
Abstract
Chronic otitis media is a persistent middle ear infection caused by various well-described bacteria that, in rare cases, can lead to severe complications including intracranial infections such as brain abscesses and meningitis. We present a case of a 42-year-old female with a complicated medical history including chronic otitis media, who developed a brain abscess and meningitis following the spread of the infection. The patient initially presented with altered mental status and concerns for acute intracranial processes were confounded by her significant polysubstance use history. Further work up revealed bacteremia. Imaging revealed middle ear effusions with skull base dehiscence and a large brain abscess in the temporal lobe. Workup revealed a diagnosis of viral and bacterial meningitis via blood, and CSF cultures from both cerebrospinal fluid and ear discharge confirmed the presence of Streptococcus pneumoniae with Epstein–Barr Virus (EBV) DNA in the CSF. The patient was treated with intravenous antibiotics, surgical drainage of the abscess, and supportive care, leading to clinical improvement and eventual discharge from the hospital against medical advice. This case highlights the potential for chronic otitis media to result in life-threatening intracranial infections, underscoring the importance of early detection, high clinical suspicion despite patient confounding medical factors, and aggressive management in cases of advanced disease.
Introduction
Chronic otitis media (COM) is an infection or inflammation of the middle ear that is long-standing, usually lasting on the order of several weeks to months, characterized by persistent middle ear effusions which can lead to recurrent ear infections, damage to middle ear structures, and hearing loss. The etiology of this process, although many times multifactorial in nature, can be driven by various factors, including previous ear infections and middle ear anatomical and physiological changes, eustachian tube dysfunction, or chronic allergies, for example. The vast majority of COM can be treated on an outpatient basis with nasal sprays, antihistamines, antibiotics, or even minimally invasive procedures such as myringotomy tubes or eustachian tube dilation. If inadequately managed, this process can lead to more severe complications such as spread of infection to the intracranial space, resulting in osteomyelitis, empyema, or intracranial abscess. 1
Infection is commonly caused by Staphylococcus aureus and Pseudomonas aeruginosa, but many bacteria have been documented in this disease’s pathogenesis. Some pathogens form a biofilm, which shields the bacteria from host immune response allowing evasion and increasing the risk of persistence and progression. Less commonly, Streptococcus pneumoniae may be implicated as was observed the patient described in this case.2,3 While usually implicated in acute infection, its role in chronic infection with intracranial complications highlights the potential for atypical pathogens to exhibit virulence in vulnerable populations.
Case History
This article presents the case of a 42-year-old female with a complex medical and social history including a history of homelessness and polysubstance abuse, multiple sclerosis, anxiety disorder with borderline personality disorder, and a reported history of central nervous system malignancy who was found down for an unknown amount of time in an abandoned home with a nondocumented last known normal by Emergency Medical Services. Upon arrival to the Emergency Department, the patient was noted to be actively seizing with decorticate posturing. The patient was intubated for low mental status and airway protection in the setting of a Glasgow Coma Score of 6 and admitted to the Medical Intensive Care Unit (MICU).
Her initial work up, including computed tomography (CT) scan of her head, demonstrated generalized parenchymal edema suspicious for anoxic brain injury, a chest X-ray with right upper/mid-lung patchy opacities that may have represented either pneumonia, aspiration, or atelectasis, and blood cultures positive for S. pneumoniae bacteremia. Her white blood cell count was 35 and she had persistently elevated fevers. The patient was started on empiric broad-spectrum antibiotics with ampicillin/sulbactam and linezolid. It is important to note that the patient’s alerted mental status work up was seemingly directed at evaluation of many of her significant medical commodities such as history of intravenous drug use, seizures, and episodes of acute hypoxic respiratory failure. This is a key understanding as, at this time, middle ear pathology was of very low suspicion for the emergency and critical care medical teams for causative etiology. This is presumably why the Ear, Nose, and Throat service was not engaged despite findings on initial CT head suggestive of a focal dehiscence of the left tegmen tympani and tegmen mastoideum with possible small and chronic left mastoid effusion. These are findings that would eventually be germane to the patient’s diagnosis and management. In critically ill, medically complex patients, all diagnostic avenues must be exhausted in a multidisciplinary manner, and specialty services such as Ear, Nose, and Throat offer unique perspectives that can yield answers to complicated questions.
