
Abstract
Background:
Biopsy is required to stage cutaneous head and neck melanomas (cHNM), but cHNM can be pathologically upstaged following surgical resection. Here, we evaluated whether upstaged cHNM with negative sentinel lymph node biopsy (SLNB) impacts survival and time to cHNM recurrence.
Methods:
We retrospectively analyzed cHNM patients with negative SLNB treated from 2007 to 2014. We included adult cHNM patients with T2a-4a disease at biopsy who underwent SLNB-negative and wide local excision. We extracted patient demographics, treatment details, and survival outcomes. Melanoma-specific survival (MSS) and cHNM recurrence outcomes were analyzed using Cox regression analysis and 95% confidence intervals (95% CI).
Results:
Overall, 87 patients met inclusion criteria, 17 of whom were upstaged after definitive treatment. No significant baseline demographic or cHNM differences were observed between groups. Excisional biopsies were most performed (n = 57, 65.5%), yet upstaged patients more frequently underwent shave or punch biopsies. Most cHNM lesions were found on the face (n = 35, 40.2%). Univariable Cox regression revealed significant association between upstaged pathology (unadjusted hazard ratio: 3.20, 95% CI: 1.12-9.16), close margins (unadjusted hazard ratio: 4.95, 95% CI: 1.61-15.20), and worse MSS; however, multivariable Cox regression did not demonstrate any relationship between upstaged pathology or margin status and MSS.
Conclusion:
Among patients with pT2-4a, SLNB-negative cHNM, pathological upstaging does not independently predict MSS when adjusted for margin status, but large multicenter prospective cohort studies are needed to further validate these findings.
Keywords
Introduction
The incidence of cutaneous head and neck melanoma (cHNM) is increasing globally, and cHNM require biopsy to confirm primary staging and guide treatment.1,2 Surgical treatment for these lesions entails wide local excision (WLE) with extirpation of a margin of uninvolved tissue that is guided by the Breslow thickness, which guides the need for sentinel lymph node biopsy (SLNB).1,3 Despite the importance of an accurate diagnostic biopsy, partial biopsy techniques like shave or punch biopsy are employed due to technical and clinical considerations such as a low pre-biopsy suspicion for melanoma, challenging anatomic regions, and large lesions that may preclude accurate tissue sampling.3-6 While partial biopsy techniques are frequently utilized, they are associated with an increased risk of pathological upstaging, which is defined as a greater Breslow thickness on final pathology compared with the Breslow thickness of the initial biopsy, and carry implications for disease management and the need for additional surgery.3,7,8 Despite a negative SLNB in cHNM, high-risk pathological features, such as Breslow thickness >2 mm, are associated with worse disease prognosis and can help identify patients who may benefit from systemic adjuvant therapy despite an absence of nodal metastasis. 9 While positive sentinel lymph node status is a known major negative prognostic factor in cHNM, there are little data evaluating the association between pathological upstaging and disease outcomes in cHNM patients with a negative SLNB.10-12 Hence, the aim of this study was to determine whether pathological upstaging in patients with cHNM who have a negative SLNB is associated with worse clinical outcomes.
Materials and Methods
This was a retrospective cohort study of patients who underwent curative melanoma treatment at a tertiary care cancer center in Hamilton, Ontario, from 2007 to 2014. The study was approved by the Hamilton Integrated Research Ethics Board.
Patients and Data Collection
Adult patients (≥18 years old) with primary stage T2a-4a cHNM underwent negative SLNB. We excluded patients with palliative intent, previous head and neck oncologic surgery or radiation, previous cHNM, and previous metastatic cutaneous melanoma of any anatomical site. We collected data on demographics, patients, tumor, and treatment data, as well as survival outcomes. For all included patients, age-adjusted Charlson Comorbidity Index (CCI) scores were calculated using relevant comorbidities. Staging of the tumors was clinical and according to the eighth edition of the American Joint Committee on Cancer TNM staging manual. 13 We defined upstaging as an increase in Breslow depth within the final pathology from the WLE when compared to the first preoperative biopsy. All samples that had no residual melanoma were not considered upstaged.
