
Abstract
Objective:
National Institute for Health and Care Excellence (NICE) no longer recommends offering systemic staging for early laryngeal cancer (T1N0 and T2N0). We aim to evaluate (1) whether guidance is being followed in our centre, (2) assess the impact on our patients and (3) perform a cost analysis.
Methods:
We retrospectively reviewed all laryngeal cases at a major Head and Neck cancer centre between January 01, 2020, and January 01, 2025. The following information was collected for all the patients: neck/systemic imaging modalities performed on patients, demographics, site of original laryngeal tumour and any metastatic disease detected by systemic imaging. We performed a cost analysis based on methods undertaken by NICE.
Results:
n = 83 patients had laryngeal cancer, n = 30 had T1N0 and T2N0 disease. Systemic imaging found no metastatic disease, n = 2 primary tumours and n = 1 lung infection. Systemic imaging cost £4207.12 and neck imaging cost £12 335.07.
Conclusions:
NICE guidance is not being followed at our centre, with limited benefits.
Introduction
Early (T1 and T2) laryngeal cancers have a low rate of locoregional and distant metastasis. 1 National Institute for Health and Care Excellence (NICE) guidelines were updated in 2016 and recommended to ‘Offer systemic imaging to all people with cancer of the upper aerodigestive tract [laryngeal cancer] except those with T1N0 and T2N0 disease’. 2 For T1 and T2 cancers of the larynx, systemic imaging was not deemed to be cost-effective. 3
This study aims to evaluate whether NICE guidance on the role of systemic imaging in the assessment and management of early laryngeal cancer is being followed in a major head and neck centre. The secondary aim is to assess the impact of this practice on the patient cohort and perform a cost analysis.
Materials and Methods
