
Abstract
Cutaneous head and neck melanoma is a separate subgroup of cutaneous melanoma that has a worse prognosis than other primary sites. The aim of this article is to examine the significance of sex and site of primary lesion as additional risk factors. Primary localization distribution and metastatic disease in the neck in a retrospective cohort of 159 patients with cutaneous head and neck malignant melanoma were analyzed. Men develop primary melanoma more frequently than women in the left peripheral head and neck regions (P = .0364), as well as clinically visible and occult metastatic disease in the left side of the neck (P = .0138). Patients with clinically occult regional metastatic disease showed a significantly poorer survival rate than the rest of the group that underwent elective neck dissections (P = .0270). Left-sided disease in male patients may be an additional risk factor in cutaneous head and neck melanoma. Performing elective neck dissections in high-risk patients might identify patients with occult metastatic disease and worse prognosis but does not offer any significant therapeutic benefit.
Introduction
Cutaneous head and neck melanoma has recently been described as a separate clinical subgroup of cutaneous melanoma that has a significantly worse prognosis and is site- and sex-specific. 1 The reasons behind this distinction remain unclear. The disease retains the dual etiologic pathways of development from common nevi with slow progression to more invasive disease forms with radial and vertical growth or de novo development from normal skin. 2 It affects people in their most productive years of life, significantly earlier than most other malignancies and, despite good results if treated early, remains linked with poor survival rates once metastatic disease develops (5% of disease-specific 5-year survival if distant metastases occur). 3 Known risk factors for melanoma development, among others, include intermittent and cumulative solar and artificial UV radiation, frequency of exposure, and inherited susceptibility to radiation damage. 4 Hindrances to further investigation are possible variations in patient populations over time and insufficient data on anatomical distribution of cutaneous head and neck melanoma, especially in southern and eastern Europe. Published studies have established differences in localization between men and women, but very few have taken into consideration the specific localizations in the head and neck area. 5 Photoprotection of the head and neck area is difficult, especially considering that the area is exposed to the highest level of UV radiation, both chronic and intermittent. 6 Further understanding of UV exposure, disease progression, and disease epidemiology may yield more efficient prevention strategies. Our aim was to establish novel connections between sex, age, and anatomic distribution on the face and neck and previously known histopathologic prognostic factors could improve upon already reported inherent differences in melanoma histopathology depending on UV exposure patterns. 7,8
Patients and Methods
This retrospective longitudinal cohort study and its protocol included 159 patients and was approved by the University Hospital Centre Bioethical Board adhering to the Helsinki Declaration of 1983. All patients with cutaneous head and neck melanoma who were surgically treated from January 1, 2000, to December 31, 2012, in our National Referral Centre for Head and Neck Melanoma were eligible for inclusion in a comprehensive oncological database. Patients were eligible for inclusion if they had a histopathologically confirmed invasive cutaneous melanoma on the head or neck and underwent primary surgical treatment in our institution and had complete disease-specific follow-up of minimum 5 years. They were treated according to standard clinical practices approved by a multidisciplinary oncological team. Clinical staging was carried out according to the current National Comprehensive Cancer Network/American Joint Committee on Cancer staging system. 9 The patients were included consecutively, with demographic information, prior history of skin malignancy, location, lesion size, previous therapy, surgical procedure, and occurrence of regional metastatic disease noted. Histopathologic analysis encompassed primary lesion Breslow thickness and Clark levels, presence of ulceration, mitosis number per mm2, tumor invading lymphocytes, satellitosis, sentinel lymph node biopsy (SNLB) results, number of examined lymph nodes, number of positive lymph nodes, extracapsular spread, and/or perineural invasion. All of the patients signed informed consent forms after evaluation by a multidisciplinary oncology team. Due to strict study protocol criteria, 83 patients were not eligible due to the following: patients with melanoma in situ lesions (noninvasive melanomas), incomplete documentation, incomplete follow-up, or localization of melanoma on mucosal surfaces. Metastatic involvement of cervical lymph nodes was documented and correlated with primary lesion localizations. These primary lesions were divided into 3 different anatomic regions: (1) central face (forehead, nose, paranasal and infraorbital area, lips, chin, and medial neck); (2) left peripheral head and neck (scalp, auriculotemporal, zygomatic, and buccal regions); and (3) right peripheral head and neck (scalp, auriculotemporal, zygomatic, and buccal regions). This was done in accordance with previously published studies that have confirmed that the division is clinically significant. 7,8
Statistical analysis was performed using MedCalc software (version 11.2.1 ©1993-2010; MedCalc Software bvba Software, Mariakerke, Belgium), using standard descriptive statistics and frequency tabulation as indicated. Associations between variables were assessed using Mann-Whitney U test, Kruskal-Wallis test, and Kaplan-Meier curve, Mantel log-rank test applied to end points to establish statistically significant correlations. All tests of statistical significance were performed using a 2-sided 5% type I error rate.