Study Outcomes
The primary outcome measure was melanoma-specific survival (MSS), which was calculated as the time from the first date of melanoma diagnosis to the date of melanoma-specific death. Secondary outcomes included overall survival (OS).
Statistical Analysis
Patients and tumor demographics were summarized as mean and standard deviation (SD) or proportions and frequencies, where appropriate. Stratified descriptive data analysis was conducted on the demographic data of these 2 groups. Continuous data were compared using Student’s t test. Categorical data were compared using the chi-squared test. Survival outcomes were analyzed using Cox regression analysis and log-rank testing, where applicable. We performed univariable analysis for MSS and incorporated several a priori clinically-pertinent demographic, disease, and treatment variables. Multivariable Cox regression analysis was then performed using clinically-relevant predictor variables and those that achieved statistical significance in univariable analysis (ie, if variance inflation factor was at least 5, then the predictor variable was removed from the model), and over-fitting was avoided by ensuring that we had at least 10 outcome events for each predictor variable. 14 P < .05 were considered statistically significant. All analyses were performed with SPSS Statistics 20.0 (SPSS, Inc, Chicago, IL, USA).
Results
Patient and Tumor Characteristics
Eighty-seven patients with cHNM were identified as meeting our inclusion criteria, of which 17 underwent pathological upstaging after surgery (Figure 1). At baseline, there was no statistically-significant difference between upstaged compared with non-upstaged patients in terms of age, sex, final depth, Breslow depth, age-adjusted CCI, and deep margins (Tables 1 and 2). The upstaged and non-upstaged groups had comparable distributions of final pathological tumor staging. Most patients had excisional biopsies (n = 57, 65.5%) and upstaged patients were nearly 3 times more likely to have had shave (11.8% vs 4.3%) or punch biopsies (52.9% vs 15.7%; P = .002). The face was the most common subsite (n = 35, 40.2%). The peripheral margin between the 2 groups was statistically-significantly different [upstaged mean: 10.4 (SD: 5.17); non-upstaged mean: 21.2 (SD: 10.88), P = .001]. However, margin status was not statistically-significantly different between groups.
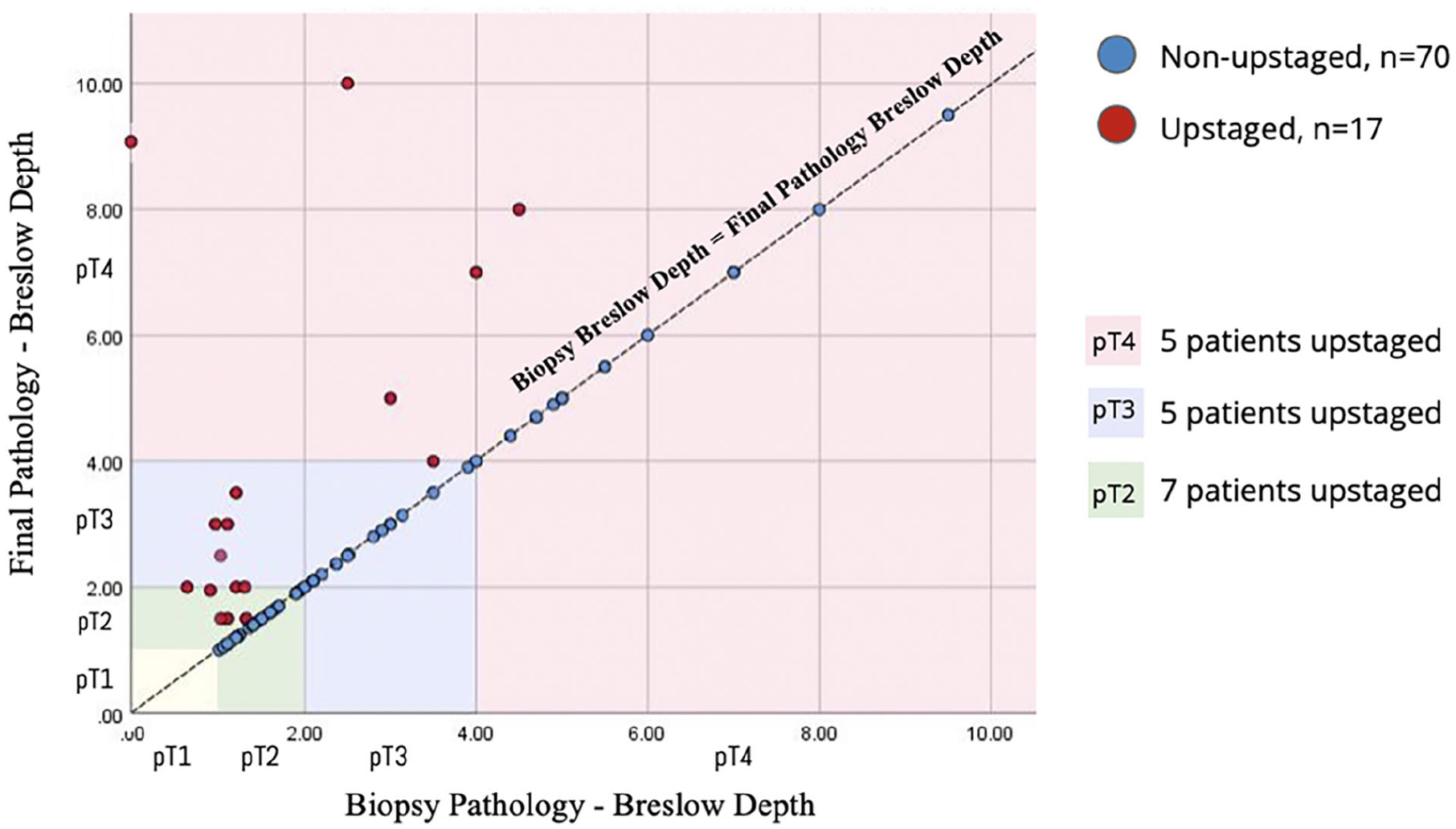
Group scatter of Breslow depth by biopsy upstaged. Seventeen patients were upstaged in final pathology (red dots) across pT2, pT3, and pT4 stages (red, blue, green rectangles, respectively), while 70 patients remained non-upstaged (blue dots).
Patient Demographics.
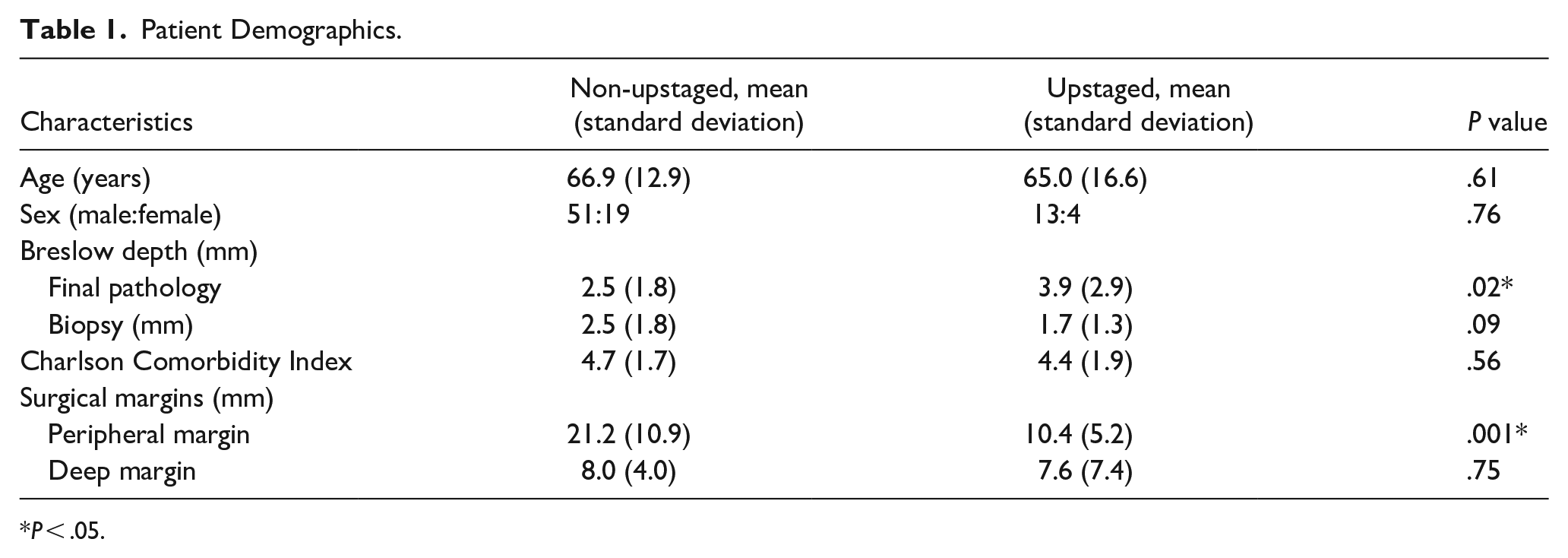
P < .05.
