
Abstract
The main objective of this report was to describe a very unique clinical case of a post-traumatic temporal bone encephalocele with lateral ventricle herniation. This report involves a 60 year-old male who initially presented with right-sided hearing loss, otorrhea, and clear rhinorrhea with metallic taste and a history of a temporal bone fracture managed conservatively 6 years prior to presentation. Computed tomography (CT) revealed a large right tegmen defect and magnetic resonance imaging demonstrated herniation of a significantly-distended lateral ventricle into the mastoid cavity. The patient underwent a combined transmastoid and middle fossa approach for encephalocele removal and tegmen repair. However, 3 months later, follow-up CT scan showed an asymptomatic subacute subdural hematoma (SDH) managed with successful bur hole drainage. Long-term follow-up especially in large skull base defects is critical to monitor delayed occurrence of encephalocele and/or cerebrospinal fluid (CSF) leak. Surgical repair with the removal of devitalized brain tissue and multilayer closure may result in the development of subacute SDH after successful repair.
Introduction
Temporal bone fracture (TBF) occurs in traumatic head injuries 18% to 40% of the time. The incidence of developing a CSF leak following a TBF ranges between 11% and 45%. 1 TBF with CSF leaks are usually managed conservatively because spontaneous resolution can be expected in 95% of cases within 2 weeks. 1 Temporal bone encephaloceles (TBE) are rare and late phenomena that can present from 1 to 21 years after initial trauma. In a case series of surgically-repaired TBEs with CSF leak, history of trauma was reported in 7.5% to 33% of patients.2 -4 Major skull base defects (>1 cm) are more often associated with encephaloceles as opposed to small defects (78% vs 29%). 4 Anterior middle fossa encephaloceles predispose patients to seizure development. 5 In this report, we describe a case of a 60 year-old man who developed a TBE with significant lateral ventricle herniation 6 years after a TBF that was initially conservatively managed. This case teaches skull base practitioners about the importance of long-term follow-up for patients with large skull base defects and highlights the depth of potential invasion of brain herniation into the mastoid cavity. The necessary written informed consent was obtained from the patient for the publication of this case report.
Case Report Description
A 60 year-old male presented with right-sided hearing loss, otorrhea, and clear rhinorrhea with metallic taste. Six years prior to presentation, he sustained a TBF falling from a moving vehicle. He reportedly had CSF leak, which was managed conservatively at the time at an outside institution. He experienced recurrent grand mal seizures after the accident but had been seizure-free for 4 years. He lacked follow-up due to social issues.
Physical examination was significant for intact tympanic membranes without effusion and right greater than left sensorineural hearing loss. Computed tomography (CT; Figure 1A and B) revealed a large right tegmen defect. Magnetic resonance imaging (MRI; Figure 1C and D) demonstrated herniation of a significantly-distended lateral ventricle into the mastoid cavity. The patient underwent a combined transmastoid and middle fossa approach for encephalocele removal and tegmen repair. Intraoperatively, the tegmen defect was 1.5 cm antero-posterior by 3 cm transverse. The defect was repaired intradurally with temporalis fascia and extradurally with autologous bone fragment, fascia lata, and abdominal fat. Lumbar drain was placed for 7 days. Tissue within the mastoid was sent to pathology where immunohistochemical staining with adequate controls and glial fibrillary acidic protein (GFAP) highlighting neural tissue, ultimately confirming the diagnosis of encephalocele. Three months after the surgical repair, the patient had no new symptoms, but a follow-up CT head showed subacute subdural hematoma (SDH) with midline shift (Figure 2A). The patient underwent right burr hole for the drainage of the SDH. One month after the burr hole procedure, he was doing well with resolving chronic SDH (Figure 2B). Reconstruction is shown on 4 month postoperative CT (Figure 2C and D).
