
Abstract
Diffuse idiopathic skeletal hyperostosis (DISH) is a condition that causes excessive bone growth along the spinal ligaments. While often silent, it can lead to symptoms such as neck pain or difficulty swallowing and, in rare cases, vocal cord paralysis (VCP). We present a 61-year-old man with progressive hoarseness due to DISH-related VCP. Early recognition of DISH as a cause of VCP is crucial, as timely diagnosis can guide appropriate management, ranging from conservative observation to surgical intervention in severe cases.
Keywords
Introduction
Diffuse idiopathic skeletal hyperostosis (DISH) is a systemic skeletal disorder characterized by progressive ossification of spinal ligaments. While often asymptomatic, cervical involvement can lead to dysphagia, airway obstruction, and, in rare cases, recurrent laryngeal nerve (RLN) compression resulting in vocal cord paralysis (VCP). 1 Given the limited number of reported cases, we present a case diagnosed with left-sided VCP secondary to DISH. This case highlights the possible underlying mechanisms and treatment considerations, contributing to a broader understanding of this rare manifestation.
Case Report
A 61-year-old male with type 2 diabetes mellitus presented with progressive hoarseness for 3 months. He denied dysphagia, dyspnea, weight loss, prior surgery, or trauma. Flexible laryngoscopy revealed left-sided VCP in a paramedian position (Figure 1). A comprehensive evaluation excluded neoplastic causes of unilateral VCP. Cervical radiography demonstrated bridging ossification anterior to the C2 to C7 vertebrae (Figure 2), while laryngeal computed tomography (CT) revealed severe anterior bony overgrowth at the left-sided C5 to C7 level with displacement of laryngeal soft tissue (Figure 3). Plain radiographs confirmed preserved intervertebral disc height, the absence of apophyseal joint bony ankylosis, and no sacroiliac joint erosion. Based on these findings, a diagnosis of DISH was established, which has contributed to RLN compression, resulting in unilateral VCP. In addition, direct cricoid impingement may have played a role in arytenoid fixation. Given his preserved voice and absence of airway compromise, conservative management was pursued.
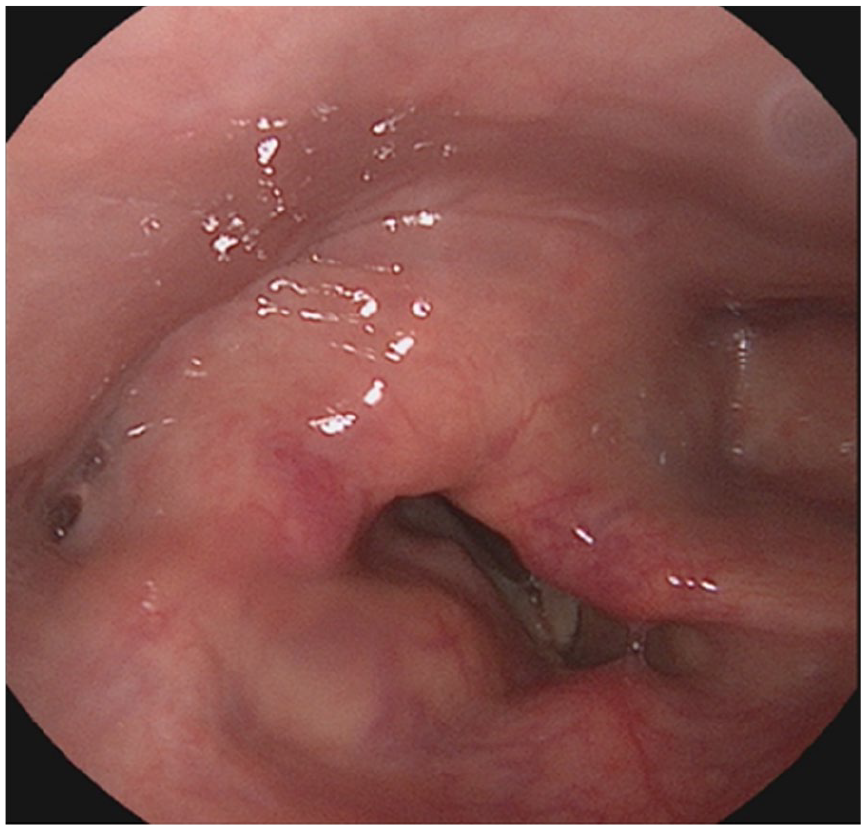
Flexible laryngoscopy revealed a left-sided vocal cord fixed in a paramedian position, accompanied by medial displacement of the left aryepiglottic fold.
