
Abstract
Objective:
To summarize recent emerging treatments for idiopathic intracranial hypertension (IIH) as an adjunct to surgical repair of cerebrospinal fluid leak by rhinology and skull base surgeons.
Data Sources:
PubMed and Embase databases.
Review Methods:
A literature review of aforementioned databases was performed on August 23, 2024, to identify studies from the past 5 years of acetazolamide alternatives and on September 16, 2024, for acetazolamide for the medical management of IIH. Data collected from studies included author, publication year, type of evidence, main findings, dosage, reported adverse effects, and medication studied.
Results:
Ten articles met screening criteria, and medications studied included the following: acetazolamide, topiramate, glucagon-like peptide-1 receptor agonists (GLP-1RAs), and 11-beta hydroxysteroid dehydrogenase type 1 (11β-HSD1) inhibitors. There were 4 randomized control trials, 1 pilot single-center study, 2 retrospective cohort studies, 1 retrospective case-control study, and 2 murine model basic science studies. There were significant findings supporting the case for increased research into their respective medications with hopeful clinical translation.
Conclusion:
Topiramate, GLP-1RAs, and 11β-HSD1 inhibitors are promising adjuncts or alternatives to acetazolamide and should be further investigated as effective IIH treatments.
Keywords
Introduction
Idiopathic Intracranial Hypertension (IIH), also known as primary pseudotumor cerebri syndrome, is a condition of increased intracranial pressure (ICP) due to a poorly-understood multivariable etiology that is often associated with women who are of childbearing age and frequently associated with recent weight gain. 1 There has been a rising incidence of IIH in the United States, likely secondary to increasing rates of obesity. 1 It has an estimated prevalence of about 2 out of every 100 000 patients in the general population, 2 but can be as high as 7.9 to 21.4/100 000 in the obese female population. 3
IIH is often treated by a multidisciplinary team that includes otolaryngologists, neurologists, neurosurgeons, and ophthalmologists. The most commonly-presenting symptoms of IIH include transient visual obscurations, visual field defects, and positional headaches, thus often being evaluated initially by ophthalmologists or neurologists. However, IIH can also present with venous phase pulsatile tinnitus, vestibular dysfunction, sensorineural hearing loss, and cerebrospinal fluid (CSF) leaks resulting in otolaryngology referrals. 1
Diagnostic criteria for IIH from the International Classification of Headache Disorders states that there must be an increased CSF pressure measured by lumbar puncture in recumbent position, epidural, or intraventricular monitoring with ≥20 cm H2O in nonobese, ≥25 cm H2O in obese, or ≥28 cm H2O in children with normal CSF studies. There must also be no evidence of other intracranial abnormalities, such as a mass or thrombus. 4
Given both IIH’s relevance and increasing prevalence make its management an important topic for otolaryngologists, IIH is currently treated via a combination of medical and surgical approaches. Weight loss is the main treatment for IIH. 5 Unfortunately, weight control is a challenging goal in acutely-affected patients and requires a multidisciplinary approach to be sustainable. 6 Surgical interventions for weight management have demonstrated both control of the papilledema and symptomatic control. 7 Acetazolamide is generally considered the first-line for pharmacological management of IIH. Although generally well-tolerated and supported, there are numerous side effects 8 associated with acetazolamide and differing evidence as to its true efficacy for IIH. 9 CSF shunts, optic nerve sheath fenestration, or endovascular dural venous stenting for patients with dural venous stenosis contributing to IIH remains as a surgical option for medically-refractory management of IIH. 1 The association of IIH with transverse venous sinus stenosis further highlights considering routine MRI for workup purposes. 10
Much of the literature regarding IIH within otolaryngology has focused on CSF leak repair outcomes with high rates of success,11,12 although medical management remains a crucial component of IIH treatment plans and to prevent further CSF leaks and other complications of IIH. There is ongoing discussion in the rhinology community about the benefit of pursuing medical management for IIH post-operation and the duration of treatment. One case series of 108 patients found a 92.82% success rate for patients who underwent surgical repair of spontaneous CSF leaks treated with either a CSF shunt or acetazolamide compared with those without postoperative intervention with an 81.87% success rate. 13 In contrast, a retrospective review of 33 patients found that only 4 patients with symptomatic IIH benefited from medical management and advised against adjuvant treatment due to side effect concerns. 14
While acetazolamide remains a reliable option, there has been increasing interest in other potential pharmaceutical options for IIH treatment such as topiramate, 9 glucagon-like peptide-1 receptor agonists (GLP-1RAs), 15 and 11-beta hydroxysteroid dehydrogenase (11β-HSD) inhibitors. 15 Herein this present study, we sought to synthesize the most recent literature regarding acetazolamide and its alternatives of medical management for IIH and highlight them for skull base practitioners.
