
Abstract
Subcutaneous emphysema following nasal surgery is a rare yet potentially severe complication. This case report describes a 40-year-old woman who developed extensive subcutaneous emphysema involving the face, neck, mediastinum, and thorax after uneventful turbinate cauterization and nostril reduction. The patient, with a history of prior septoplasty and rhinoplasty, presented with nasal obstruction and underwent the procedure under general anesthesia. Postoperatively, she developed progressive neck swelling, which rapidly extended to cervicofacial, mediastinal, and thoracic regions. Imaging via noncontrast computed tomography (CT) confirmed widespread air infiltration, while fiberoptic laryngoscopy and bronchoscopy ruled out aerodigestive injuries. Multidisciplinary management included mediastinal drainage, leading to dramatic symptom resolution. The mechanism likely involved inadvertent mucosal perforation during thermal ablation, creating a one-way valve effect that permitted air ingress during Valsalva maneuvers. This case underscores the anatomical continuity between cervical and mediastinal fascial planes, enabling rapid air dissemination. Key lessons include the importance of early imaging for atypical postoperative swelling, judicious use of thermal energy during turbinate procedures to minimize mucosal injury, and patient counseling to avoid forceful maneuvers post-surgery. Despite an uncomplicated intraoperative course, occult tissue defects can precipitate life-threatening complications, necessitating prompt intervention. Surgeons should maintain a high index of suspicion for subcutaneous emphysema in nasal surgeries, particularly when employing thermal techniques, and prioritize multidisciplinary collaboration to optimize outcomes. This report highlights the critical balance between procedural efficacy and safety in preventing rare but consequential complications.
Keywords
Introduction
Subcutaneous emphysema, characterized by the infiltration of air into fascial planes and subcutaneous tissues, is a well-documented but rare complication following surgical procedures involving the head and neck. 1 While most cases arise from traumatic or iatrogenic causes, such as maxillofacial surgery or endotracheal intubation, its occurrence after routine nasal surgeries, including septoplasty or rhinoplasty, remains exceedingly uncommon.2,3 Notably, subcutaneous emphysema extending to the mediastinum and thorax poses significant clinical challenges due to the risk of respiratory compromise and delayed diagnosis. 4 The majority of reported cases following nasal surgery are associated with turbinate reduction techniques, such as radiofrequency ablation or electrocautery, which may inadvertently create mucosal defects allowing air entry into deeper tissues.3,5 However, the progression of emphysema to involve the neck, mediastinum, and thoracic regions—as observed in this case—is exceptionally rare, with only sparse documentation in the literature.4,6 Such extensive spread underscores the potential for occult tissue injury during seemingly uncomplicated procedures and highlights the need for heightened clinical suspicion in postoperative settings.
This case report describes a severe and unusually extensive subcutaneous emphysema involving the face, neck, mediastinum, and thorax following turbinate cauterization and nostril reduction, despite an uneventful surgical course. By integrating imaging findings and procedural insights, this report aims to emphasize the importance of early recognition, multidisciplinary management, and preventive strategies to mitigate risks associated with nasal surgeries.
Case Presentation
A 40-year-old woman presented with nasal obstruction without accompanying nasal discharge, headache, or hyposmia. Regarding her medical history, she underwent a septoplasty one and a half years ago and a rhinoplasty a year ago, both of which were completed without any complications related to anesthesia or post-anesthesia resuscitation. On examination, hypertrophy of the inferior turbinates was observed. The treatment involved turbinate cauterization combined with nostril reduction, performed under general anesthesia. The procedure lasted approximately thirty minutes and was completed without any surgical complications. However, in the postoperative period, she developed neck swelling. Physical assessment showed subcutaneous emphysema extending into the neck and upper thoracic regions, without dyspnea or hypoxia. In the following days, the emphysema extended to include the lower thoracic area, as well as the neck and facial regions. Fiberoptic laryngoscopy showed normal laryngeal structures, and direct bronchoscopy revealed no abnormalities (Figure 1). Noncontrast axial and coronal CT scans of the head, neck, and thorax demonstrate extensive emphysema involving the face, neck spaces, mediastinum, upper and lower thoracic regions, and subcutaneous tissues (Figure 2). The patient underwent mediastinal drainage by a thoracic surgeon, during which methylene blue was administered, revealing no esophageal injury. Symptoms improved dramatically following the intervention (Figure 3), and the subcutaneous emphysema gradually subsided. The patient was subsequently discharged with complete resolution of the symptoms.
