
Abstract
Unilateral vocal cord paralysis-related voice change is a common presentation in the otorhinolaryngology clinic. The well-known etiology was recurrent laryngeal nerve injury due to surgery, traumatic event, or tumor compression, but there are still other etiologies that could interfere with the route of the recurrence laryngeal nerve and lead to unilateral paralysis of the vocal cord. In this report, we presented a rare case of unilateral vocal cord paralysis resulting in diffuse idiopathic skeletal hyperostosis.
Introduction
Diffuse idiopathic skeletal hyperostosis (DISH) is a kind of skeletal disorder that causes calcification of ligaments, joint capsules, and tendon, which led to formation of bone spurs. The most common parts involved are the upper back, the cervical, to the thoracic spine. The spurs may compress the surrounding tissue or nerve and cause mostly subtle symptoms, pain, or stiffness. Less patients present with dysphagia or airway obstruction due to the elongated cervical spinal process. 1 The cases of voice change are even rare. The aim of this article is to report a case of DISH present with hoarseness.
Case Report
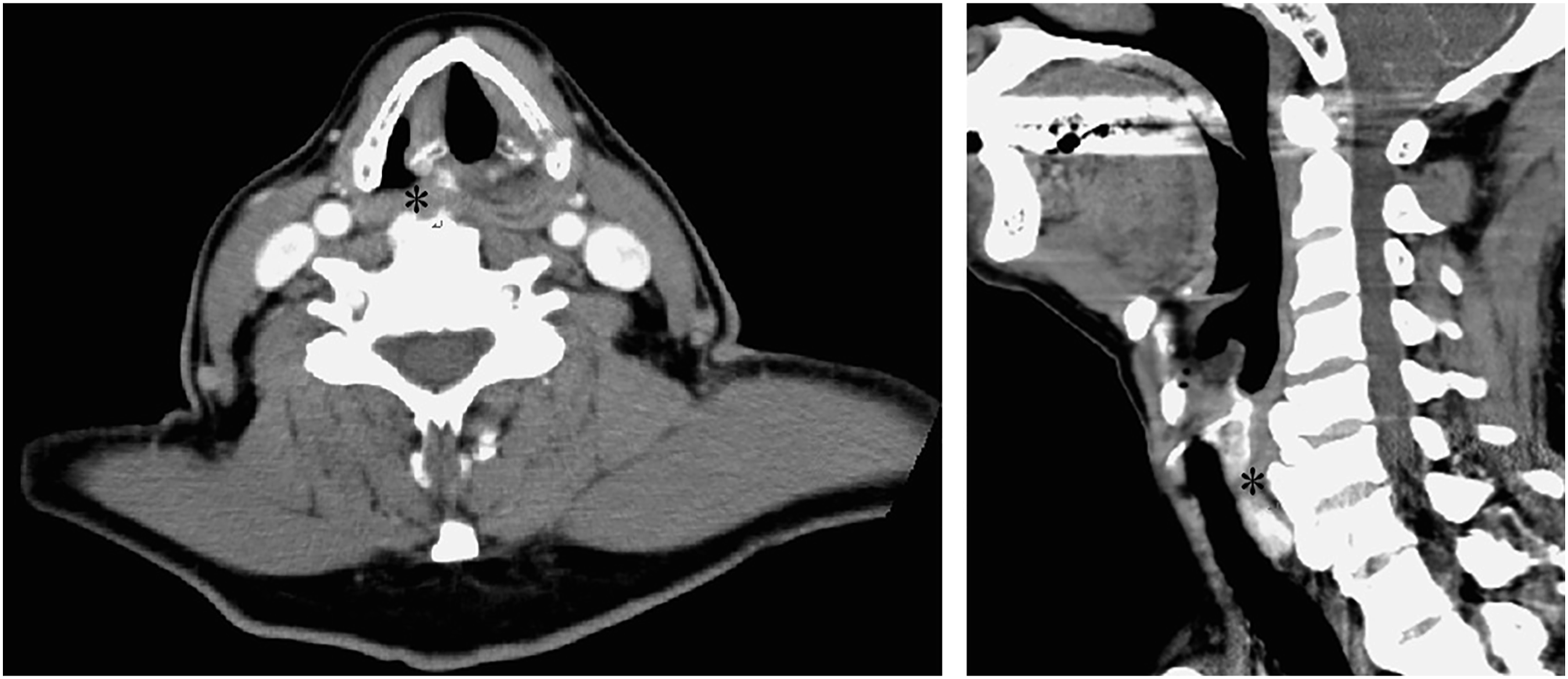
A 76-year-old man presented with a history of odynophagia over many years and hoarseness in the last two years. He denied any surgical history prior to the event. The laryngoscopy examination revealed a paralyzed right vocal cord, especially