Materials and Methods
Search Strategy
A literature review was conducted with the following 2 search strings: (1) “idiopathic intracranial hypertension” AND “topiramate” OR “glp-1” OR “acetazolamide” and (2) “pseudotumor cerebri” AND “topiramate” OR “glp-1” OR “acetazolamide.” These search terms were entered into PubMed and Embase with a filter of 2019 onward until search date to select papers published within the past 5 years. A search for acetazolamide alternatives was conducted on August 23, 2024, and for acetazolamide on September 16, 2024. All articles were reviewed. References of articles were also searched for additional relevant studies. Both authors Y.L. and A.E.A. completed searches and discussed any article inclusion discrepancies. A team of neuro-ophthalmologists and skull base surgeons also approved of final study selection and provided their clinical expertise as well as insight. Duplicates of findings were identified via Rayyan and excluded. A Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart outlines the literature review process (Figures 1 and 2).
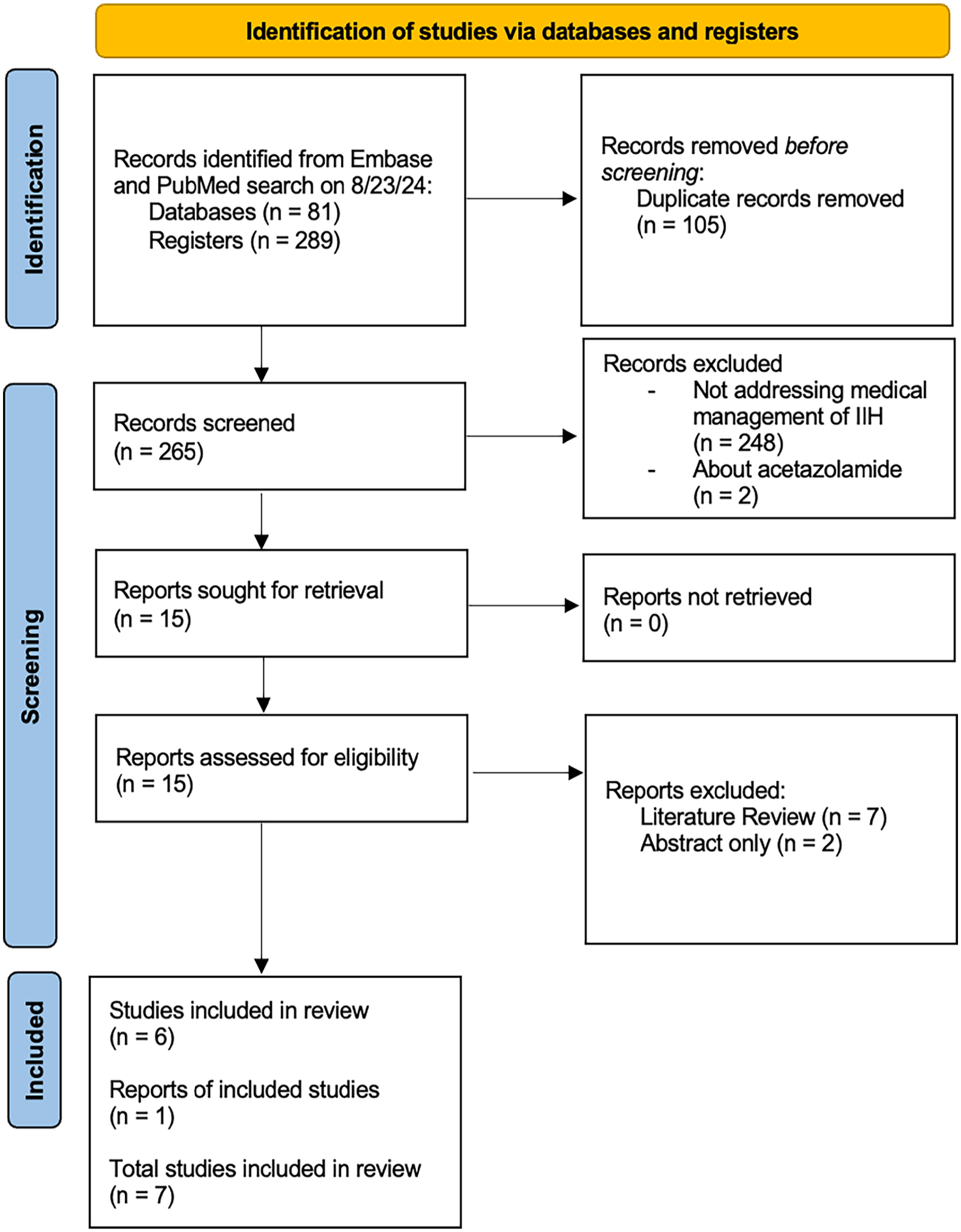
PRISMA flow diagram for alternatives to acetazolamide search conducted on August 23, 2024.