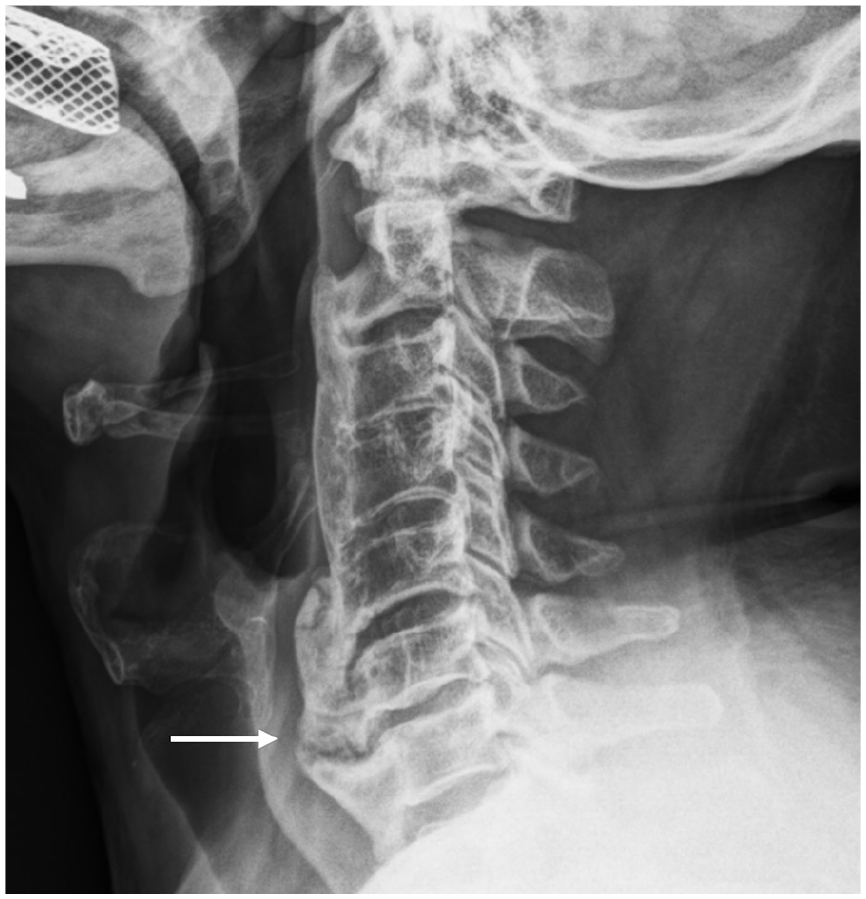
Cervical radiography demonstrated anterior bony bridging of the C2 to C7 vertebrae, with severe osteophyte formation predominantly at the C5 to C7 (arrow) levels.
