
Abstract

Significance Statement
In this article, we describe an occurrence of a congenital glottic web. Glottic webs are a rare occurrence, and symptoms overlap with those of more common or benign conditions such as laryngomalacia or respiratory infection. It is imperative that cases of glottic web are well documented to better understand their incidence and to allow for early diagnosis and treatment.
A 20-year-old active-duty female presented with a history of a congenital glottic web (Figure 1). She reported that she has always had a hoarse voice, but she has been otherwise healthy and asymptomatic. After joining the navy, she had noticeable exertional dyspnea and stridor during her physical readiness test. The congenital glottic web had made it difficult to pass the physical. On the GRBAS (Grade, Roughness, Breathiness, Asthenia and Strain) scale used to assess vocal quality, she was evaluated to be G1R1B1A1S0. Additional laryngeal functional tests found that she met the following 3 parameters that correlate to hoarseness. The average fundamental frequency, perceived as habitual speaking pitch, was higher than the normal limit. Additionally, noise to harmonic ratio and measures of perturbation of frequency (jitter %) and amplitude (shimmer %) were also increased. The overall pitch range also exceeded the normal limit. Habitual speaking loudness in connected speech and overall range of loudness were both decreased. Measures of mean peak air pressure and mean airflow during voicing were mildly increased.
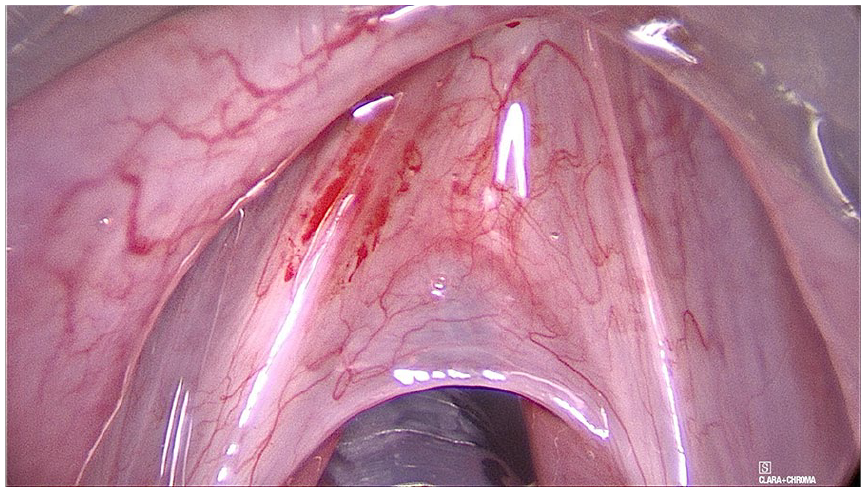
Glottic web. Intraoperative view of the congenital glottic web.
A failure of the larynx to recanalize can lead to the formation of a congenital glottic web. Glottic webs can be characterized as either anterior or posterior and staged according to Cohen’s classification based on approximate percentage of obstruction. The majority of diagnoses have been found to be anterior glottic webs. Congenital webs are often diagnosed based on symptoms of stridor, hoarseness, and persistent respiratory distress, but they have also been misdiagnosed for more common conditions such as respiratory illness or asthma. 1 Vocal abnormality is the most commonly reported dysfunction, and in some cases, the driving characteristic of diagnosis. 2 In this patient, hoarseness was the primary presenting symptom until the physical readiness test. Less symptomatic cases have also been found incidentally during difficulties with intubation. 3 The preferred method for staging and classification is rigid bronchoscopy, though flexible bronchoscopy and flexible laryngoscopy can be employed to consider and exclude the differential diagnoses. 4
An embryologic failure of the vocal folds to separate causes the development of the congenital glottic web. Studies investigating pathogenesis have suggested a genetic driver for this disruption. In 1 family, the laryngeal web malformation was found in 3 generations. 5 There is also a strong association between congenital glottic webs and the 22q11.2 deletion, which leads to disruption in the development of the third and fourth pharyngeal pouches. The diagnosis of a laryngeal web can be up to 40% sensitive for the diagnosis of this deletion. 3 Current research has also shown the β-catenin pathway may be implicated in the separation of the vocal folds. 6
Accurate and timely diagnosis is important in determining prognosis and treatment. Management is based on the Cohen classification, thickness of the web, and degree of subglottic extension. 7 Laryngeal webs can be treated either endoscopically with laser or with open reconstruction. In this case, the patient underwent micro suspension direct laryngoscopy with laser division of the glottic web and insertion of a glottic stent. Grades I to II often are treated endoscopically, while grades III to IV are often treated with an open repair. 8 An important consideration in treating congenital glottic webs is recurrence. In comparing the 2 approaches, researchers have found that regrowth of webbing can take place with either method. 7 A systematic review found that for grades I and II, there was no significant difference in morality or revision and in cases that were grades III and IV, there were lower revision rates for cases managed with an open approach. 8 There are no significant differences in the rate of recurrence regardless of method. 8 However, untreated cases can eventually lead to airway difficulties such as persistent respiratory distress and subglottic stenosis. 9
Footnotes
Ethical Considerations
Ethical approval to report this case was obtained in the form of written patient consent.
Author Contributions
Both authors contributed equally to the research and authorship of this article as outlined by the International Committee of Medical Journal Editors criteria.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.