abduction (Figure 1). Under clinical suspicion of malignancy, diagnostic imaging modalities were performed. Contrast-enhanced face and neck CT demonstrated prominent anterior osteophyte formation, C4 through T6, with ossification of anterior longitudinal ligament and compression of the post-cricoid larynx (Figure 2), consistent with the diagnosis of diffuse idiopathic skeletal hyperostosis. Laryngoscopy showed a decrease in abduction of the right vocal cord (star). Contrast-enhanced computed tomography showed the presence of cervical spine osteophytes compressing the post-cricoid larynx (star) with atrophy of the left posterior cricoarytenoid muscle (PCA).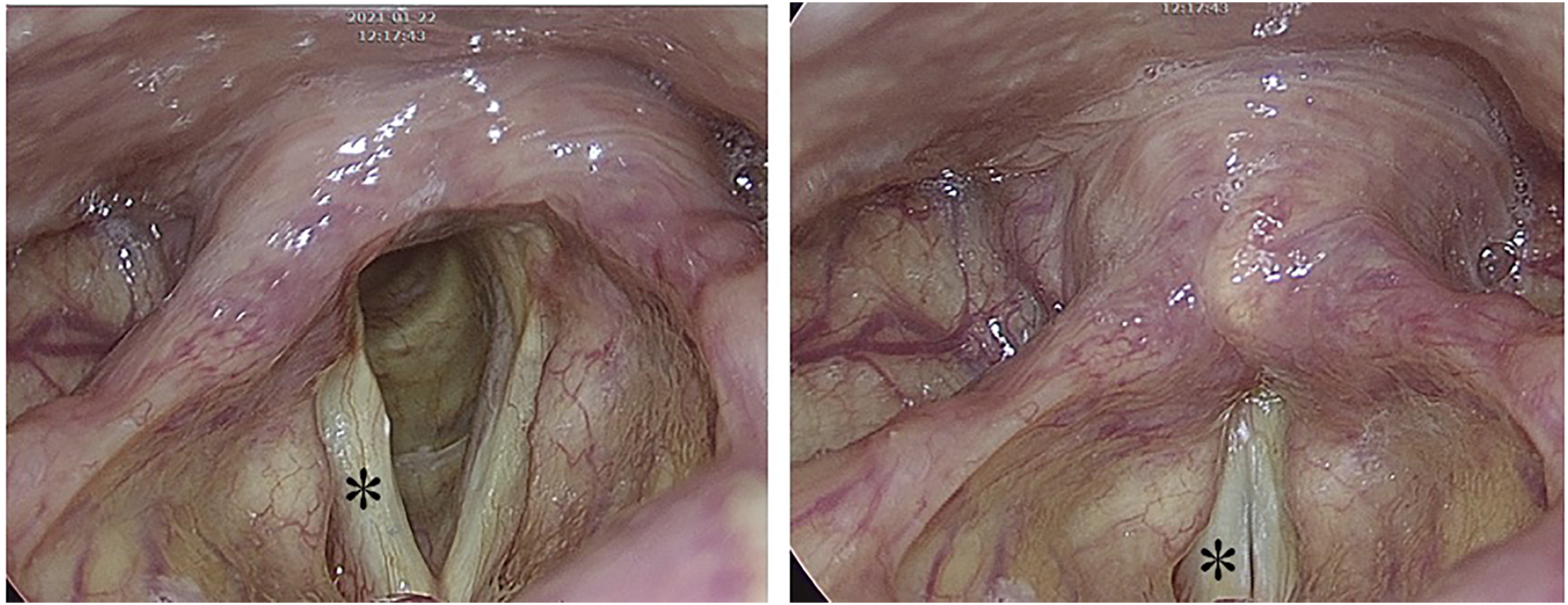
Discussion
Unilateral vocal paralysis, without known or suspected injury, is the most common result of malignancy. 2 However, other uncommon causes should still be considered. CT scan is strongly suggested to be performed routinely in this group of patients. Diffuse idiopathic skeletal hyperostosis is usually asymptomatic or slightly symptomatic. Dysphagia accounts for 75% of symptoms, but dysphonia accounts for only 2.5%. 3 In this case, the diagnosis of DISH might be omitted if no CT scan was performed. Detecting the underlying disease of unilateral vocal paralysis accurately is important for effective treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared that they have no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.