Results
This study included 159 surgically treated patients from January 1, 2000, to December 31, 2010, while maintaining strict exclusion criteria. Among the 159 patients who were eligible for inclusion, 56 were women and 103 were men, with a male to female ratio of 1.84. Average age was 58.12 years, with age ranging from 11 to 96 years. Among the 159 patients, there were 50 lentigo maligna melanomas (31.4%), 57 nodular melanomas (35.8%), 48 superficial spreading melanomas (30.1%), and 4 desmoplastic melanomas (2.5%). Breslow thickness ranged from 0.11 to 17 mm, with an average thickness of 3.02 mm. Men were affected significantly more often (Mann-Whitney U test, P < .001; Table 1). The highest incidence of head and neck melanoma was in the age-group of 61 to 80 years, followed by the age-group of 41 to 60 years. There was no statistical difference in average age at primary lesion occurrence between sexes. There were 35 patients in T1, 34 in T2, 50 in T3, and 40 in T4 disease stages. There were 115 patients in clinical N0 stage, 22 in N1, 17 in N2 stage, and 5 in N3 stage (Table 2). Standard procedure was to perform an excisional biopsy and a definitive re-excision if melanoma was histopathologically confirmed. When Breslow thickness measured between 1 and 4 mm, an SNLB was performed. Patients with positive sentinel lymph nodes underwent modified radical neck dissections in a separate procedure, after obtaining definitive pathohistological results. In patients with high-risk lesions, but a clinically negative N status, elective neck dissections were performed. Lymphoscintigraphy was performed in select patients with Breslow thickness over 4 mm in order to investigate lymph node drainage patterns which could be included in subsequent elective neck dissections. In patients with high-risk lesions (T3b, T4a, and T4b) and a clinically negative neck, elective neck dissections were performed. The minimal extent of elective neck dissections included ipsilateral regions II, III, and IV, with I or V included depending on the primary tumor localization. In patients with clinically apparent metastatic disease, curative neck dissections were performed. Sentinel lymph node biopsies were performed in 62 patients and 15 were positive for metastatic disease. The 15 patients with positive SNLB were included in the cN0 group data analysis and underwent completion modified radical neck dissections, but at a later date, after definitive histopathologic results were obtained and were excluded from comparison between clinically positive and negative neck dissections. There were 35 elective neck dissections and 37 curative radical or modified radical neck dissections. In addition, 27 superficial parotidectomies and 4 total parotidectomies were performed. In total, 45 patients were histopathologically positive for regional metastatic disease. In 37 patients, the metastases were clinically evident, and in additional 8 patients (17.8%, 7 males and 1 female), occult regional metastatic disease was found after elective neck dissections for clinical N0 stage. Adjuvant radiotherapy and chemotherapy were recommended to all patients with histopathologically positive regional metastatic disease, including patients with positive SNLB.
Clinical and Histological Characteristics of Cutaneous Head and Neck Melanomas According to Sex and Age.