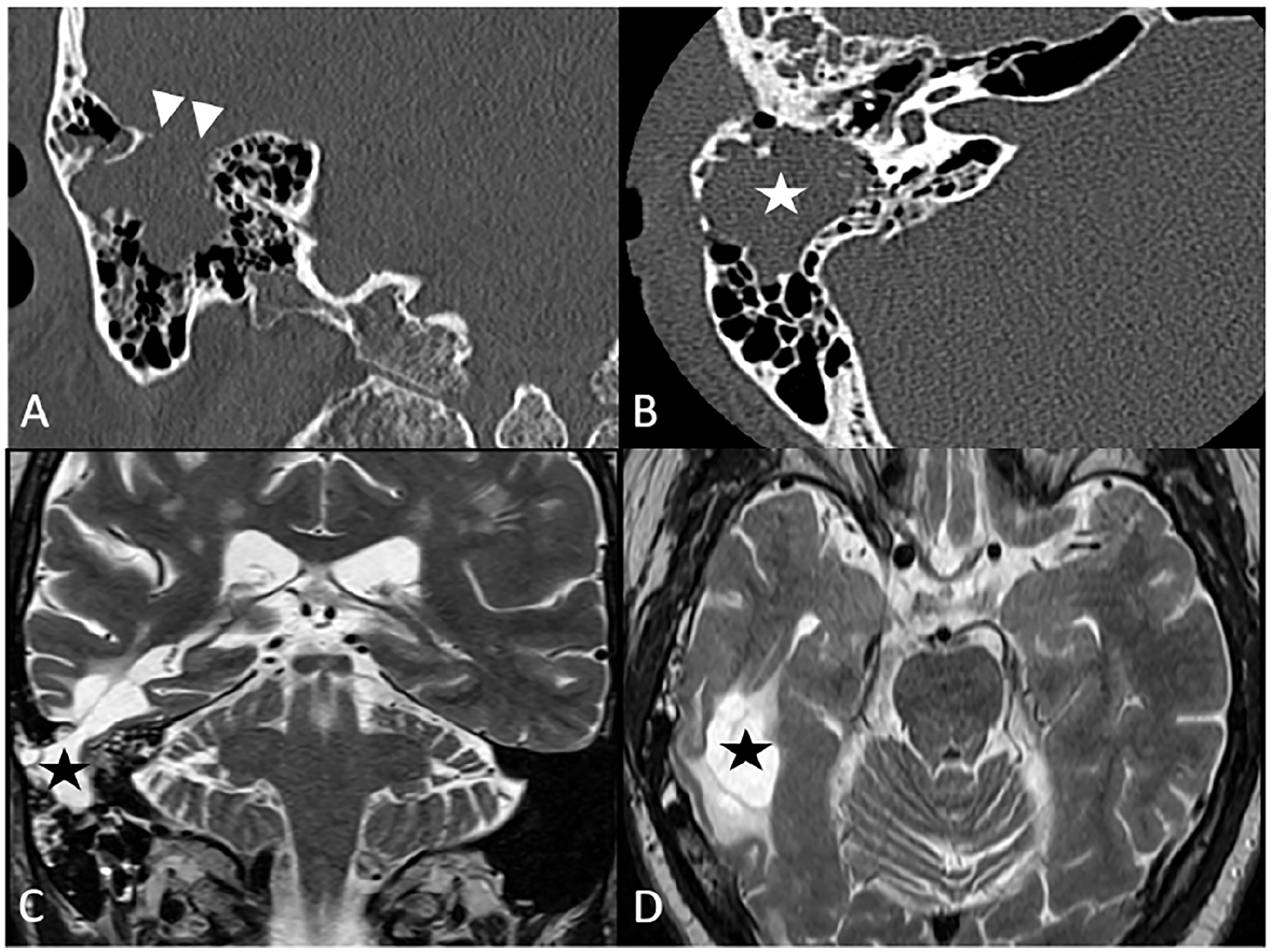
(A) Coronal CT demonstrates large tegmen defect (arrow heads); (B) axial CT shows partial mastoid opacification (white star); (C) coronal MRI T2 image reveals herniation of lateral ventricle into the mastoid (black star); (D) axial MRI T2 image illustrates significantly-dilated lateral ventricle (black star). CT, computed tomography; MRI, magnetic resonance imaging.