Because of the concern for mental status and central nervous system depression in the setting of strep pneumoniae bacteremia, a lumbar puncture was obtained which demonstrated polymorphonuclear neutrophils (PMNs), high protein count, and low glucose. The results were positive for Epstein–Barr Virus DNA (EBV) and S. pneumoniae. At this time, her IV antibiotics were also switched to empiric meningitis coverage with vancomycin and ceftriaxone.
Several days later, with clinical nonimprovement with antibiotics and medical care, the otolaryngology service was consulted for evaluation of temporal bone changes identified on the patient’s CT head and facial imaging with temporal bone sequences demonstrating focal dehiscence of the left tegmen tympani and tegmen mastoideum (Figure 1). There were also concerns for chronic mastoid effusion and a small encephalocele on a previous magnetic resonance imaging (MRI) (Figure 2). Unfortunately, the patient’s history and exam were limited by the patient’s altered mental status and variable agitation/combativeness and high levels of sedation for patient safety and ventilatory compliance. There was no drainage from the bilateral external auditory canals (EACs), but there was a cerumen impaction in the left ear obscuring view of the tympanic membrane (TM). The right EAC and TM were within normal limits as were the mastoid regions to inspection and palpation. Fiberoptic flexible nasopharyngolaryngoscopy revealed normal nasal and nasopharyngeal mucosal surfaces including normal eustachian tube orifices bilaterally without drainage or purulence. The left ear was minimally debrided at bedside, but patient tolerability led to abortion of procedure.
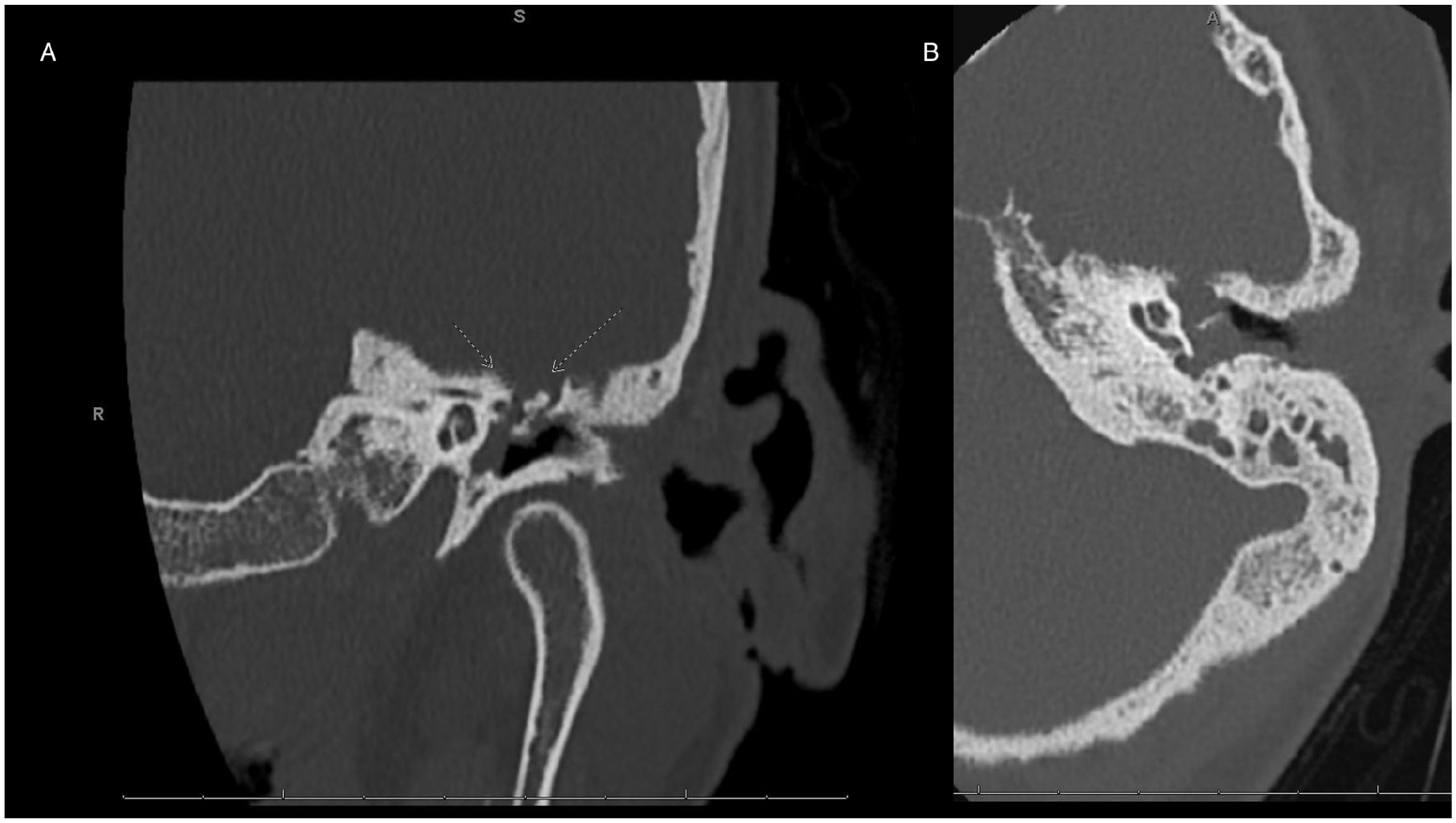
Noncontrasted CT temporal bone images demonstrating tegmen dehiscence and mastoid effusion in the coronal (A) and axial (B) planes. CT, computed tomography.
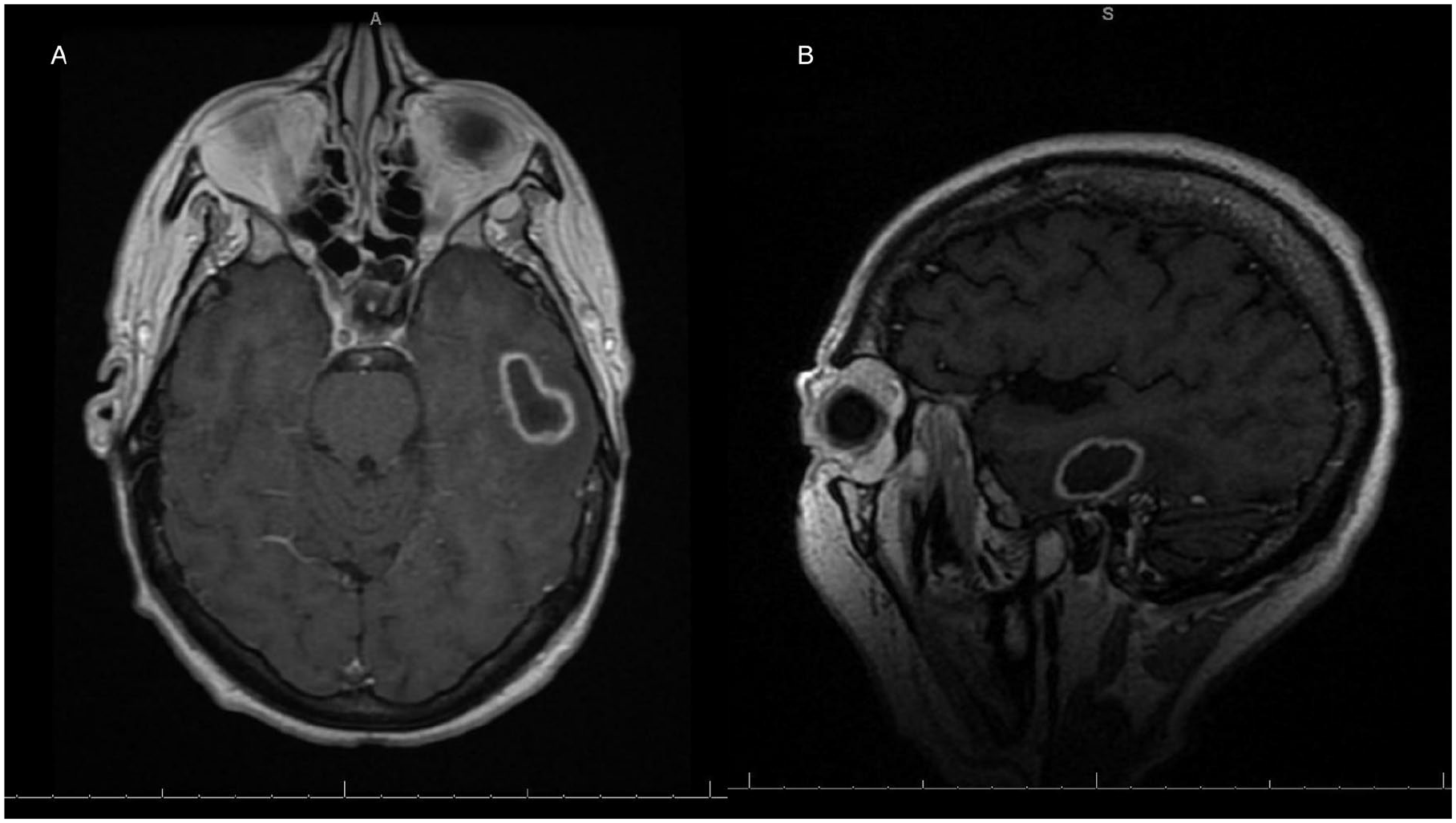
Contrasted enhanced T-1 weighted MRI images demonstrating left temporal lobe abscess in the axial (A) and sagittal (B) planes. MRI, magnetic resonance imaging.
MRI was used to image the brain and demonstrated an intraparenchymal pyogenic abscess along the inferior aspect of the left temporal lobe measuring 1.9 × 2.2 × 2.6 cm contiguous with dehiscence of the tegmen tympani/tegmen mastoideum associated with the chronic mastoid effusion with findings consistent with ventriculitis and infectious meningitis (Figure 2).
The patient was taken to the operating room the following day for a left-sided mastoidectomy, myringotomy with t-tube placement, evacuation of intracranial abscess, and drain placement with otolaryngology and neurosurgery. This procedure yielded expected findings of diffusely inflamed mastoid cavity without cholesteatoma with dehiscence along the tegmen with purulent drainage from the dehiscent tegmen tympani. At no point did cultures from the ear, mastoid, or intracranial abscess grow any bacteria. Patient microbiological evaluations are present in Table 1.
Patient’s Microbiological Work Up and Respective Results During Hospitalization.