A retrospective review of cases was performed. The data gathered were part of a service evaluation project, which is exempt from ethics approval according to our institution. All data collected were anonymised, and patient consent was sought. Data were extracted for all patients who had larynx cancer between January 01, 2020, and January 01, 2025, following a search of the electronic patient management system. Patients who had T1N0 or T2N0 disease were analysed for further data collection. Following data collection, the total cost of the imaging used was analysed. Cost for each imaging modality was obtained using the ‘National Cost Collection: National Schedule of NHS costs—Year 2020-2021’. 4 The data were analysed using SPSS Statistics (Version 29 IBM). Fisher’s exact test, chi-square test and independent T test were applied, significance set at P < .05. All findings were reported to the Head and Neck MDT team, and clinician feedback was sought.
Results
Patient Population Results
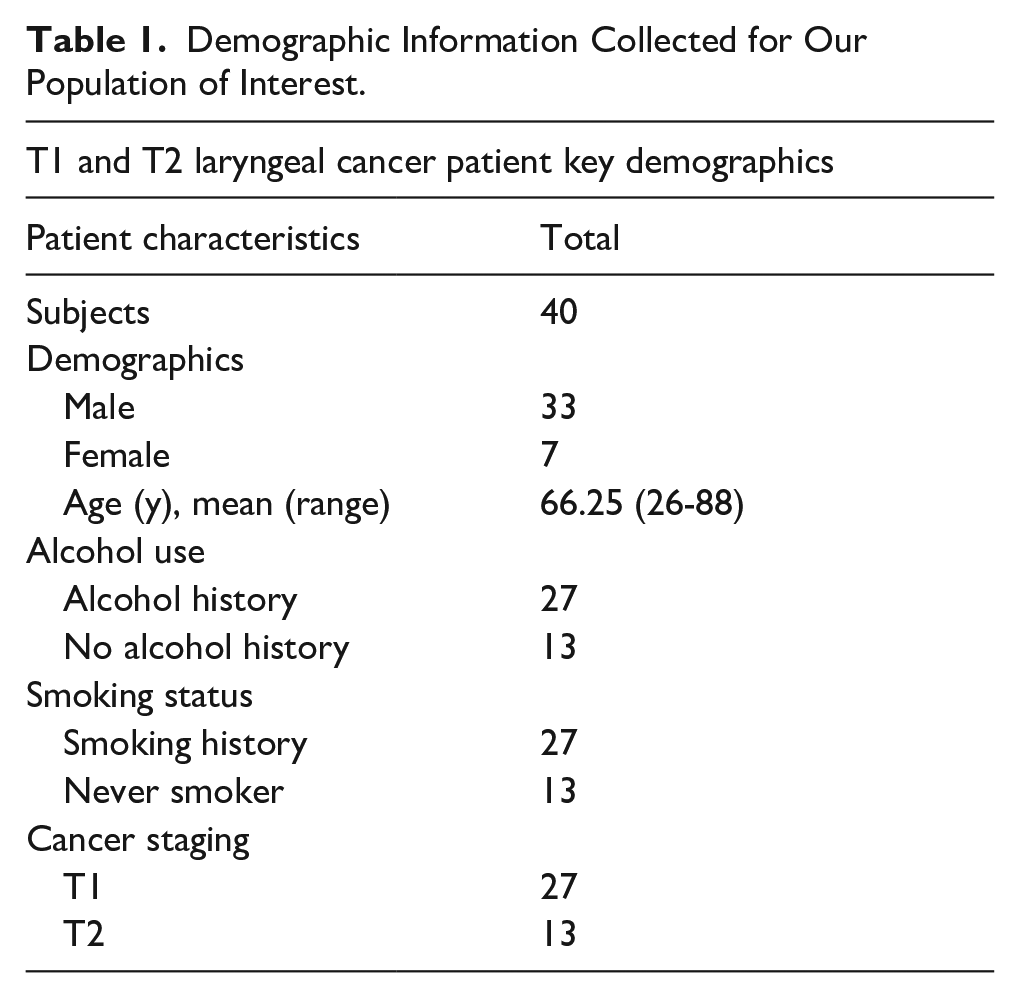
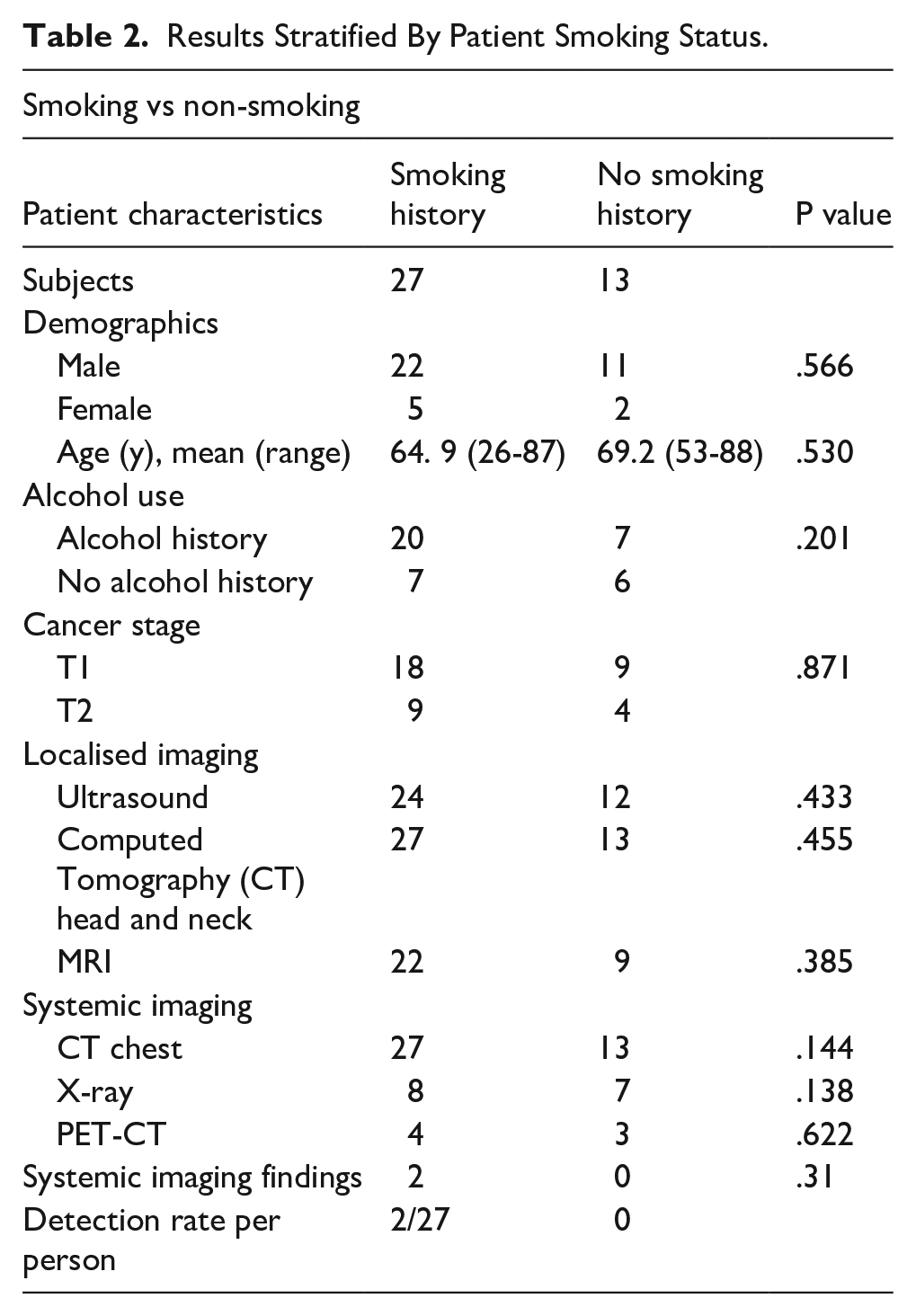
T1 and T2 laryngeal cancer was identified in n = 40 patients (Table 1). The population was male-dominated n = 33, and the mean age of the population was 66. Alcohol usage was prevalent in n = 27 reported current or previous alcohol use. Smoking was also prevalent; n = 27 reported current or previous smoking use. The population of interest contained a majority (n = 27) of T1 tumours and a minority (n = 13) of T2 tumours. Systemic imaging yielded n = 2 positive findings, with both patients having a smoking history. Smoking history was not significant (χ2 = 1.104, df = 1, P = .31, Fisher’s exact test, P = .55) for systemic imaging findings (Table 2). There was no significant difference in demographics and imaging between smoking and non-smoking patients, see Table 2 for P values.