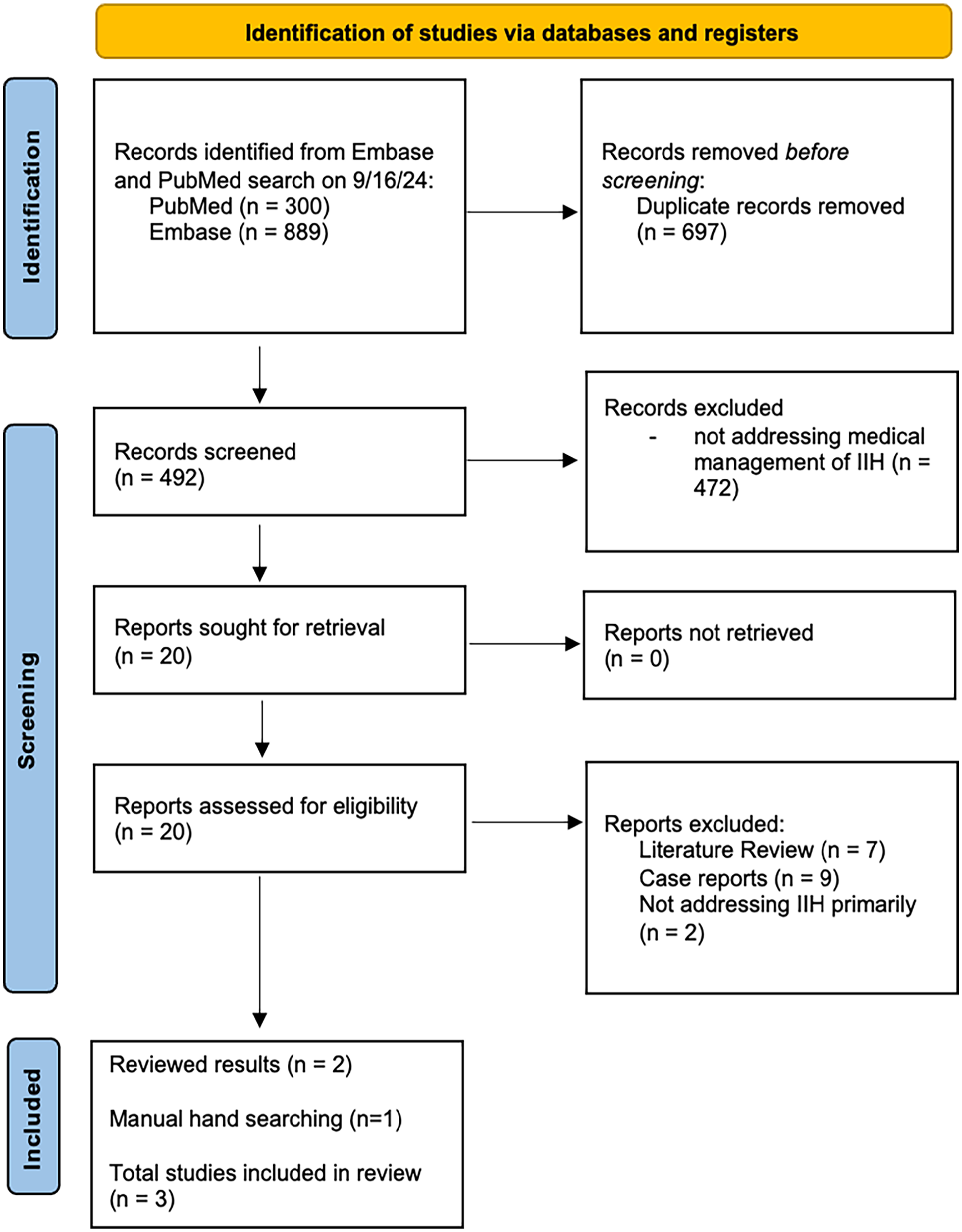
PRISMA flow diagram for acetazolamide search conducted on September 16, 2024.
Selection Criteria and Data Extraction
Inclusion criteria were that the paper had to examine the medical management of IIH with acetazolamide or its alternatives. Exclusion criteria included that the paper was examining other aspects of IIH treatment such as surgical management, not in English, case reports, a systematic/literature review, and no full text available. Data extracted from the papers included study design, type of evidence, author, publication year, medication studied, dosing, reported adverse effects, and the main study outcomes.