Cutaneous Head and Neck Melanoma Characteristics.
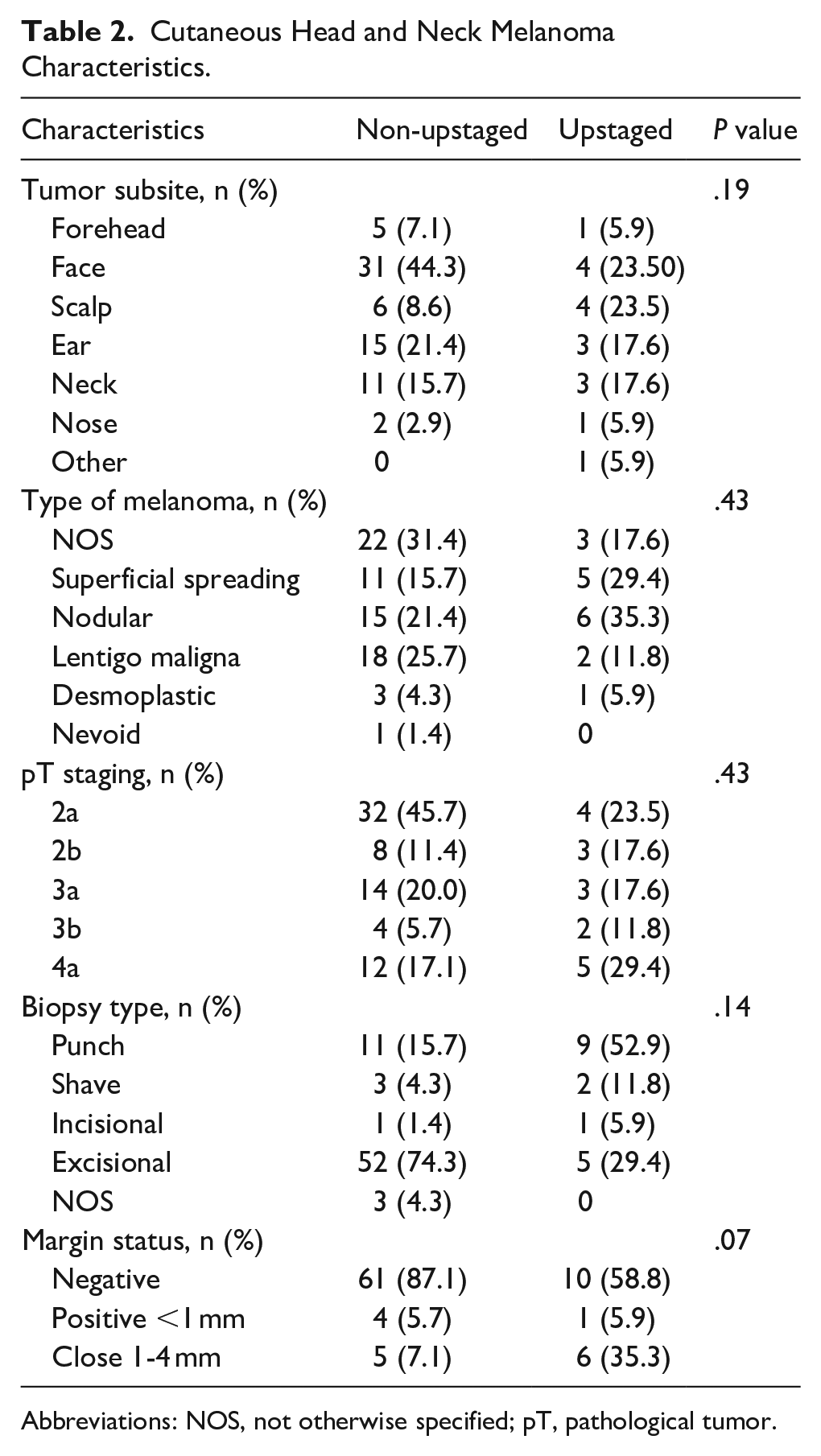
Abbreviations: NOS, not otherwise specified; pT, pathological tumor.
