
Abstract

Hypocalcemia remains the most frequent complication following total thyroidectomy, with potentially serious clinical consequences ranging from neuromuscular irritability to cardiac arrhythmias.1,2 Its occurrence, even when transient, prolongs hospitalization and necessitates intensive monitoring and supplementation.1,2 Identifying patients at increased risk before surgery is therefore critical for early intervention and optimal postoperative care.
Our prospective study of 117 patients undergoing total thyroidectomy examined a broad panel of clinical and biochemical parameters to determine predictors of post-thyroidectomy hypocalcemia (Table 1). Consistent with earlier literature, lower preoperative calcium and vitamin D levels were associated with postoperative hypocalcemia. However, on multivariate analysis, only elevated preoperative serum phosphate remained a statistically significant independent predictor (Figure 1). Each unit increase in serum phosphate raised the likelihood of developing hypocalcemia by nearly 5-fold (OR = 4.7; 95% CI: 1.8-11.9). Notably, age, gender, and other commonly cited risk factors were not independently associated in our cohort.
Comparison of Preoperative Clinical and Biochemical Variables Between Patients With and Without Postoperative Hypocalcemia.

Abbreviations: ALB, albumin; anti TPO, antithyroid peroxidase; Ca, calcium; g/dl, grams per deciliter; Ca_intra, calcium measurements during operation; IU/ml, international units per milliliter; kg, kilograms; max, maximum; mEq/l, milliequivalents per liter; Mg, magnesium; mg/dl, milligrams per deciliter; min, minimum; ng/ml, nanograms per milliliter; pg/ml, picograms per milliliter; PO4, phosphate; pre, Ca_Pre, calcium measurements before operation; PTH, parathormone; T3, triiodothyronine; T4, thyroxine; time (min), operating time (min); TSH, thyroid stimulating hormone; μIU/ml, milli-international units per milliliter.
Statistical significance.
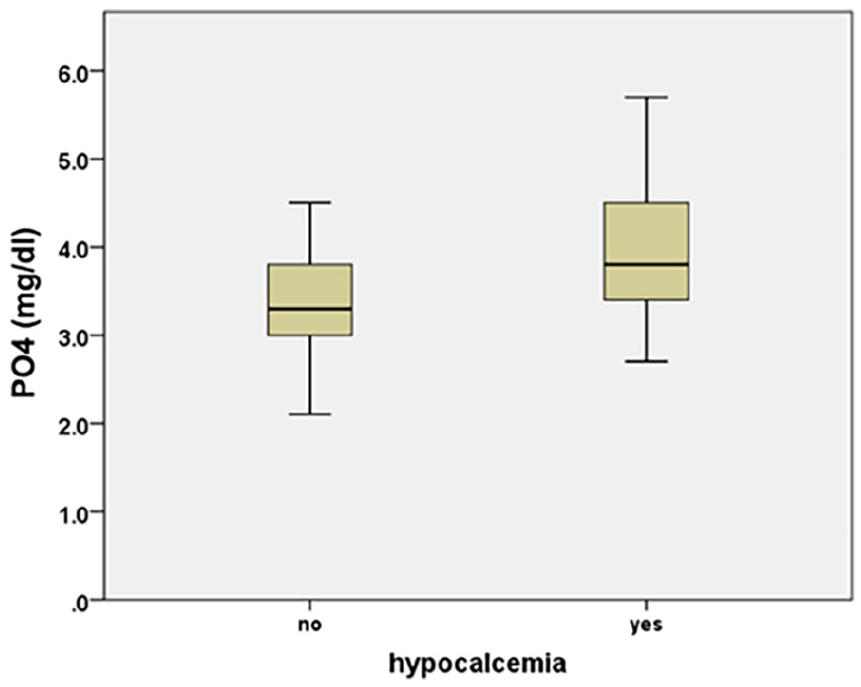
Boxplot showing preoperative serum PO4 levels in patients with and without postoperative hypocalcemia. PO4, phosphate.