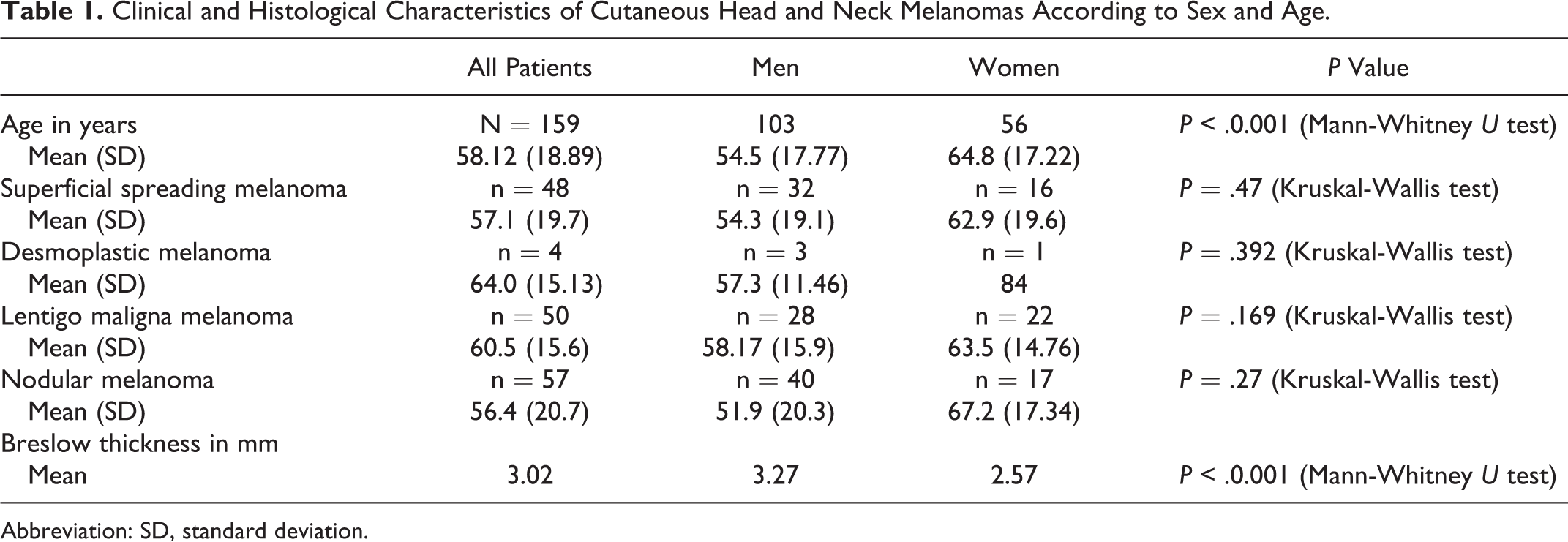
Abbreviation: SD, standard deviation.
Distribution of Head and Neck Melanomas’ T and N Stages According to Sex.a
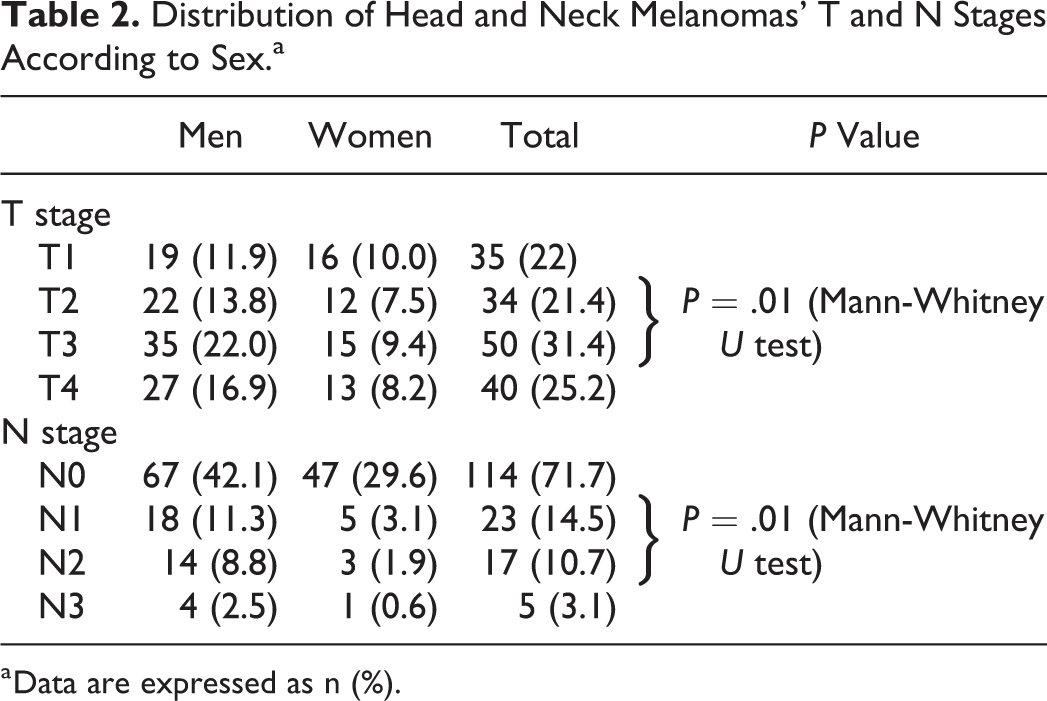
a Data are expressed as n (%).