Survival Outcomes
The mean follow-up for all patients was 6.71 years (SD: 2.96, range = 0.66-12.38) and total of 43 (49.4%) patients died. Of the patients who died, 10 (58.9%) were from the upstaged group and 33 (47.1%) were from the non-upstaged group. Across both groups, 23 (26.4%) patients died secondary to melanoma. OS and MSS are shown in Figure 2. There was no statistically-significant difference in OS (X2 = 3.21, P = .07), time to locoregional recurrence (X2 = 3.66, P = .06), or time to distant metastasis between groups (X2 = 3.36, P = .07). However, pathologically-upstaged patients had worse MSS than non-upstaged patients (X2 = 3.21, P = .02).
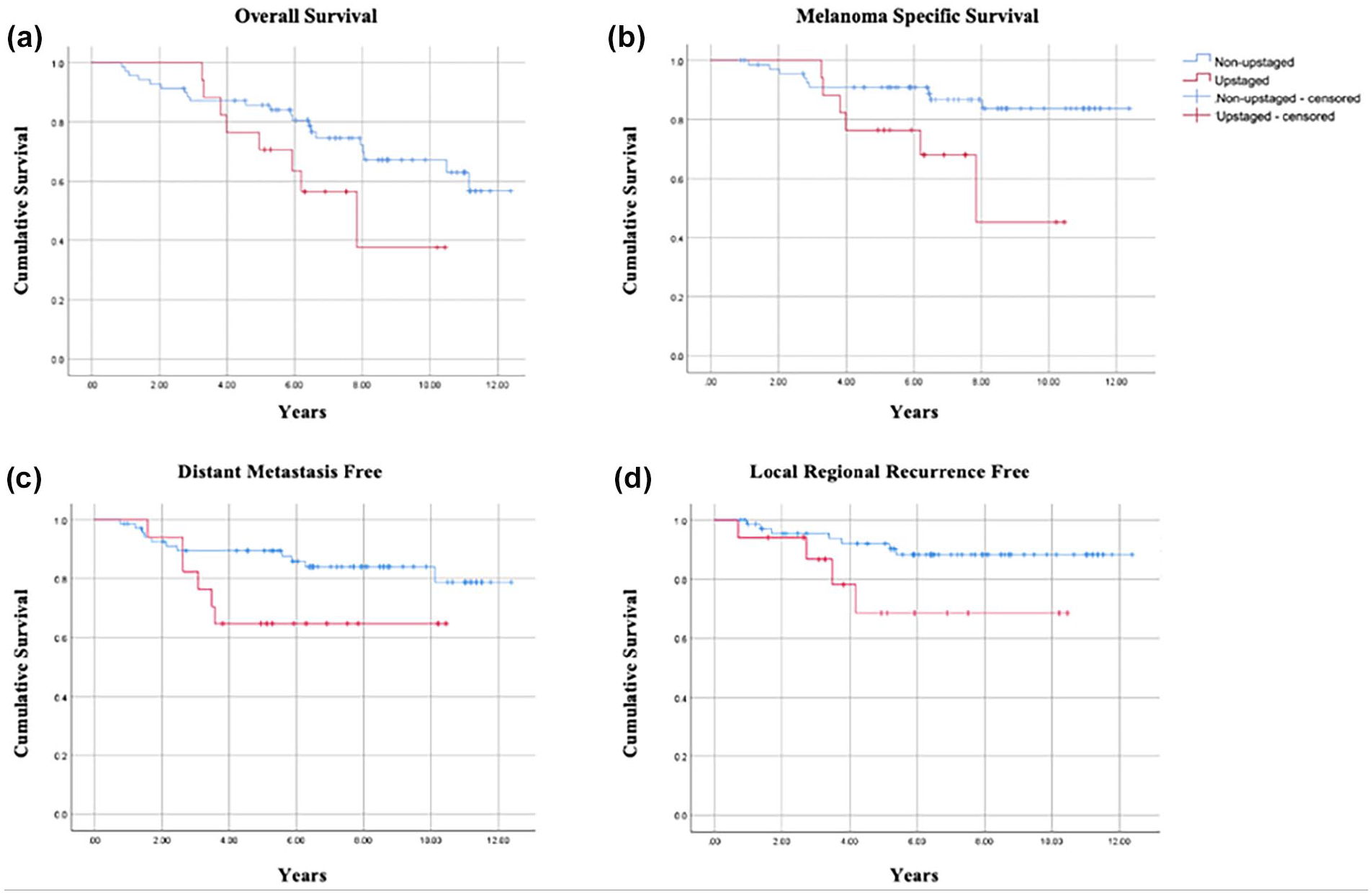
Kaplan-Meier curves for (a) overall survival, (b) melanoma-specific survival, (c) distant metastasis free, and (d) local regional recurrence free between the upstaged and non-upstaged group.
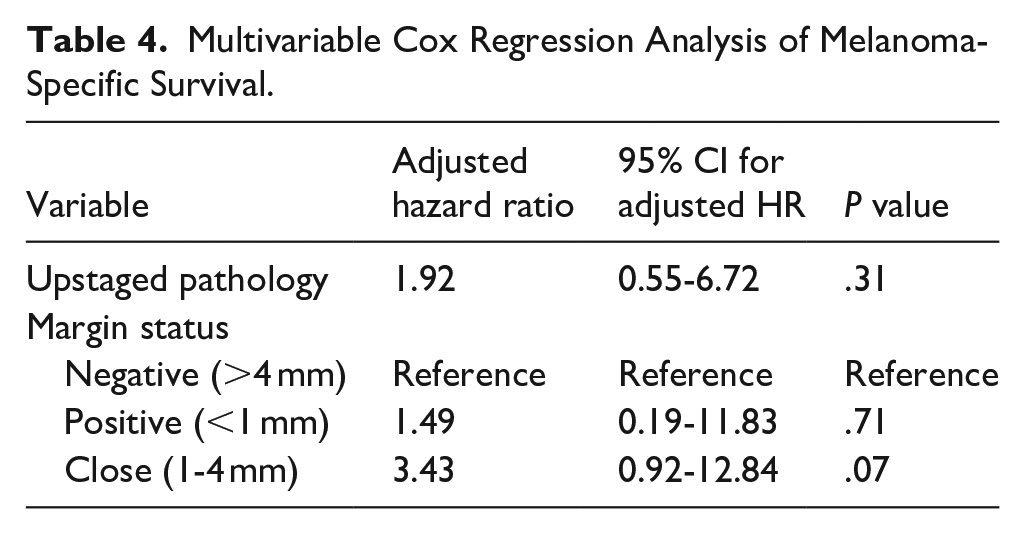
We then evaluated the impact of patient and disease factors on MSS using both univariable and multivariable Cox regression analyses. In our univariable analysis, pathological upstaging [unadjusted HR: 3.20, 95% confidence interval (95% CI): 1.12-9.16, P = .03] and close margin status (unadjusted HR: 4.95, 95% CI: 1.61-15.20, P = .01) were significantly associated with worse MSS (Table 3). In our multivariable Cox regression analysis, the proportional hazards assumption was satisfied, and no significant collinearity existed between margin status and pathological upstaging (ie, variance inflation factor = 1.12 for each variable). We found that neither pathological upstaging (adjusted HR: 1.92, 95% CI: 0.55-6.72, P = .31), positive margins (adjusted HR: 0.71, 95% CI: 0.19-11.83, P = .71), nor close margins (adjusted HR: 3.43, 95% CI: 0.92-12.84, P = .07) were predictive of MSS (Table 4).