Results
A total of 10 articles were identified that fit inclusion criteria and summarized in Table 1. Seven articles were of acetazolamide alternatives (Figure 1) and 3 were of acetazolamide (Figure 2). Articles ranged in type and level of evidence with 4 randomized control trials (RCTs), 2 basic science murine model studies, 2 retrospective cohort studies, 1 retrospective case-control study, and 1 open-label single-center pilot study. Topiramate and acetazolamide were the most studied medications with 4 studies, respectively, while there were only 2 studies examining GLP-1s and 1 examining 11β-HSD inhibitors. Each study made a case for using their respective acetazolamide alternative either as a single treatment or in conjunction with acetazolamide. All selected studies examining human subjects included adult patients except for Jeon-Chapman et al. 16
Summary of Findings of Literature Review of Medications for Idiopathic Intracranial Hypertension Published Within the Past 5 Years (2019-2024).
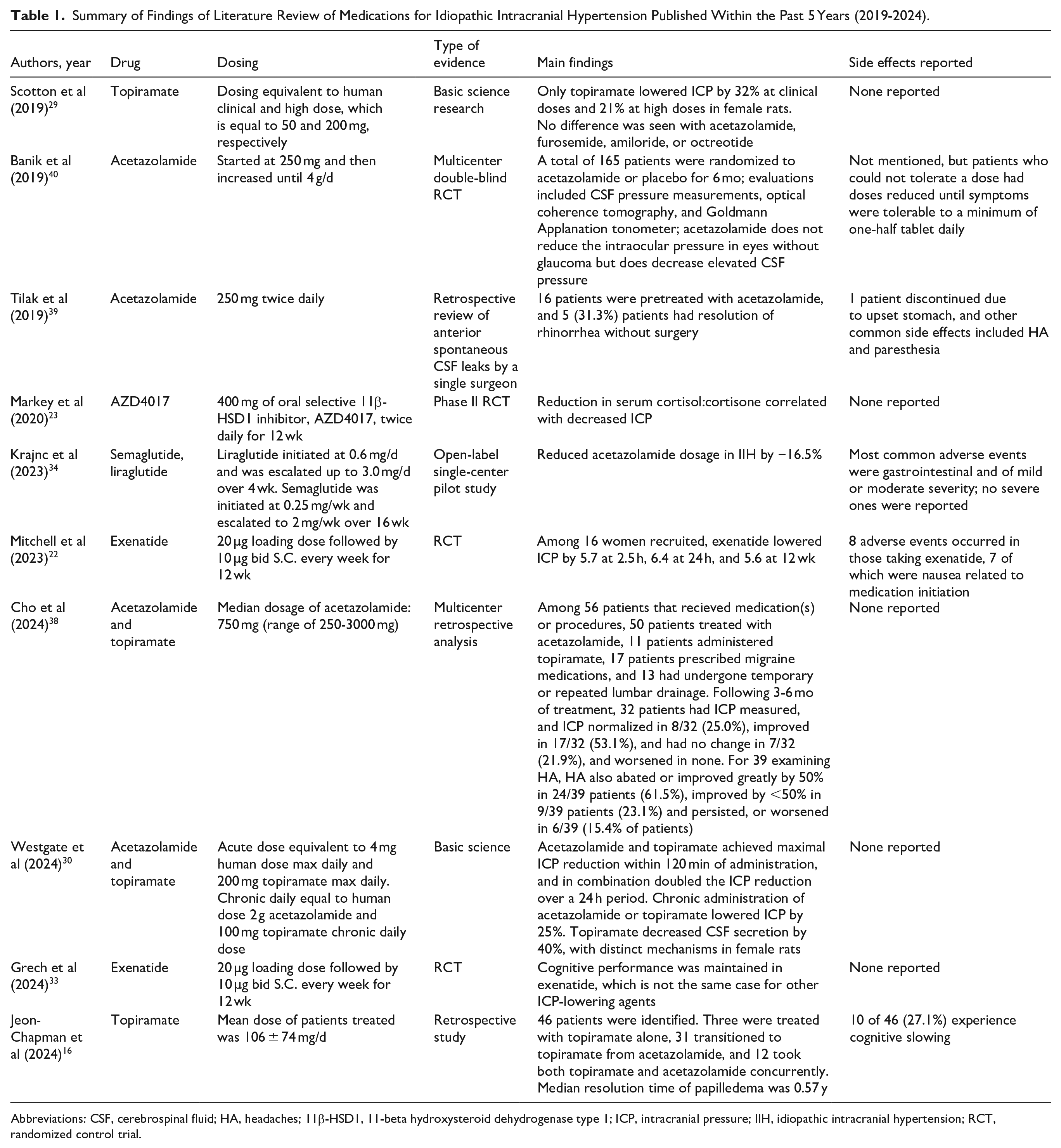
Abbreviations: CSF, cerebrospinal fluid; HA, headaches; 11β-HSD1, 11-beta hydroxysteroid dehydrogenase type 1; ICP, intracranial pressure; IIH, idiopathic intracranial hypertension; RCT, randomized control trial.
