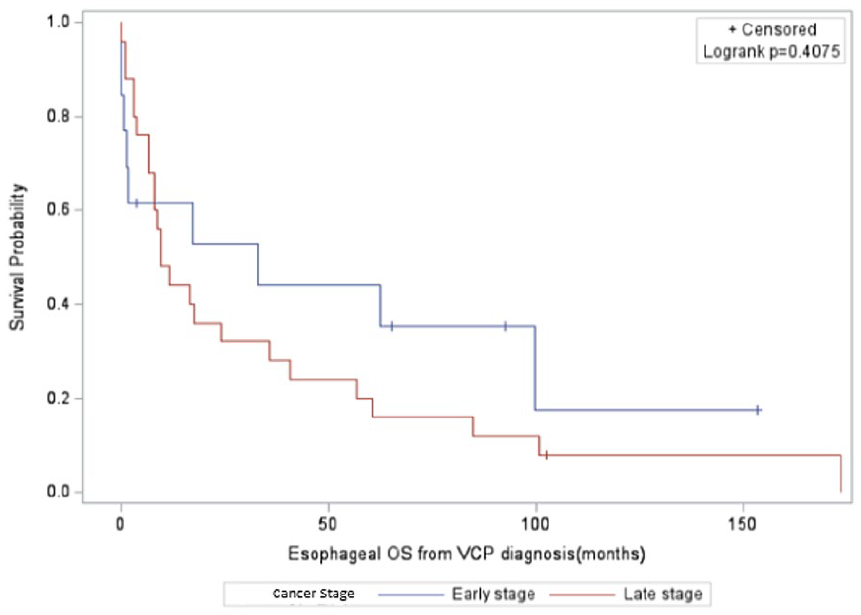
Overall survival—esophageal cancer.
Discussion
This study highlights a specific, under-recognized group: those with extralaryngeal malignancies who present with VCP due to their cancer diagnosis. Our results show that, given the improved longevity for patients diagnosed with cancer, even those with a historically poor prognosis, this population may benefit from durable VCP intervention.
It is important to recognize that in these patients, symptoms of VCP may often be overlooked, as the clinical focus remains on managing their malignancy. Moreover, standard oncology quality-of-life tools frequently fail to capture the unique impact of VCP. For patients with advanced cancer, where quality of life may supersede curative goals, VCP management deserves greater consideration.
In their review on management of unilateral VCP, Marques et al noted injection laryngoplasty’s effectiveness, noninvasiveness, and low rate of complications. 16 Vila et al also noted that patients who received early injection were less likely to undergo medialization thyroplasty, supporting the conclusion that early injection is justified given its low risk of complications and significant quality of life benefit. 17 In cancer patients, an important aspect to consider is prognosis and the time they have left to benefit from any interventions. Although neither study focused on oncology, the low-risk profile and functional benefits support early intervention in cancer patients.
Oftentimes, patients undergoing active cancer treatments may be significantly deconditioned and therefore be poor surgical candidates. One of the benefits of injection laryngoplasty is that it can be performed in the clinic without the need for general anesthesia. Ballard et al found no clinically meaningful difference in outcomes between clinic-based and operating room procedures, 18 further underscoring the feasibility of minimally invasive intervention.
Despite these advantages, injection laryngoplasty has a limited and variable duration of effect. Injectables can last 4 to 6 months for hyaluronic acid, 12 months for fat, and up to 18 months for calcium hydroxyapatite.19-22 Complications include under-medialization, which may require repeat procedures; over-medialization, which can be challenging to reverse; and superficial injections, which can disrupt the mucosal wave, leading to suboptimal, and potentially permanent, voice outcomes. By contrast, medialization thyroplasty offers long-term results with few complications, 23 and should therefore be considered for patients with extended survival, even in late-stage disease.
As cancer therapies advance and efforts in screening and early detection improve, patients are living longer and have increased benefit from interventions that enhance quality of life. For example, while lung cancer remains the leading cause of cancer-related deaths in the United States, survival rates have improved by 21% over the past 5 years.13,14 In our study, patients diagnosed with late-stage cancer demonstrated a mean OS of approximately 6.5 years. These findings suggest that the traditional approach—reserving vocal fold injections for patients with a “poor” prognosis and performing medialization thyroplasty only in those expected to survive long term—should be reconsidered. Today, the aim should be long-term functional outcomes with minimal risk, high reliability, and low complication rates, regardless of cancer stage.