Univariable Cox Regression Analysis of Melanoma-Specific Survival.
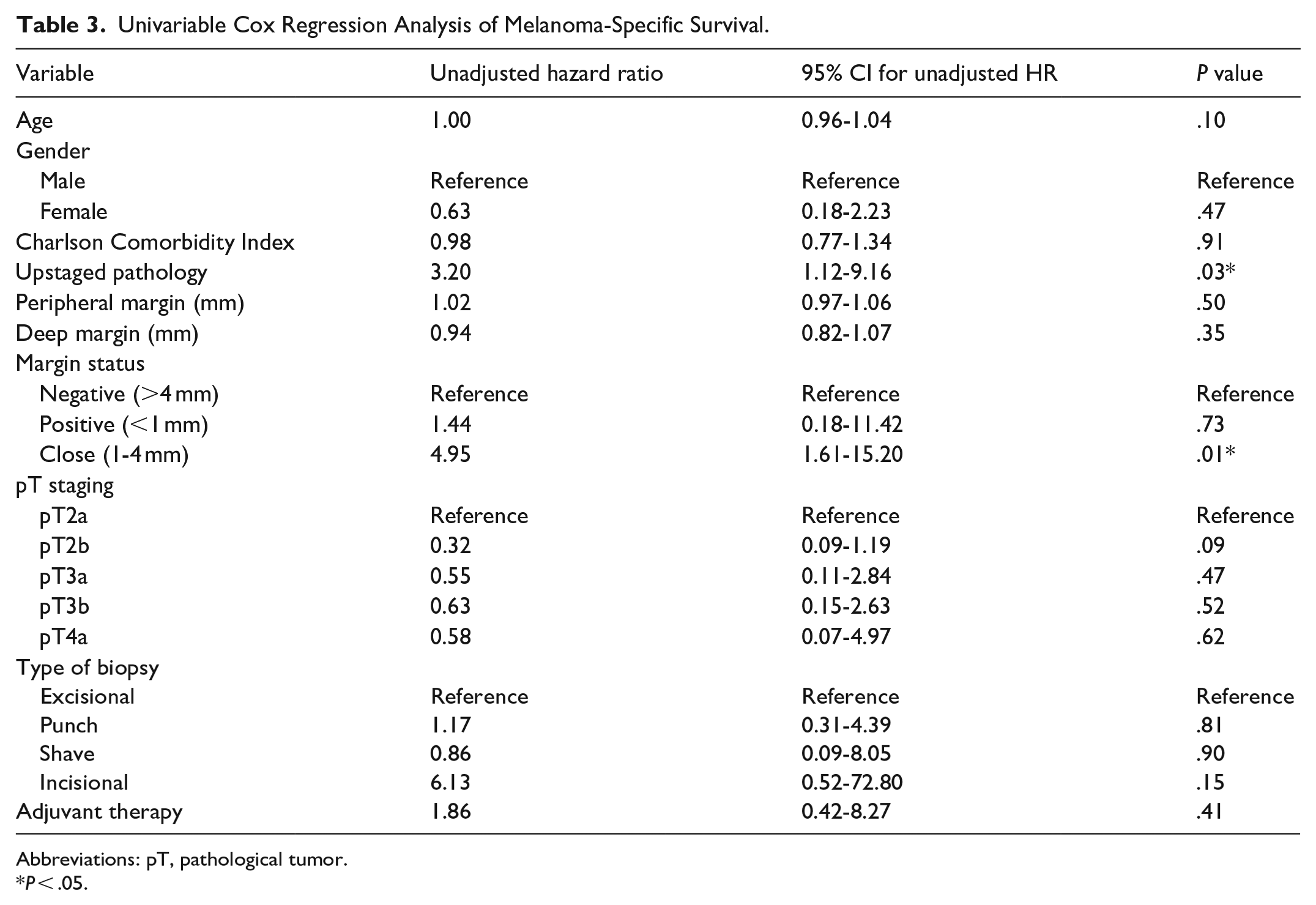
Abbreviations: pT, pathological tumor.