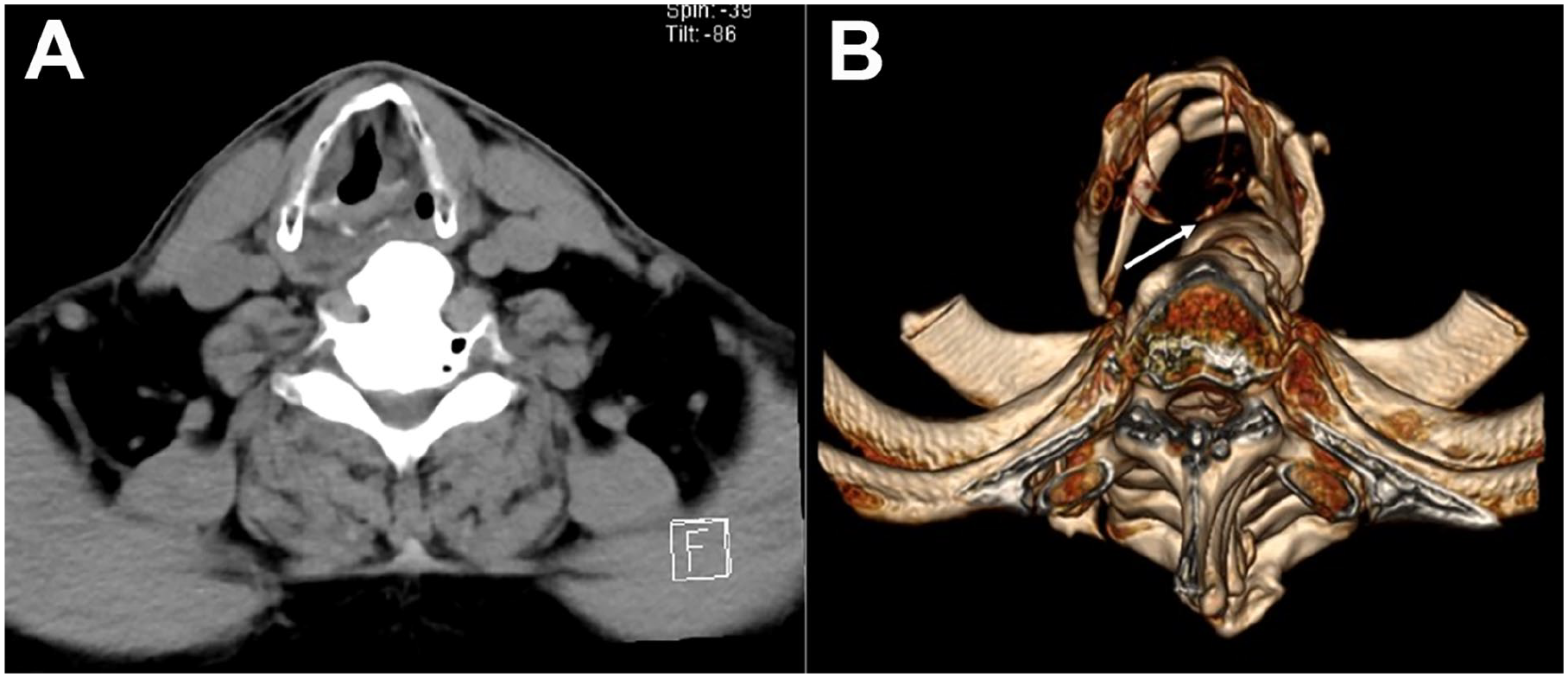
(A) Axial CT of the larynx revealed left-sided vocal cord paralysis, accompanied by a dilated left pyriform sinus and anteromedial deviation of the arytenoid cartilage. (B) Three-dimensional reconstruction of the CT showed prominent cervical osteophytes compressing the left post-cricoid larynx and arytenoid cartilage (arrow). CT, computed tomography.
Discussion
DISH is an age-related condition characterized by extensive ossification of spinal ligaments, particularly the anterior longitudinal ligament. DISH has been associated with older age, male sex, obesity, hypertension, atherosclerosis, and diabetes mellitus. The Resnick criteria remain the most widely used diagnostic standard, requiring (1) calcification and ossification along the anterolateral aspect of at least 4 contiguous vertebral bodies; (2) preserved intervertebral disc height with minimal degenerative changes in the affected area; and (3) absence of apophyseal joint ankylosis and no sacroiliac erosion, sclerosis, or bony fusion. 2
Although cervical DISH is often asymptomatic, it can lead to dysphagia, foreign body sensation, neck pain, spinal stiffness, and, in rare cases, VCP. The most common etiologies of VCP, as identified in our previous study, include iatrogenic injury (40.2%), neoplastic compression (29.9%), and idiopathic causes (10.7%). 3 In this case, after a comprehensive evaluation excluding all other potential etiologies, DISH remained the only plausible cause of unilateral VCP.