This study’s retrospective design lends itself to several limitations. First, we can only speculate on the correlation between VCP and OS in patients diagnosed with extralaryngeal malignancies, given the lack of a control group. Despite our efforts, it was not possible to compare patients with cancer diagnoses of the same stage but without VCP to our population. This was due to the heterogeneity in the chart reporting on cancer staging, which precluded the ability to identify patients using ICD codes. This objective finding may have shed further insight into the relationship between VCP and OS.
In addition, our results mainly focused on cancer stage and survival. Although we discussed the profound impacts on quality of life that VCP can have, our study did not utilize any validated instruments to measure quality of life, given its retrospective nature. Prospective studies with formal quality of life assessments could better inform treatment decision-making in the future.
As an example, Kupferman et al found all their cancer patients benefited from injection laryngoplasty in terms of self-reported improvement in voice and airway protection. Seventy-one percent who were aspirating prior to the procedure no longer required a modified diet afterward. 6 Our study identified aspiration events in 37% of patients (n = 140). We did not include data on whether aspiration improved after intervention or if speech therapy was utilized as either a means of treating aspiration or as an alternative treatment modality for VCP, which is another important area of future study.
Furthermore, VCP may be transient, asymptomatic, or well compensated, all of which may have varying impacts on patient quality of life and treatment decisions. Understanding the natural history and outcomes in these subgroups could further inform management strategies.
Notably, a significant portion of our patients (n = 140) developed iatrogenic VCP, raising concerns about potential confounded data if the nerve was inadvertently injured intraoperatively. To mitigate this concern, we only included cases where the nerve was intentionally cut to allow for oncologic resection as identified during surgery and confirmed in the operative report.
In conclusion, cancer patients afflicted by VCP represent a unique and vulnerable population. There are many medical and social factors that influence decisions to pursue treatment. Despite these barriers, many patients survive months to years after diagnosis and are therefore at risk of impaired quality of life. The current preference for short-acting interventions in patients with limited prognosis should be reevaluated. Instead, these patients deserve access to interventions with low morbidity, few complications, and long-standing results.
Future studies should investigate quality of life outcomes associated with VCP management in cancer patients, compare intervention strategies, and evaluate matched controls without VCP. Such work could guide a more patient-centered approach to care.
Supplemental Material
sj-docx-1-ear-10.1177_01455613251360134 – Supplemental material for Life Expectancy in Patients Diagnosed with Extralaryngeal Malignancies and Vocal Cord Paralysis
Supplemental material, sj-docx-1-ear-10.1177_01455613251360134 for Life Expectancy in Patients Diagnosed with Extralaryngeal Malignancies and Vocal Cord Paralysis by Danae Alexandrou, Veronica Drozdowski-Nuccio, Kayeromi Gomez and Steven Charous in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
We thank Loyola University Medical Center for data access and Dr Charous for his guidance. We appreciate Dr Gomez for his assistance with data collection and analysis, and acknowledge the IRB for study approval. Finally, we appreciate the patients whose de-identified data made this research possible.
Ethical Considerations
This study was approved by the Loyola University Medical Center Institutional Review Board.
Consent to Participate
Verbal informed consent was required for the recruitment of patients to complete the survey via email and phone.
Author Contributions
All authors have contributed significantly to this manuscript. Specifically, the contributions are as follows:
Danae Alexandrou: writing – original draft, writing – review & editing, data organization - creation of tables and graphs.
Veronica Drozdowski-Nuccio, MD: conceptualization, methodology, writing – original draft, writing – review & editing.
Kayeromi Gomez, PhD: data collection, data organization, statistical analysis.
Steven Charous, MD: writing – conceptualization, methodology, review & editing, supervision.
All authors are in full agreement with the content of the manuscript and approve its submission to the Otolaryngology – Head and Neck Surgery Journal.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.