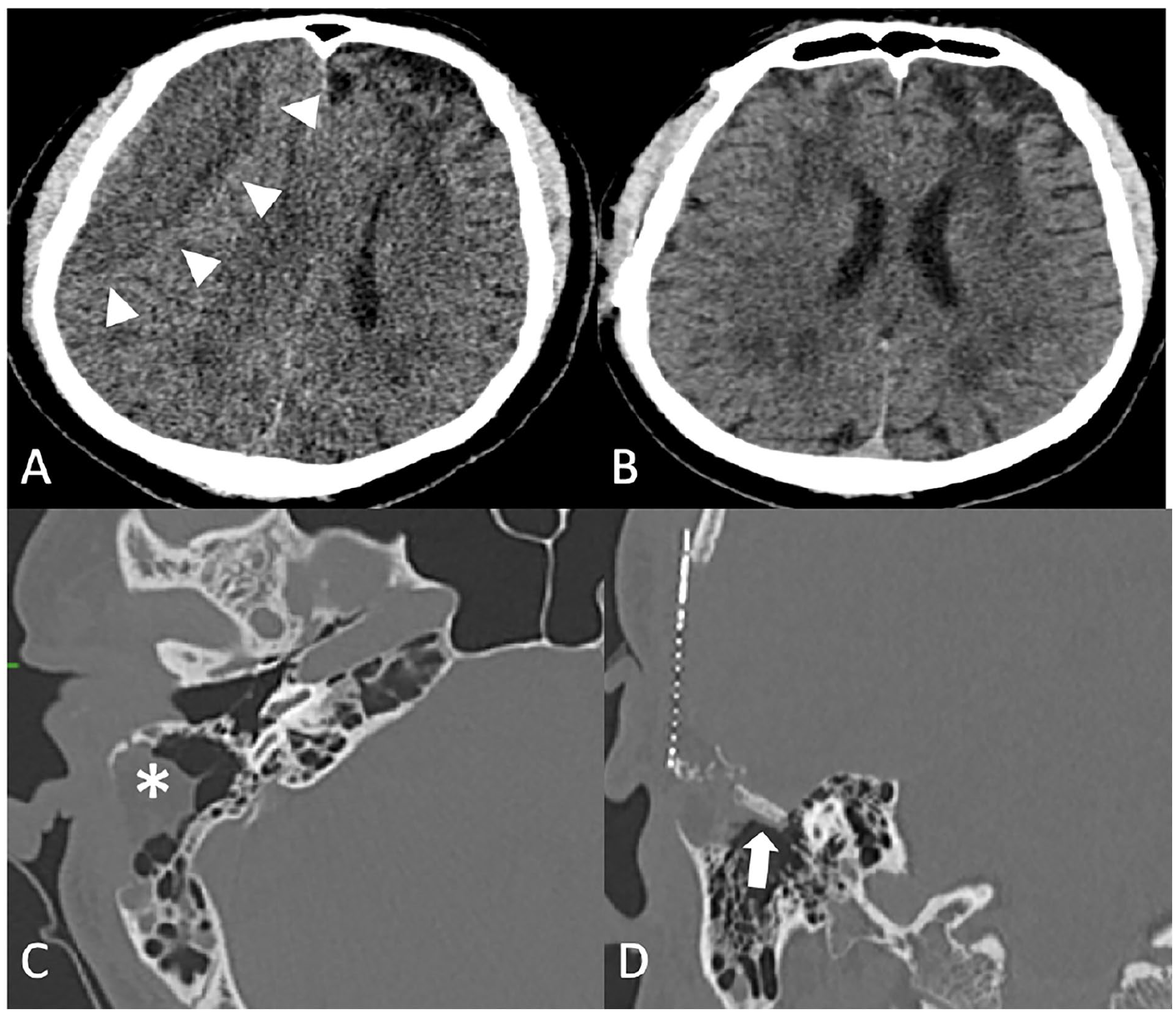
(A) Coronal CT shows a subacute subdural hematoma (arrow heads); (B) resolution of the SDH after bur hole procedure; (C) postoperatively fat graft (asterisk) in the mastoid cavity; (D) autologous bone graft (arrow) for repair at the tegmen. CT, computed tomography; SDH, subdural hematoma.