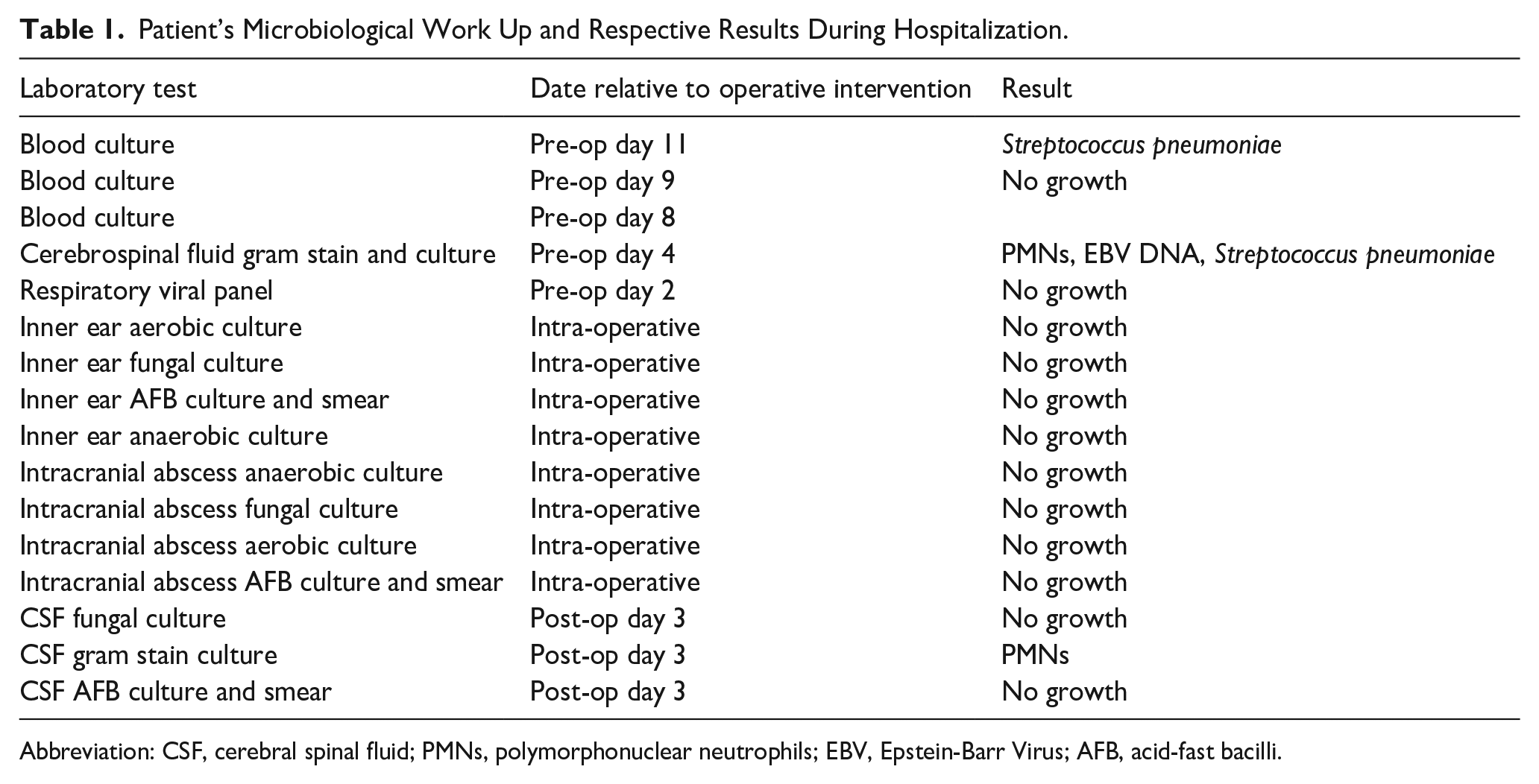
Abbreviation: CSF, cerebral spinal fluid; PMNs, polymorphonuclear neutrophils; EBV, Epstein-Barr Virus; AFB, acid-fast bacilli.
On postoperative day one, the patient developed concern for a possible cerebral spinal fluid (CSF) leak as demonstrated by clear fluid persistently leaking from her left ear and collecting in the conchal bowl. Consequentially, neurosurgery placed a lumbar drain and removed the craniotomy drain, otolaryngology removed the t-tube and performed fat graft myringoplasty. The fluid was collected and sent for beta-2-transferrin testing and was negative which lowered the suspicion for a CSF leak.
Postsurgical CT imaging was overall nonrevealing of acute processes and demonstrated removal of left temporal approach surgical drain and evolving postoperative changes of prior parenchymal abscess evacuation.