Including our case, a total of 10 DISH-associated VCP cases have been identified in the literature (Table 1). All affected individuals were older males, with a mean age of 71.2 years. Among them, 4 presented with bilateral VCP, while 6 had unilateral VCP without a laterality predominance. Several patients also had common comorbidities, including diabetes; and hypertension.
List of Detailed Information of Diffuse Idiopathic Skeletal Hyperostosis-Associated Vocal Cord Paralysis Cases.
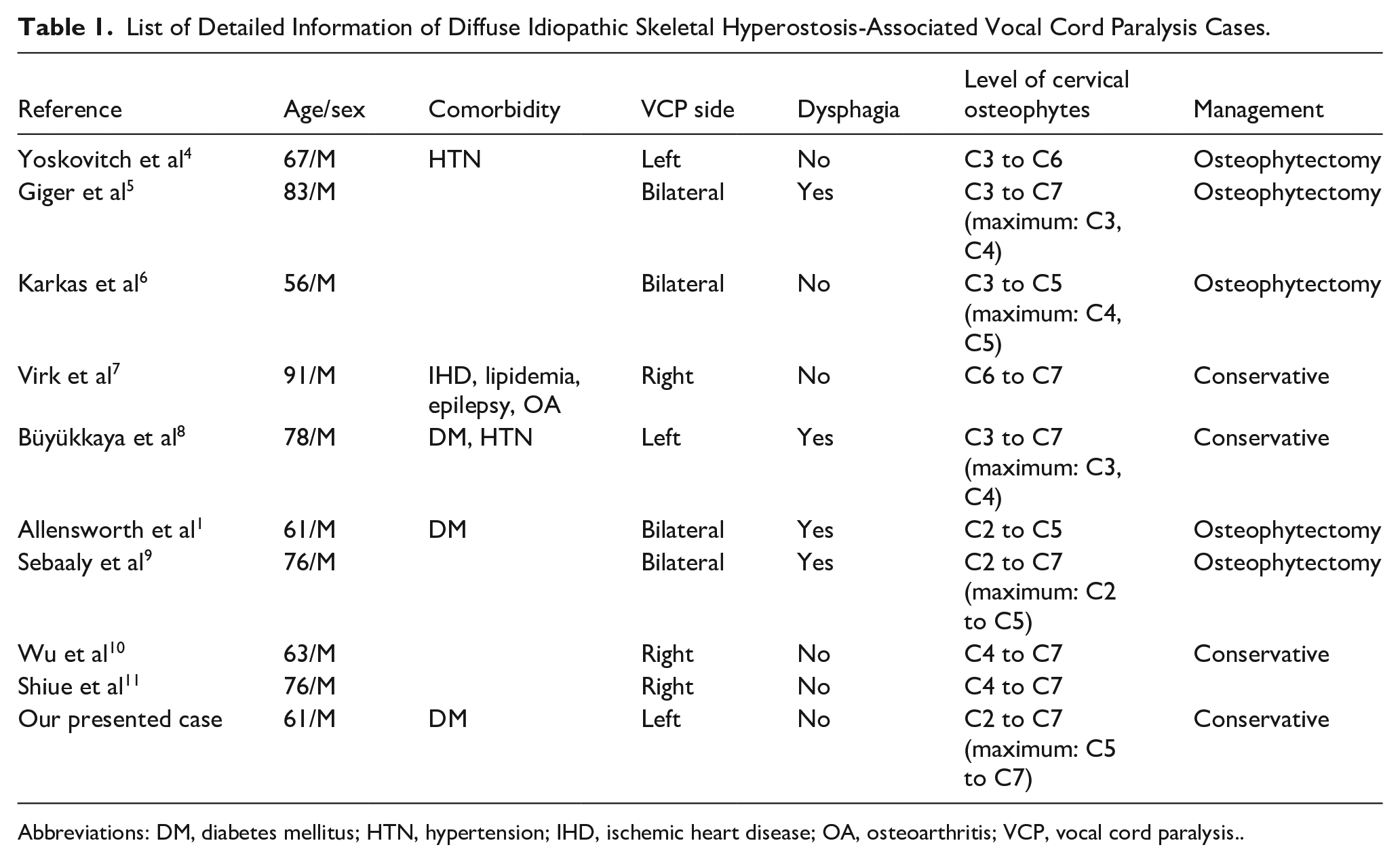
Abbreviations: DM, diabetes mellitus; HTN, hypertension; IHD, ischemic heart disease; OA, osteoarthritis; VCP, vocal cord paralysis..