These findings highlight the potential utility of serum phosphate – a readily available and inexpensive laboratory parameter – as a risk stratification tool in the preoperative evaluation of patients undergoing thyroidectomy. Although serum phosphate is routinely measured in certain medical contexts, such as chronic kidney disease or critical illness, it is not commonly included in standard pre-thyroidectomy workups. Yet the evidence emerging from our study, supported by findings from Sam et al, suggests that elevated phosphate levels may reflect subtle parathyroid dysfunction or reduced parathormone (PTH) activity prior to surgery – an impairment that may be unmasked or exacerbated by surgical manipulation or devascularization of the parathyroid glands. 3
Phosphate is intricately involved in calcium homeostasis. In physiologic conditions, PTH lowers serum phosphate by promoting renal excretion while increasing serum calcium through bone resorption and activation of vitamin D.4,5 Elevated phosphate in the presence of normal PTH levels may thus point to early or functional parathyroid insufficiency.4,5 Moreover, excess phosphate suppresses the renal enzyme 1-alpha-hydroxylase, reducing active vitamin D (calcitriol) synthesis and thereby impairing intestinal calcium absorption.4,5 These mechanisms suggest that phosphate may not only serve as a marker of risk but also contribute causally to hypocalcemia following thyroidectomy.
From a practical standpoint, integrating phosphate measurement into the routine preoperative evaluation could be a simple yet valuable addition. When interpreted alongside calcium, PTH, and vitamin D, it may help refine risk assessment. In our clinical setting, patients with elevated phosphate levels (>4.5 mg/dl) are now monitored more closely postoperatively, with consideration for early calcium supplementation and delayed discharge if other risk factors are present.
In settings where rapid PTH assays are unavailable – particularly in public hospitals or resource-limited regions – serum phosphate may serve as a surrogate early predictor of hypocalcemia. Unlike PTH, phosphate and calcium assays are widely available and inexpensive. Furthermore, since the decline in phosphate levels in response to intact PTH is more immediate than the subsequent rise in calcium, early postoperative phosphate may help identify patients at risk before overt hypocalcemia develops. 6 This is especially relevant in institutions where thyroidectomy patients are routinely hospitalized for at least 48 hours and fluid management is controlled, limiting confounding hemodilution effects. 6 In such contexts, serial phosphate monitoring in the first 24 to 48 hours postoperatively may provide timely and actionable insights. 6
Interestingly, parallels can be drawn from the field of parathyroid surgery, where the interplay between PTH and phosphate is central to postoperative management. 7 In parathyroidectomy, abrupt PTH withdrawal leads to a marked drop in phosphate excretion, often resulting in transient hyperphosphatemia – a phenomenon that reinforces the sensitivity of phosphate to dynamic PTH shifts. 7 Applying similar reasoning, subtle preoperative elevations in phosphate in thyroidectomy patients may reflect impaired PTH responsiveness, even before overt dysfunction is clinically manifest.3,6
While the predictive role of phosphate is increasingly recognized, the question arises as to whether preoperative correction of hyperphosphatemia could mitigate postoperative hypocalcemia. This remains speculative, as interventional data in this population are lacking. Prospective trials are needed to determine whether such strategies could translate into clinical benefit in thyroidectomy patients. Until then, individualized decision-making should prevail, particularly in those with borderline vitamin D levels or signs of impaired calcium metabolism.
The existing literature provides mixed support for the role of phosphate. Sam et al identified serum phosphate as a reliable predictor of hypocalcemia in vitamin D-replete patients. 3 However, Sousa Ade et al did not find any correlation between magnesium or phosphate and hypocalcemia. 8 These discrepancies may reflect differences in cohort composition, sample size, or analytical thresholds. Nevertheless, our findings – based on a systematically studied cohort with rigorous multivariate analysis – add weight to the hypothesis that phosphate is a clinically meaningful marker.
Future directions should focus on prospective investigations with larger sample sizes and standardized protocols that integrate phosphate into predictive models of hypocalcemia. In parallel, interventional studies evaluating whether correction of elevated phosphate levels can mitigate hypocalcemia risk would help clarify the clinical utility of this marker. As the field of thyroid surgery continues to evolve, a nuanced understanding of phosphate dynamics may offer new opportunities to optimize perioperative care and outcomes.
Footnotes
Ethical Considerations
The study was approved by the Institutional Review Board (IRB) of General Hospital of Ioannina “G. Hatzikosta.” The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Consent to Participate
Written informed consent was obtained from participants included in the report.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.