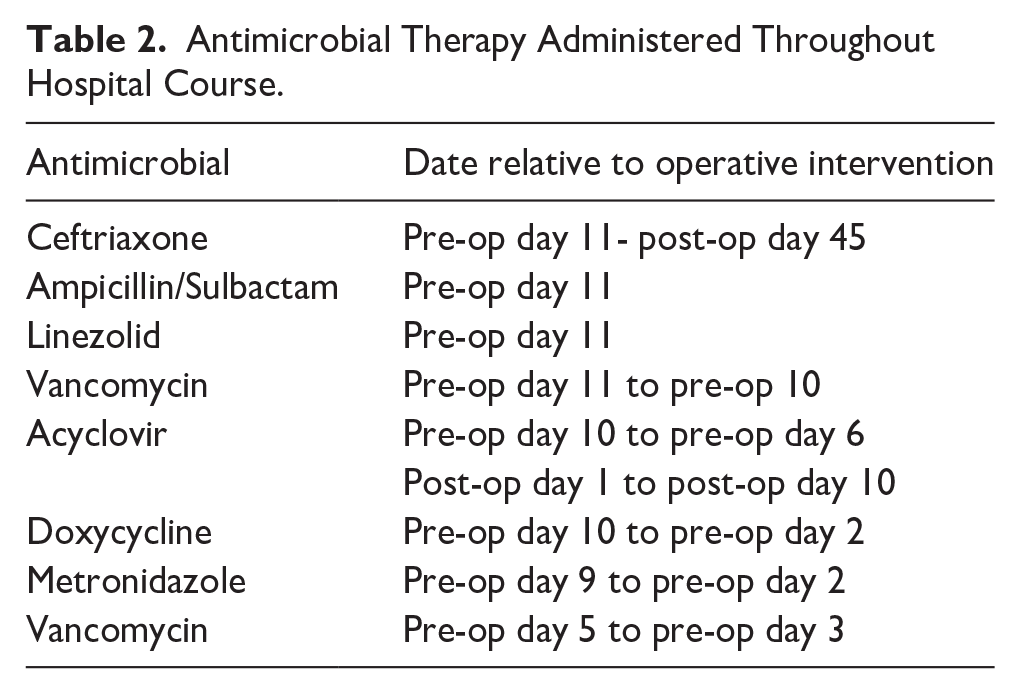
The Infectious Disease team, who had been following the patient and adjusting her antimicrobial regimen regularly based on evolving data, recommended 8 weeks of ceftriaxone and acyclovir for treatment of her meningitis. Her full antimicrobial course can be seen in Table 2. She was ultimately discharged against medical advice six weeks after her surgery and was lost to follow-up in part secondarily to her complicated socioeconomic status and multifaceted medical and substance dependence history.
Antimicrobial Therapy Administered Throughout Hospital Course.
Discussion
For nonprogressive cases of COM, outpatient management is aimed at stopping disease progression and preventing complications. Oral antibiotics are indicated for refractory or worsening cases and treatment should be guided by culture results. Common pathogens implicated in COM include Pseudomonas and Staphylococcus aureus, and less commonly Proteus mirabilis, Escherichia coli, and Enterococcus faecalis. Empiric treatment should cover both Pseudomonas and Methicillin-resistant Staphylococcus aureus (MRSA) due to their high prevalence in chronic and complicated cases. 4 Further, Pseudomonas is highly resistant to Ciprofloxacin and Levofloxacin. S. aureus displays some resistance to Ciprofloxacin, though to a lesser extent and occasionally displays methicillin resistance. P. mirabilis has also been shown to have some resistance to Ciprofloxacin with one study isolating a strain producing extended-spectrum beta-lactamase.5,6 Timely intervention can help prevent the spread of infection to adjacent structures and reduce the risk of progression to more severe disease.