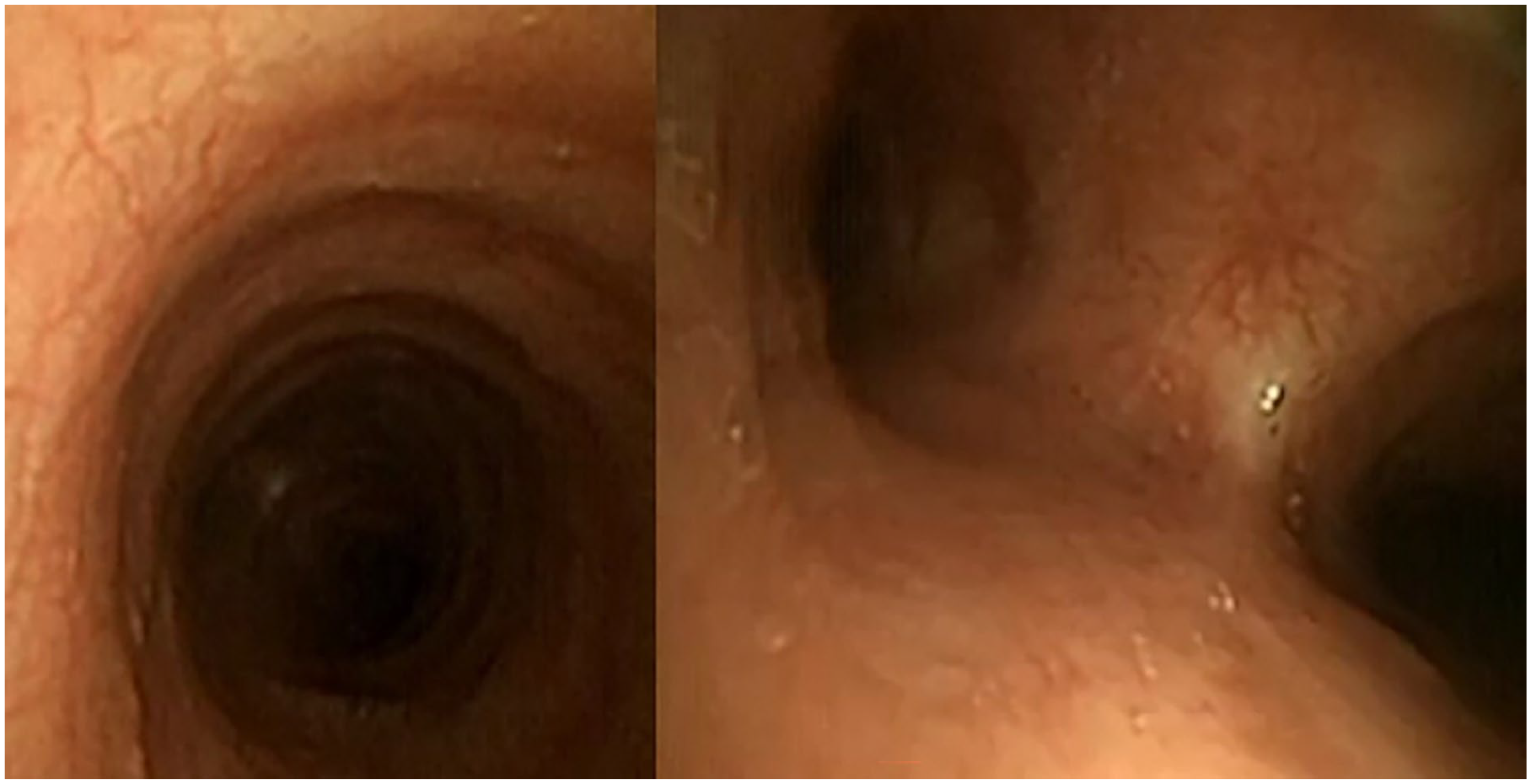
Direct bronchoscopy revealed no abnormalities.