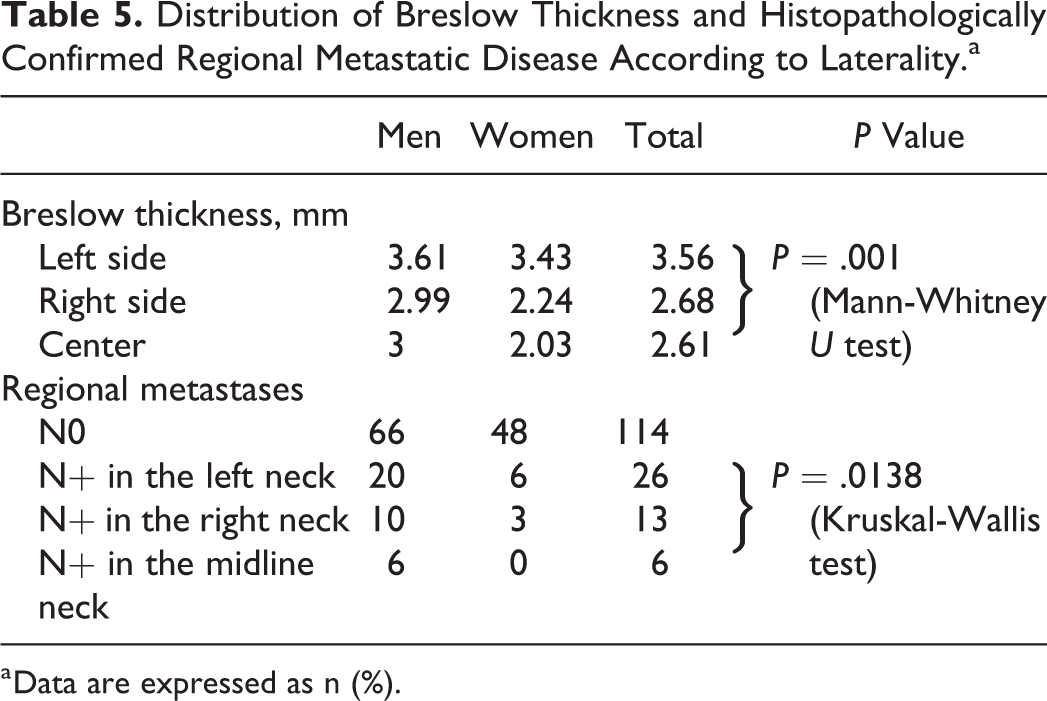
Data from the total cohort population (n = 159) show that the most frequent localization of the primary lesion was the left peripheral face and neck region (n = 72, 45.3%), followed by the right peripheral region (n = 46, 28.9%) and the central region of the head and neck (n = 41, 25.9; Table 3). After analyzing the relationships between anatomical distribution and sex, it became apparent that men develop primary melanoma lesions more frequently than women in the left peripheral head and neck regions (P = .0364, Kruskal-Wallis test; Table 4). Breslow thickness is significantly higher in both sexes in the left lateral regions versus the rest of the head and neck (Mann-Whitney U test, P = .001). Clinically apparent regional metastatic disease is significantly more frequent in men, who, in addition, develop clinically visible and occult metastatic disease more frequently in the left side of the neck (P = .0138, Kruskal-Wallis test; Table 2). Histopathological type of melanoma showed that desmoplastic and nodular melanoma types correlated with an increasing number of elective and curative neck dissections (Kruskal-Wallis test, P < .000001). When analyzing the relationship between N stage and histopathologic data, greater Breslow thickness correlated positively with increasing N stage (Kruskal-Wallis test, P = .0003). Poorer survival correlated well with rising T categories (Kaplan-Meier curve, Mantel log-rank test, P = .0045; Figure 1). Rising T stage correlated positively with the possibility of performing an elective or curative neck dissection (Kruskal-Wallis test, P < .000001; Table 5 and Figure 2). Elective and curative dissections were performed significantly more often in male patients than in female patients (Kruskal-Wallis test, P = .041; Figure 3). The group of patients with clinically occult regional metastatic disease showed a significantly poorer survival rate than the rest of the group that underwent elective neck dissections (Kaplan-Meier curve, Mantel log-rank test, P = .0270; Figure 4). There was no difference in survival between patients with occult or clinically visible regional metastatic disease (Kaplan-Meier curve, Mantel log-rank test, P = .6835; Figure 5).