Studies range in efficacy demonstrating a reduced ICP, reduced amount of acetazolamide necessary, and maintaining cognitive performance. Most studies reported no adverse events, and for those that did, side effects of the medication were within the expected possibilities. A review of the mechanism of action (MOA), side effects, and how each medication treats IIH is detailed below. Acetazolamide alternatives are also outlined in Table 2 with MOA, comparison to acetazolamide, dosing, and level of evidence.
Summary of Acetazolamide Alternatives.
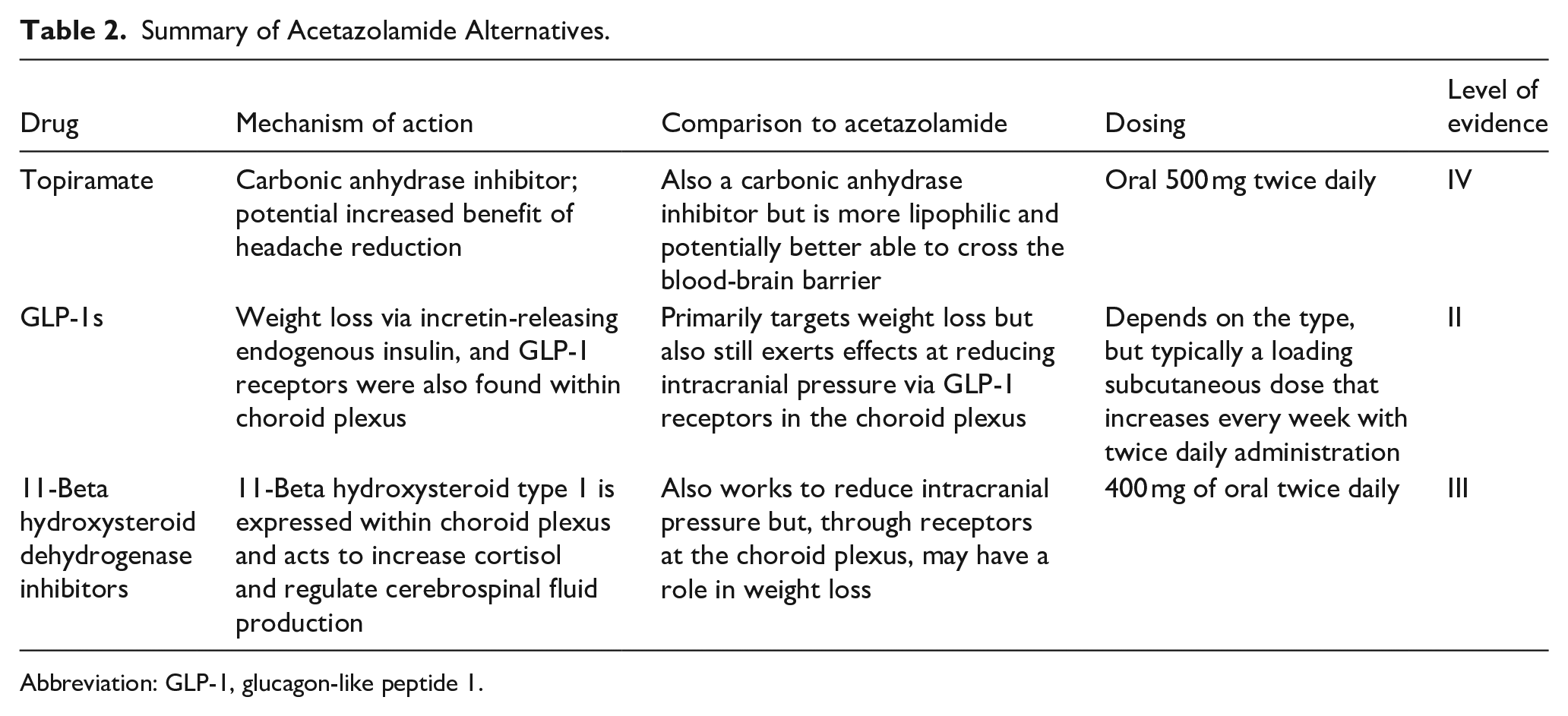
Abbreviation: GLP-1, glucagon-like peptide 1.