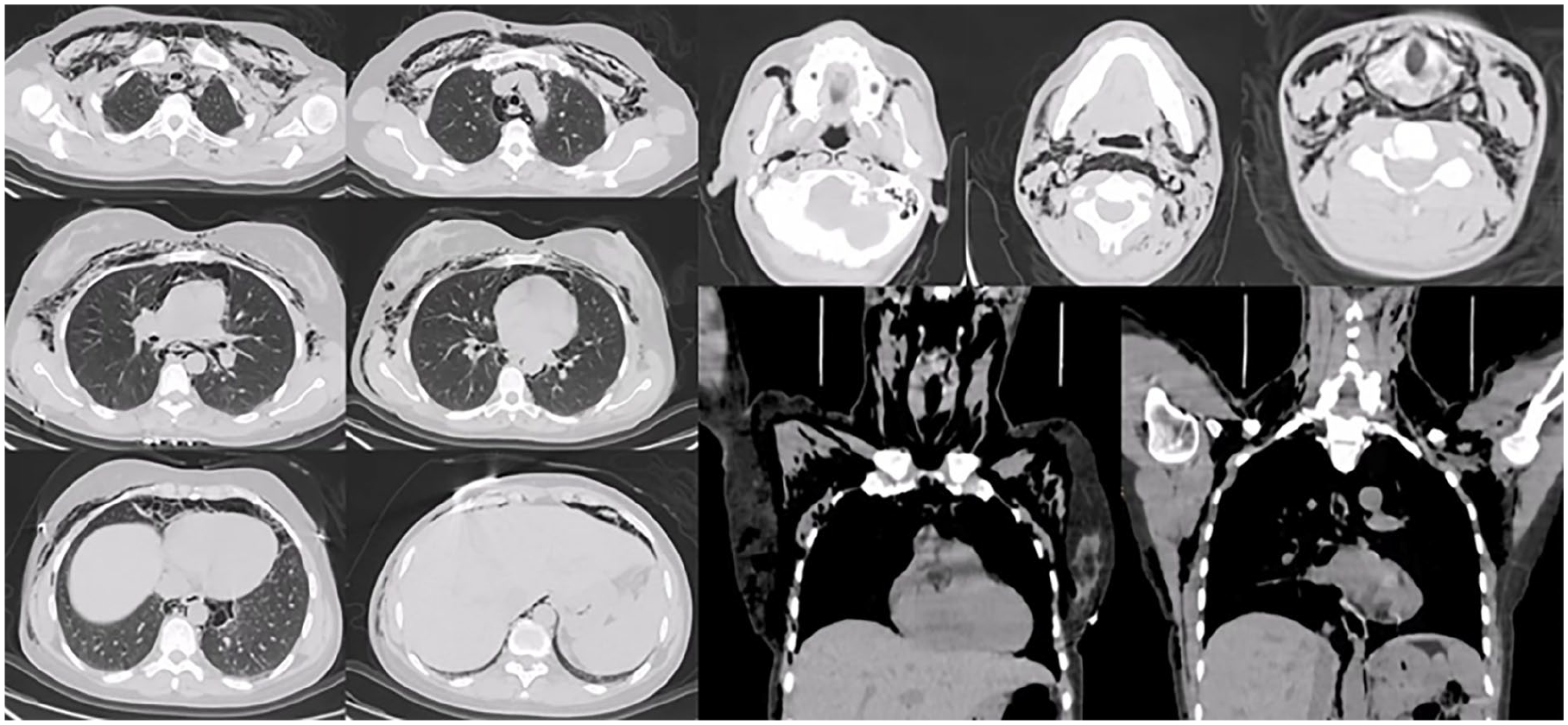
Noncontrast axial and coronal CT scans of the head, neck, and thorax demonstrate extensive emphysema involving the face, neck spaces, mediastinum, upper and lower thoracic regions, and subcutaneous tissues.

Before and after mediastinal drainage.
Discussion
Subcutaneous emphysema following nasal surgery, though rare, underscores the critical interplay between surgical technique, anatomical vulnerability, and postoperative complications. In this case, the extensive spread of emphysema to the neck, mediastinum, and thorax highlights the potential for occult tissue injury during seemingly routine procedures, such as turbinate cauterization and nostril reduction. The mechanism likely involved inadvertent mucosal perforation during thermal ablation, creating a one-way valve effect that allowed pressurized air from nasal Valsalva maneuvers (eg, coughing, sneezing) to infiltrate fascial planes.1,2 Similar pathways have been described in cases of septoplasty and rhinoplasty, where disruption of mucosal integrity permits air migration into deep cervical and mediastinal spaces.2,4 Notably, the absence of intraoperative complications in this patient emphasizes the subtlety of such injuries, which may only manifest postoperatively with delayed symptom progression.