Demographic Information Collected for Our Population of Interest.
Results Stratified By Patient Smoking Status.
Total Costing
The total cost for neck imaging was £15 670.57 and systemic imaging £5897.91, amounting to £21 568.48. The incremental cost of CT imaging of the chest was reported as part of systemic imaging.
Clinician Feedback
The primary reason for continued systemic imaging was the high smoking prevalence in the population, leading clinicians to view imaging for laryngeal cancer as an opportunity to screen for lung cancer. CT and chest X-rays were perceived as easy to organise.
Discussion
This study highlights a notable deviation from NICE guidelines at our centre, with many clinicians opting for a more cautious approach by performing systemic imaging on patients with T1N0 and T2N0 laryngeal cancers. Despite the lack of explicit recommendations for routine systemic imaging in early-stage disease, our findings indicate a clinical preference for comprehensive assessment, possibly influenced by patient-specific risk factors such as smoking history.
Of the 27 patients with a documented history of smoking, 24 underwent systemic imaging, with 2 cases revealing suspicious lesions. Further PET-CT imaging and biopsy confirmed both cases as T1 lung adenocarcinomas, and the patients subsequently received curative treatment via lobectomy. These findings suggest that systemic imaging may be justified in selected patients, particularly in populations with high smoking prevalence, due to its potential to detect secondary primary tumours (SPTs) at an early and treatable stage.
Interestingly, statistical analysis did not identify smoking as a significant independent risk factor for the presence of SPTs. Nevertheless, all patients in our cohort underwent at least 1 form of systemic imaging—CT chest being the minimum standard—regardless of smoking status. The decision to image all patients appears to be influenced by the overall high prevalence of smoking (58%) in our cohort, markedly higher than the national average of 13% in England.
The 2016 NICE review concluded that systemic imaging, particularly PET-CT, was not cost-effective for early-stage laryngeal cancer due to the low incidence of distant metastases. However, this assessment did not consider the potential benefits of detecting SPTs, nor the long-term cost savings and clinical advantages of early intervention. The data from our study support the notion that imaging may offer significant benefits in high-risk populations, particularly given the strong association between laryngeal cancer and SPTs, especially in the lungs, as reported by multiple studies post-2016.5-7
Further evidence from the literature supports this concern. Yurday et al reported significantly poorer overall survival among patients with laryngeal cancer and SPTs, with lung cancer accounting for 61.5% of related deaths. 8 Head and neck cancers are associated with SPT, and most commonly with SPT in the lung. 9 Additionally, untreated Stage I non-small-cell lung cancer (NSCLC) has a 5-year survival rate of only 6%, compared to 9% for T1 tumours. 10 The financial burden of treating advanced NSCLC (~£25 000) greatly exceeds the estimated cost of systemic imaging over 5 years at our centre (£5897.91), underscoring the potential cost-effectiveness of early detection. 11
A key strength of this study is its demographic similarity to the cohort examined in the National Head and Neck Cancer Audit, which underpinned the 2016 NICE guidelines. This enhances the relevance of our findings to UK clinical practice. However, several limitations must be acknowledged. The retrospective, single-centre design restricts generalisability and limits statistical power. The absence of a uniform imaging protocol further undermines the reliability of SPT detection rates. Moreover, confounding variables such as prior malignancies, comorbidities, symptomatology and patient age were not controlled for, primarily due to limited sample size and retrospective data collection.
Conclusion
This study underscores the potential clinical value of systemic imaging in early-stage laryngeal cancer, particularly in populations with a high prevalence of smoking. While our findings support a more cautious imaging approach, we recognise that our study design does not provide sufficient evidence to formally challenge current NICE guidelines. We advocate for larger, multicentre prospective studies to better evaluate the diagnostic and economic implications of systemic imaging in this patient group and to inform future guideline development (Figure 1).