Despite appropriate treatment, COM can progress to life-threatening complications including mastoiditis, skull base osteomyelitis, meningitis, and brain abscess. These complications often occur through direct extension of infection from the middle ear to the mastoid and surrounding structures leading to intracranial destruction. Diabetes mellitus is a major risk factor for skull base osteomyelitis given its implications in microangiopathy and altered immune response which facilitates tissue invasion. Other risk factors include hypertension, ischemic heart disease, and immunosuppression which delays healing and increases susceptibility to complications. 7
Skull base osteomyelitis (SBO) is a severe complication of chronic otitis media, characterized by the extension of infection to the temporal, sphenoid, or occipital bone with potential involvement of adjacent structures and cranial nerves. Symptoms include headache, otorrhea, otalgia, and cranial nerve deficits. 8 Diagnosing SBO can sometimes be difficult due to the nonspecific and insidious presentation which leads to delayed recognition and management. This point is particularly important to note in our patient given her medical history and presumed substance use or primary neurologic etiology for decompensation and mental status changes.
Once progression to skull base osteomyelitis has occurred, management typically involves surgical intervention (if evidence of intracranial pathology) and prolonged intravenous antibiotics through a peripherally inserted central catheter (PICC) line. First-line antibiotic therapy includes fluoroquinolones, third-generation cephalosporins, aminoglycosides, carbapenems, and vancomycin, and therapy typically lasts 6 to 20 weeks with a minimum of 3 months of therapy being the general protocol. 8 Duration of antibiotic treatment depends on a multitude of factors including susceptibility of the pathogen to antibiotic therapy and spread of infection past the middle ear which may warrant prolonged therapy. Blood and tissue cultures guide antimicrobial therapy, and persistent or worsening cases may warrant biopsy to identify atypical pathogens. Fungal pathogens such as Aspergillus or Scedosporium may be implicated in some cases of skull base osteomyelitis, particularly in immunocompromised patients or those with refractory infections. In individuals who fail to improve with the standard 3 month regiment, antibiotics can be continued for 4 to 6 months to treat chronic osteomyelitis. 9 A prior case reported persistent infection with Scedosporium apiospermum after both oral and IV antibiotics, which resolved with voriconazole. 10 Another case reported successful management of SBO with 6 weeks of IV levofloxacin after multiple courses of oral antibiotics failed. 11 Surgical intervention is indicated for abscess drainage, necrotic tissue debridement, refractory cases, or cholesteatoma removal to prevent recurrence. Further, cases with facial nerve involvement warrant surgical intervention to avoid neurological complications.
This case highlights the importance of early detection, aggressive management, and tailored therapy to prevent progression to life-threatening complications associated with COM. Favorable prognosis is achieved with timely diagnosis and intervention, but delayed or resistant treatment leads to high-risk cases with poor outcomes. Long-term follow-up with imaging is essential to monitor treatment response and prevent recurrence.
Conclusion
The case presented highlights an infrequent but severe complication of chronic otitis media leading to skull base dehiscence, development of an intracranial abscess, and bacterial meningitis with concurrent EBV infection. The patient’s course defined by combination of surgical intervention for source control, antibiotic therapy, and appropriate management of surgical and infectious sequelae emphasizes the importance of timely diagnosis and aggressive management in such unique cases of progressive infections. The presence of both viral and bacterial infections, as well as the patient’s multifactorial altered presentation complicated the clinical picture, emphasizing the need for a multidisciplinary approach to such cases. Overall, early recognition, multidisciplinary medical management, and prompt treatment are crucial in improving patient outcomes and preventing long-term neurological sequelae of complicated cases of chronic otitis media and its sequelae.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to Participate
Informed consent for information published in this article was not obtained given the patient’s lack of follow-up and inability to reach the patient. All reasonable steps have been taken to protect patient identify. There is no identifying information presented in this case report.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The participants of this study did not give written consent for their data to be shared publicly, so due to the sensitive nature of the research supporting data are not available.