P < .05.
Multivariable Cox Regression Analysis of Melanoma-Specific Survival.
Discussion
We demonstrate that cHNM patients with negative SLNB and upstaged final pathology were found to have worse MSS on univariable analysis, but this finding was not maintained when adjusting for margin status. OS, time to locoregional recurrence, and time to distant metastasis were also not significantly different between patients with upstaged and non-upstaged cHNM. Lee et al similarly identified that an increase in tumor stage on final pathology was not significantly associated with a difference in recurrence-free survival or MSS in acral melanoma. 7 Likewise, Kim et al found that survival outcomes were unchanged in acral melanoma where the exact Breslow thickness was inaccurate on initial biopsy. 2 As with our findings, these authors did not identify an effect of pathology upstaging on survival outcomes when regression analysis was controlled for margin status. Additionally, Gazivoda et al determined that head and neck site, nodular melanoma, acral lentiginous melanoma, and lymphovascular invasion were all associated with upstaging on final pathology. 15
The trend toward close margin status in upstaged patients may be explained by surgeons accepting smaller surgical margins for functional or cosmetic reasons, due to an inaccurately-thin Breslow thickness on initial biopsy. Moreover, the initial decision for and increased frequency of partial biopsies among upstaged patients may also be influenced by similar functional or cosmetic concerns. Specifically, our study showed that upstaged patients were more likely to have had shave or punch biopsies, which is consistent with recent reports of increasing usage of partial biopsy methods to sample lesions suspicious for melanoma, despite some national guidelines recommending the use of narrow excisional biopsies.16-19 This association between partial biopsy methods and upstaging is previously described by Doolan et al’s retrospective review of 2304 consecutive cases of new primary cutaneous melanoma, which demonstrated higher rates of upstaging for punch, shave, and partial incisional biopsies than for excisional. 4 Our study’s results, in conjunction with existing literature, highlight the potential benefit of narrow excisional biopsies to minimize sampling error in suspected melanomas, especially given that partial biopsy methods may lead to upstaging and corresponding changes in prognostication and therapeutic decision-making.
A limitation of the current study is the small sample size and the lack of power for evaluating our primary outcome. This study was conducted at a single tertiary care center, which also carries the risk of selection bias for advanced or challenging cHNM. Additionally, the low number of outcome events and the risk for model over-fitting precluded the inclusion of other clinically-pertinent predictor variables in our multivariable Cox regression model. Our data also pre-date the use of immunotherapy at our center, which impacts outcomes in the adjuvant setting in patients diagnosed with stage IIB cHNM.20-22 Despite these limitations, this study advances our understanding of the prognostic impact of pathological upstaging on SLNB-negative cHNM patients.
Conclusion
In pT2-4a N0 cHNM, upstaged final pathology is not associated with worse MSS when adjusting for margin status. Upstaged final pathology in cHNM is associated with higher rates of shave or punch biopsies and small peripheral margins. Future multicenter prospective studies with larger sample sizes are needed to validate these findings and advance our understanding of pathological upstaging in cHNM.
Footnotes
Author Contributions
Surabhi Sivaratnam: data collection and manuscript preparation. Michael Xie and Phillip Staibano: study design, data collection, data analysis, and manuscript preparation. Sepideh Mohajeri: manuscript editing. Kelvin Zhou, Ali Zhang, and Raphaelle Koerber: data collection and data analysis. J.E.M. (Ted) Young and Han Zhang: study design, data collection, and manuscript preparation.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data are available upon request.