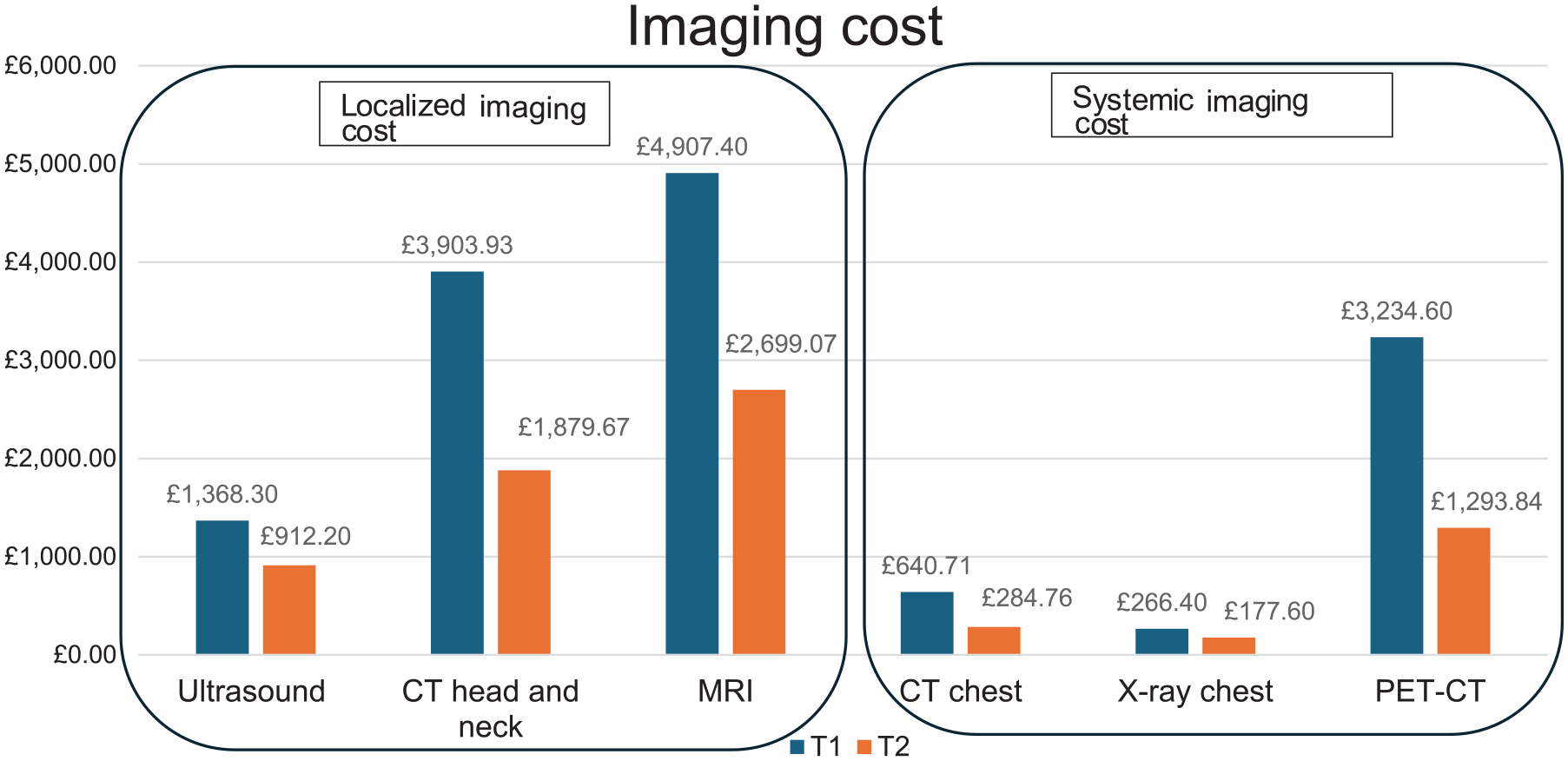
Cost of imaging modalities.
Footnotes
Acknowledgements
We would like to thank the head and neck team at University College London Health Trust for their support.
Author Note
This paper was presented at the Irish Head and Neck Conference in 2023.
Ethical Considerations
Ethics approval was not required as the data gathered was part of a service evaluation project, which is exempt from approval according to our institution. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Consent to Participate
Informed consent was obtained from all patients for this study.
Author Contributions
PAT contributed to the concepts, design, definition of intellectual content, literature search, data acquisition, data analysis, statistical analysis, manuscript preparation, manuscript editing and manuscript review. SK contributed to the data acquisition and manuscript review. PS contributed to the concepts, design, manuscript editing and manuscript review.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data Availability Statement
All data generated or analysed during this study are included in this published article.