Discussion
This is a unique case of a patient who developed a delayed post-traumatic TBE with significant lateral ventricle herniation who then developed a subacute SDH. TBEs are a rare condition and cause of chronic otorrhea. A chart review from 1990 to 2000 of revision chronic ear surgery, found only 1% or 12 out of 1130 cases encephaloceles or CSF leaks. 6 Identifying TBEs can be challenging due to both their rarity and nonspecific symptoms including fullness, otorrhea, and hearing loss, making imaging critical for diagnosis.
Differential diagnoses of TBE include the following: chronic otitis media, cholesteatoma, cholesterol granuloma, facial nerve schwannoma, hemangioma, and mucocele and can be partially distinguished via imaging. High-resolution CT scans reveal dehiscence of the tegmen with complete or partial opacification of the mastoid air cells. MR images confirm the diagnosis of meningoencephaloceles by delineating tissue that is isointense to brain parenchyma and surrounded by CSF, which is hypointense on T1 and hyperintense on T2. Encephaloceles do not restrict on diffusion-weighted imaging images, which distinguish the lesion from cholesteatoma. Cholesterol granuloma can be distinguished by its hyperintensity on both T1 and T2 images. Both schwannoma and hemangioma are iso- to hypointense on non-contrast T1 images, contrast enhancing, and hyperintense on T2. Mucoceles have variable signal intensities on MRI.
A review of the existing literature identified a literature review with follow-up ranging from 2 to 48.7 months with complications including CSF leaks, abscess, sensorineural hearing loss, recurrent cholesteatomas, tympanic membrane perforations, meningitis, extradural hematoma, and temporary expressive aphasia. 3 Another retrospective chart review of 32 patients with CSF leaks and encephaloceles of temporal origin treated by a single neurosurgeon with follow-up ranging from 1 to 11 years had complications of reexploration of infected grafts as well as worse hearing but no reported subacute SDHs. 7 Similar to our patient history, a literature review of 267 patients with encephaloceles with epilepsy found that 262 (98.13%) of encephaloceles were located in the temporal lobe and that 13 (4.87%) presented with generalized tonic-clonic seizures. 8 Of note, not every patient in the review received surgical treatment for seizure management. In line with other patients with TBE, our patient underwent a combined mastoid-middle fossa approach. 9
To our knowledge, this is the first reported case of a TBE with lateral ventricle extending through the tegmen. Illustrated in this patient is the extent of cerebral herniation that can protrude into the mastoid. The herniation of the ventricle likely took place overtime and was responsible for the patient’s grand mal seizures.
Conclusions
This case alerts the skull base teams about the need for long-term follow-up especially in large skull base defects to monitor delayed occurrence of encephalocele and/or CSF leak. Surgical repair with the removal of devitalized brain tissue and multilayer closure is effective. However, fluid compartment shifts due to disturbances in the CSF flow pattern may result in the development of subacute SDH after successful repair and necessitates follow-up imaging. This is a single reported case of post-traumatic TBE, and there must be more research into the postoperative outcomes of TBE repair and identifying patterns of TBEs with associated imaging findings.
Footnotes
Author Note
Submission Statement: This is an original manuscript and has not been published elsewhere either in part or whole. Previous Presentations: No portion of the paper has been presented or published previously.
Ethical Considerations
Our institution does not require ethics approval for reporting individual cases or case series.
Author Contributions
Colyn White: preparation, creation, and/or presentation of the published work, specifically writing the initial draft (including substantive translation). Preparation, creation, and/or presentation of the published work by those from the original research group, specifically critical review, commentary, or revision including pre- or post-publication stages. Young Lee: preparation, creation, and/or presentation of the published work, specifically writing the initial draft (including substantive translation). Dr Maryam Rahman: ideas; formulation or evolution of overarching research goals and aims. Oversight and leadership responsibility for the research activity planning, including mentorship external to the core team. Dr Si Chen: ideas; formulation or evolution of overarching research goals and aims. Oversight and leadership responsibility for the research activity planning, including mentorship external to the core team.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.