Acetazolamide
Acetazolamide is a carbonic anhydrase inhibitor (CAI) which leads to decreased CSF production and thus lowered ICP. 8 Acetazolamide also exerts numerous other effects throughout the body, as carbonic anhydrase is found within red blood cells, eyes, and the proximal tubule of the kidney and is an approved treatment for numerous other conditions such as glaucoma and altitude sickness. 17 The main and most common adverse effects include the following: fatigue, nausea, emesis, abdominal pain, and diarrhea. 17 Acetazolamide can be prescribed up to a maximum dose of 4 g daily; however, many lowered their dosage at around mean doses of 1.5 g due to adverse effects. 18 Current practice in the neuro-ophthalmological community is starting at around 500 mg twice daily and modifying the dose based on visual field and optical coherence tomography analysis. 19 Other clinicians may begin with acetazolamide at 250 to 500 mg twice daily and titrate as needed. 18
Topiramate
Topiramate is a second-generation antiepileptic drug used for the treatment of migraines and is approved for chronic weight management in individuals with a body mass index (BMI) >30 kg/m2. 20 There are also many other off-label uses such as prevention of cluster headaches and managing Tourette and Prader-Willi syndromes. Topiramate’s primary MOA involves enhancing GABA-A receptor activity; however, it also has some weak CAI effects, making it a potential treatment for IIH. 20 Some neurologists consider topiramate second-line for refractory IIH, but there are theories that it may be superior to acetazolamide as it is a more lipophilic CAI and potentially able to better cross the blood-brain barrier. 9
Topiramate’s most common side effects often involve the central nervous system resulting in effects such as fatigue, dizziness, and somnolence with the most worrisome being memory loss in about 10% and confusion in 20% of cases. 20 There is also an association with metabolic acidosis risk due to the inhibition of carbonic anhydrase isozymes as well as acute myopia and secondary acute angle-closure glaucoma. Hepatotoxicity is also a risk. 20
Glucagon-Like-Peptide 1 Receptor Agonists
GLP-1RAs are medications (eg, -tide suffix medications, such as semaglutide, exenatide) used to treat type 2 diabetes and obesity. GLP-1RAs have been recommended in the 2023 American Diabetes Association guidelines for lowering cardiovascular risk. 21 These medications work via promoting GLP-1, which is an incretin hormone that stimulates insulin secretion. These medications are often dosed subcutaneously as they have poor oral bioavailability. 21 The main side effects of GLP-1RAs include gastrointestinal effects such as nausea and diarrhea.
GLP-1RAs have also been shown to regulate fluid secretion and increase diuresis at the renal proximal tubule. 22 GLP-1Rs are also expressed in the choroid plexus, which is the predominant area of CSF production in the brain. 22 GLP-1RAs also promote weight loss and obesity, which is a major risk factor for IIH. 22
11-Beta Hydroxysteroid Dehydrogenases Inhibitors
11β-HSD type 1 (11β-HSD1) is expressed in the choroid plexus to increase cortisol availability and regulate CSF production. 23 It has also been shown that 11β-HSD1 is dysregulated in obesity. There have been selective inhibitors of 11β-HSD1 that have been developed for the treatment of obesity, hepatic steatosis, metabolic syndrome, and type 2 diabetes. These benefits are modulated by the regulation of glucocorticoids. 24 11β-HSD1 inhibitors are receiving increasing interest as a potential therapy for numerous conditions. There have been minimal adverse effects reported thus far, but this remains an active area of research. 23
Discussion
This review sought to present otolaryngologists with the most recent literature (within the past 5 years) regarding the nonsurgical treatment options for IIH. As previously mentioned, acetazolamide is the standard of care for the medical management of IIH; however, one study has reported varying levels of efficacy. 1 Previous studies have established improvements in papilledema, visual impairment, quality of life, and ICP, but the extent to which these benefits apply to certain symptoms or patients remains unclear.1,25,26 In particular, acetazolamide appears limited in its ability to alleviate headaches due to the observation that the headaches associated with IIH do not necessarily correlate with ICP. Moreover, headaches can potentially persist even after the resolution of IIH or may be unrelated to ICP or IIH altogether. 27 Additionally, acetazolamide can be difficult to tolerate due to adverse effects, such as fatigue, nausea, vomiting, diarrhea, and tinnitus. 7 Consequently, there is interest in exploring other pharmaceutical options. While the literature on these alternative medications is limited, the published data are certainly promising. The medications outlined in this review exhibit differing mechanisms of action, but in common, they appear to have some impact on CSF production and weight loss.