The rapid extension of emphysema to the mediastinum and thorax aligns with the anatomical continuity between cervical and mediastinal fascial compartments. Air can track along the retropharyngeal and prevertebral spaces into the mediastinum, facilitated by negative intrathoracic pressure during respiration. 4 This case mirrors reports in literature, where high-pressure air entry through mucosal defects led to widespread emphysema. 6 The absence of esophageal injury, confirmed via methylene blue administration during mediastinal drainage, further supports an iatrogenic nasal origin rather than aerodigestive tract perforation. The management of extensive emphysema remains contentious. Conservative approaches, including antibiotics, cough suppression, and restricted oral intake, are often sufficient for localized cases.2,6 However, mediastinal involvement necessitates prompt intervention to avert life-threatening complications such as mediastinitis or tension pneumothorax. 4
While in the case reported by Al Jaber et al, a conservative management strategy was employed following pneumomediastinum and subcutaneous emphysema after septorhinoplasty. This approach included oxygen therapy, continuous surveillance of vital signs and respiratory status, pain control, and careful monitoring on potential symptoms of respiratory distress. The conservative treatment proved effective, leading to clinical improvement and gradual resolution of the complications. 7 In this patient, mediastinal drainage proved pivotal in decompressing air collections, paralleling strategies described in thoracic trauma cases. 4 The dramatic symptom resolution post-drainage underscores the importance of multidisciplinary collaboration, particularly with thoracic surgery, when emphysema extends beyond cervicofacial regions. Preventive measures are paramount. Turbinate procedures, including radiofrequency ablation, carry inherent risks of mucosal injury due to thermal spread or excessive tissue resection. 8 Technical modifications, such as limiting energy delivery depth and avoiding aggressive tissue manipulation near the nasopharynx, may mitigate these risks. Additionally, postoperative patient education to avoid Valsalva maneuvers could reduce air ingress through latent defects.2,4 Intraoperative vigilance for mucosal breaches, coupled with immediate repair using autologous grafts (eg, cartilage or fascia), may further prevent air leakage.2,4 This case also invites comparison to subcutaneous emphysema following other otolaryngologic procedures, such as tonsillectomy or canalplasty.2,4 While the etiologies differ, the unifying theme is the inadvertent creation of tissue defects that permit air entry. For instance, one of the reports emphysema due to pharyngeal constrictor muscle injury during tonsillectomy, whereas other describes temporomandibular joint (TMJ) capsule exposure during canalplasty.2,4 Such parallels reinforce the need for meticulous tissue handling across all head and neck surgeries. The extensive subcutaneous emphysema observed here underscores the need for procedural refinement in turbinate surgery. While radiofrequency and electrocautery are effective for turbinate reduction, their thermal effects may increase mucosal fragility, predisposing to microperforations during concurrent procedures like nostril narrowing.3,5 Preoperative assessment of mucosal integrity, particularly in revision cases, could mitigate such risks by identifying atrophic or scarred regions prone to iatrogenic injury. 9 Additionally, adopting minimally invasive techniques, such as ultrasound-guided turbinate reduction—which demonstrates comparable efficacy with lower mucosal trauma—may reduce air dissection potential. 5 Postoperative protocols emphasizing avoidance of positive-pressure maneuvers (eg, nose-blowing) and early imaging for atypical swelling remain critical to prevent delayed ccomplication. 4 Finally, imaging remains indispensable for diagnosis and monitoring. CT scans, as utilized here, excel in delineating air distribution and guiding intervention.4,6 However, clinicians must balance radiation exposure with clinical urgency, particularly in younger patients. Fiberoptic laryngoscopy and bronchoscopy, performed here to exclude laryngotracheal injury, are also critical adjuncts to rule out alternative etiologies. 6
This case exemplifies the unpredictable nature of subcutaneous emphysema following nasal surgery. Early recognition, tailored imaging, and timely intervention—supported by a multidisciplinary framework—are essential to optimize outcomes. Surgeons must remain vigilant to anatomical vulnerabilities and adopt preventive strategies to minimize this rare but consequential complication.
Conclusion
This case illustrates that even routine nasal procedures—such as turbinate cauterization combined with nostril reduction—can give rise to extensive subcutaneous emphysema tracking from the face into the neck, mediastinum, and thorax. Although intraoperative findings were unremarkable, a small mucosal defect likely served as a conduit for pressurized air, underscoring the sometimes–occult nature of thermal injuries. Prompt recognition by clinical examination and CT imaging, together with early multidisciplinary intervention—including mediastinal drainage—proved critical to rapid symptom relief and full recovery. To minimize risk, surgeons should employ conservative energy settings when performing thermal turbinate reduction, inspect and repair any mucosal breaches intraoperatively, and counsel patients to avoid forceful Valsalva maneuvers after surgery. Vigilance for unexpected swelling and a low threshold for imaging will ensure timely management of this rare but potentially serious complication.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases. Written informed consent was obtained from the patient for publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the author or corresponding author upon reasonable request.