The proposed mechanisms of VCP secondary to DISH include (1) direct RLN compression by cervical osteophytes, leading to true paralysis; (2) arytenoid cartilage fixation due to osteophyte impingement on the cricoarytenoid joint; and (3) vocal fold edema secondary to venous outflow obstruction, causing temporary immobilization. 1 In the present case, laryngoscopic examination ruled out vocal fold edema. Laryngeal CT revealed prominent cervical osteophytes compressing the post-cricoid larynx, which may have contributed to restricted arytenoid mobility. However, definitive confirmation of arytenoid cartilage fixation remains inconclusive, as operative direct laryngoscopy and electromyography were not performed. The compression of the RLN remains the most plausible mechanism underlying left-sided VCP in a paramedian position.
Dysphagia was not observed in this case, likely due to the anatomical distribution of hyperostotic involvement. In cervical DISH, dysphagia is most commonly associated with anterior osteophyte formation at the C3 to C5 levels, where the normal epiglottic tilt covers the laryngeal inlet. 12 However, in this patient, the most severe osteophyte formation was located at the C5 to C7 levels, which may account for the absence of dysphagia. Our analysis of 10 DISH-associated VCP cases further supports this observation, as cases of VCP with dysphagia predominantly exhibited osteophytes at upper cervical levels, whereas VCP without dysphagia was more frequently associated with lower cervical osteophytes (Table 1).
For patients with mild symptoms related to cervical hyperostosis, a non-surgical approach is generally preferred, including speech therapy, swallowing therapy, and dietary modifications. However, if dysphagia or airway obstruction worsens despite conservative management, surgical intervention may be necessary. Osteophytectomy is the primary surgical treatment aimed at symptom relief, with the anterolateral approach often favored for its optimal surgical access while minimizing excessive manipulation of surrounding structures. 13 Notably, in all 5 reported cases of DISH-associated VCP that underwent surgical intervention, vocal cord mobility was successfully restored, with favorable long-term outcomes (Table 1).
Conclusion
Though often asymptomatic, DISH should be considered in elderly males with progressive hoarseness, dysphagia, or respiratory distress. Cervical radiography can readily confirm this rare but identifiable condition, enabling timely diagnosis and appropriate management. This case highlights DISH as an uncommon cause of unilateral VCP, emphasizing the need to recognize skeletal hyperostosis in patients with unexplained hoarseness. While conservative management is appropriate for asymptomatic or mildly symptomatic patients, progressive dysphagia, airway obstruction, or bilateral VCP may necessitate surgical osteophytectomy.
Footnotes
Ethical Considerations
A written informed consent was obtained from the patient and was approved by Tri-Service General Hospital Institutional Review Board (TSGHIRB No. B202515009).
Author Contributions
Xin-Tian He: First author and preparation of draft.
Hsin-Chien Chen: Corresponding author and editing of manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a grant from the Tri-Service General Hospital (TSGH-A-114002 to Hsin-Chien Chen).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.