Topiramate, which can promote weight loss, also has the potential to inhibit carbonic anhydrase and thus reduce CSF production due to its similar structure to acetazolamide.9,28 Additionally, as a medication that is already indicated for headaches, it may have added benefits for the common headache symptoms of patients with IIH. 9 Our review highlights 2 basic science and 1 retrospective study on topiramate for IIH management. Scotton et al compared topiramate to a variety of other medications (acetazolamide, amiloride, octreotide, and furosemide) to measure changes in ICP in rodents. They found that only subcutaneous administration of topiramate significantly lowered ICP (by 32% at clinical doses). Oral administration of topiramate and acetazolamide was tested, and again, there was a significant ICP reduction in topiramate only. 29 However, it is important to note that this study is limited by its use of a non-diseased rat model and not by assessing the effects of repeat dosing.
Westgate et al also explored the effects of topiramate (and acetazolamide) in a randomized crossover design rat model but measured both the acute and chronic effects of treatment. Over the acute 24 hour period, both medications significantly decreased ICP and had the greatest effects when given in combination. Chronically, over 10 days of administration, both groups saw a significant reduction in ICP, and they also showed a reduction in CSF production in the topiramate group. Moreover, they observed different changes in gene expression associated with CSF secretion between the 2 groups, highlighting the likelihood that the 2 medications have distinct mechanisms of action. 30 Like the previously-mentioned study by Scotton et al, the use of rodents in this investigation, particularly non-diseased models, creates uncertainty when trying to extrapolate these findings to humans.
Another topiramate study by Jeon-Chapman et al retrospectively analyzed pediatric patients with IIH with a focus on the course of papilledema and headaches, with a variety of cohorts including the following: those who were switched from acetazolamide to topiramate due to insufficient improvement or inability to tolerate acetazolamide, concurrent treatment with both, and those treated with topiramate alone from the start. 58.7% of the patients on topiramate had improved headache, and all patients on topiramate alone had resolution of papilledema. Notably, the most common side effect was cognitive slowing in 21.7% of patients. 16 The study was limited in its retrospective nature and sample size, with a cohort of only 3 patients who started on topiramate alone. Given its retrospective nature, there was also a notable degree of heterogeneity in follow-up intervals, subjective reporting of headache symptoms, and availability of fundus photography or papilledema grading.
In addition to the well-known weight loss effects of GLP-1RAs, GLP-1Rs are expressed within the choroid plexus, and in 2017, a rodent study displayed that the activation of these receptors resulted in reduced CSF production and ICP.31 -33 These findings have begun to be translated to human patients with IIH, and in our review exhibited the highest degree of evidence, with 2 RCTs and an open-label single-center case-control pilot study.22,31,34 Mitchell et al primarily assessed the changes in ICP between exenatide and placebo and found that exenatide was superior in reducing ICP at 2.5 and 24 hours. This effect remained at the 12th week but was not statistically different than the placebo group. The authors highlighted that due to the propensity for a rapid decline in patients with IIH, it is advantageous that exenatide appeared to have a rapid onset of action. 22 Importantly, in the aforementioned comparison between acetazolamide and topiramate by Westgate et al, they reported a maximal ICP reduction within 120 minutes. 30 Thus, GLP-1RAs may also prove to be amenable to countering rapid increases in ICP among patients with IIH. Mitchell et al also mentioned that due to the lack of a significant change in body weight and the improvement in ICP at such a short interval (2.5 and 24 hours), it would be reasonable to conclude that the mechanism relates more to its action on CSF as opposed to weight loss. 22 Despite its randomized design, the limitations include a focus on ICP exclusively, as opposed to other important manifestations of IIH. Additionally, the groups were not matched according to baseline headache frequency and severity or degree of visual field deficits.
In the case-control study by Krajnc et al, 2 other GLP-1RAs were studied, semaglutide and liraglutide, which achieved a greater percentage of weight loss than in control. They also observed a significantly-higher reduction in headaches and decreased need for acetazolamide than in the control group. 34 This study was limited in its lack of randomization or blinding and did not account for events that may influence outcomes such as smoking cessation. Beyond weight loss, these studies indicate that GLP-1RAs may reduce ICP, improve quality of life, and reduce the reliance on acetazolamide (especially for patients who do not tolerate it). GLP-1RAs have also increasingly been studied and shown to be efficacious for a myriad of other conditions, including headaches and pain. 35
11β-HSD1, which is also expressed in the choroid plexus, has previously been linked to the pathogenesis of IIH. Prior studies have revealed increased levels of 11β-HSD1 in the disease and an association between decreased levels of 11β-HSD1 and reduction in ICP.36,37 These findings give way to a potential therapeutic target for inhibition examined by 1 RCT. Markey et al showed a significant decrease in the ratio of serum cortisol to cortisone over 12 weeks in the treatment group compared with that in control, which correlated with a decrease in ICP. It also appeared safe and well-tolerated with no reported adverse effects. 23 Importantly, this investigation could not directly evaluate 11β-HSD1 inhibition at the choroid plexus, but rather it was inferred through biomarkers, and thus could not definitively conclude the medication’s impact on the target tissue. Furthermore, the sample size was small, and the study time period was likely too short to observe the extent of clinical efficacy.
We also assessed recent literature for the widely used and first-line acetazolamide and found there to be a relative paucity of high-level evidence within recent years. A landmark study by Wall et al, 7 examined 165 patients with IIH in a multicenter, double-blind, randomized placebo-controlled trial. All participants underwent lifestyle modification programs, which included low sodium diet and lifestyle management. They found that there was modest improvement in visual field function. 7 While this study was strong in design and encouraging in its outcomes, additional research must corroborate its findings.
With some exception, recent studies regarding acetazolamide tend to be case reports or do not primarily examine acetazolamide, such as Cho et al, 38 which makes distinguishing individual treatment effects difficult. While it was a retrospective review, Tilak et al reported impressive findings in their analysis of patients with spontaneous CSF rhinorrhea treated with acetazolamide prior to undergoing surgical repair. Based on their findings, they proposed considering a trial of acetazolamide prior to committing to surgery, as nearly one-third of their patients achieved CSF leak resolution and avoided surgery altogether. 39 In a double-blinded RCT, Banik et al examined intraocular and CSF pressure between IIH patients treated with acetazolamide compared with placebo. They found that acetazolamide did not reduce intraocular pressure in patients without glaucoma, but it did reduce CSF pressure. 40
While we sought to be thorough in our literature search, there is a possibility that our search missed relevant studies. There is also the inherent bias of published literature to only include significant data to support hypotheses, thus lacking contrary data. Future studies should seek to address the limitations of the included studies and investigate the combination of these medications as well as newer weight loss medications. This advancement can be achieved via head-to-head studies between the medications examined in this review, and also more human trials in general for medications studied in animal models in the present review. More research is necessary to more fully differentiate and support first-line medical management for IIH in addition to publishing more updated IIH management guidelines that include otolaryngologists and skull base surgeons. While there is insufficient evidence to make current specific practice change recommendations, there is support to warrant clinical trials comparing IIH medications. Additional future research would also benefit from considering the use of these medications as adjuncts to surgical CSF leak repair to support a comprehensive care plan for patients with IIH that includes both surgical and medical options.
Overall, while limited as a whole, there are enough data for otolaryngologists to increase their understanding of the various pharmaceutical options available for IIH management and hope for a more comprehensive approach for otolaryngologists to treat patients with IIH. From the limited data that currently exist regarding medical IIH management, otolaryngologists should consider implementing acetazolamide and alternatives into their practice. However, until formal IIH management guidelines are created, we recommend that every patient be evaluated holistically with other comorbidities in mind. For example, if there is a patient with a high BMI, a GLP-1RA may be considered, as opposed to another patient with a more primary complaint of headaches may be recommended topiramate. Moreover, while our stated findings from this review are encouraging in terms of the potential efficacy of alternatives to acetazolamide, there are potential risks to these other agents that must be considered on an individual patient basis. These include topiramate’s potentially-adverse cognitive effects 9 and the recent attention received by GLP-1RA’s for neurological side effects (eg, dizziness, tremor) that may be exacerbated among patients with neurological conditions. 41 In addition, we feel it is imperative to continue to collaborate with a multispecialty team in treating IIH (eg, neuroophthalmology) due to the prevalence of chronic unrelated headaches and the most likely cause of permanent morbidity being blindness.27,42,43
Conclusion
IIH remains an important condition for otolaryngologists to not only diagnose and recognize but also understand how to treat both surgically and medically. With the continuing improvement in and the release of new weight-loss medications, it is important for otolaryngologists to understand their utility for treating IIH. Additionally, otolaryngologists should remain up-to-date on the newer findings regarding the evidence for acetazolamide alternatives, especially for those with refractory headaches or intolerance to acetazolamide. Together, with other specialties and improved medications, there is a real potential to help improve the treatment of patients with IIH.
Footnotes
Ethical Considerations
This article does not contain any studies with human or animal participants.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.