Distribution of Head and Neck Melanomas According to Major Topographic Location and Sex.a
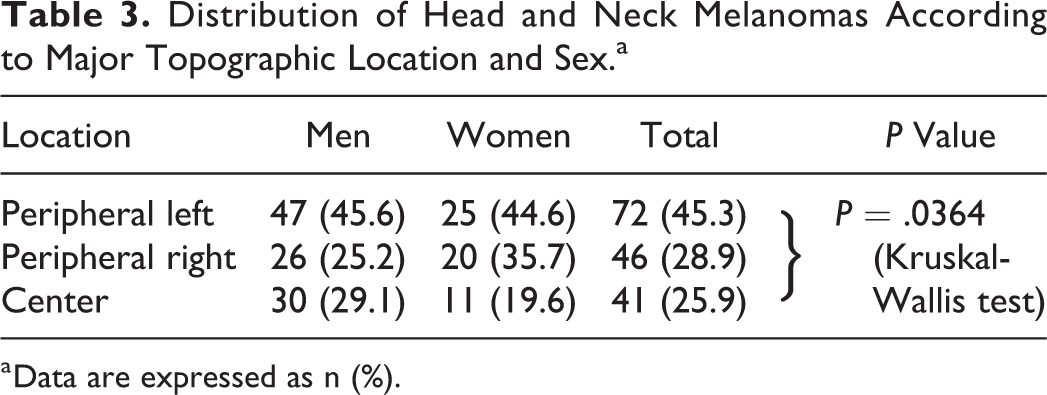
a Data are expressed as n (%).
Detailed Topographic Distribution of Head and Neck Melanomas According to Sex.a
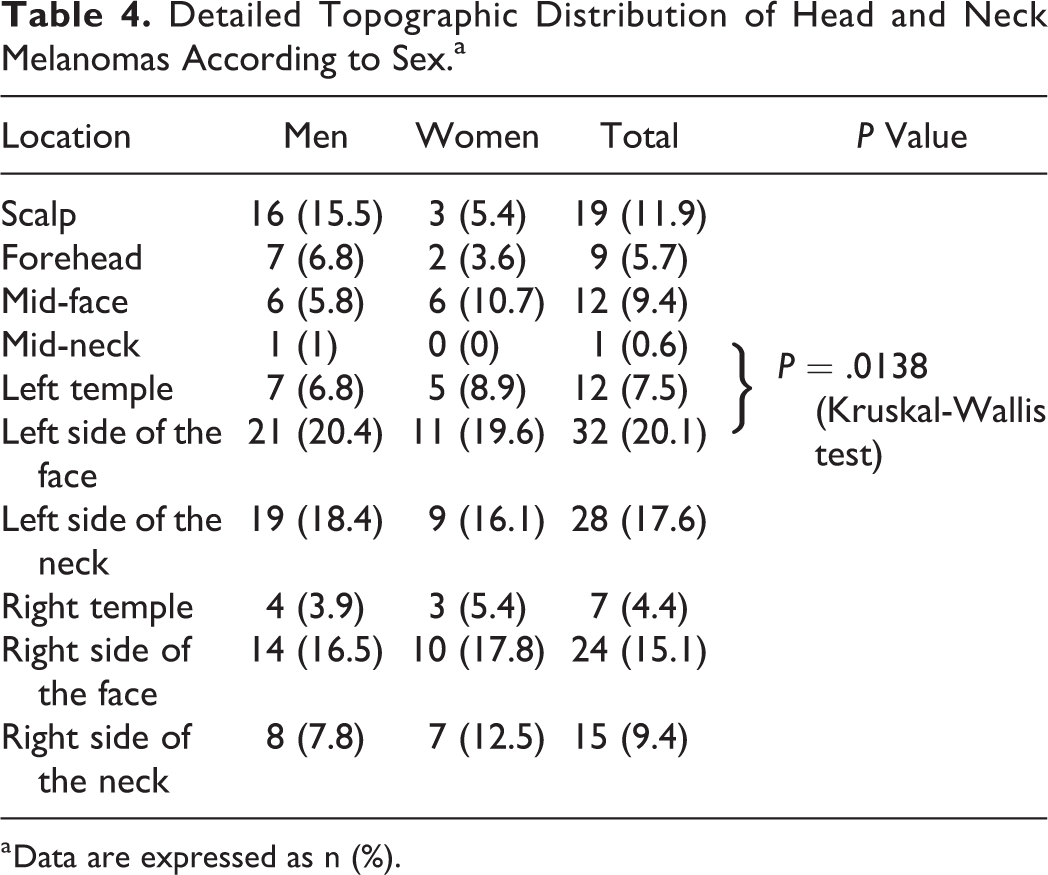
a Data are expressed as n (%).
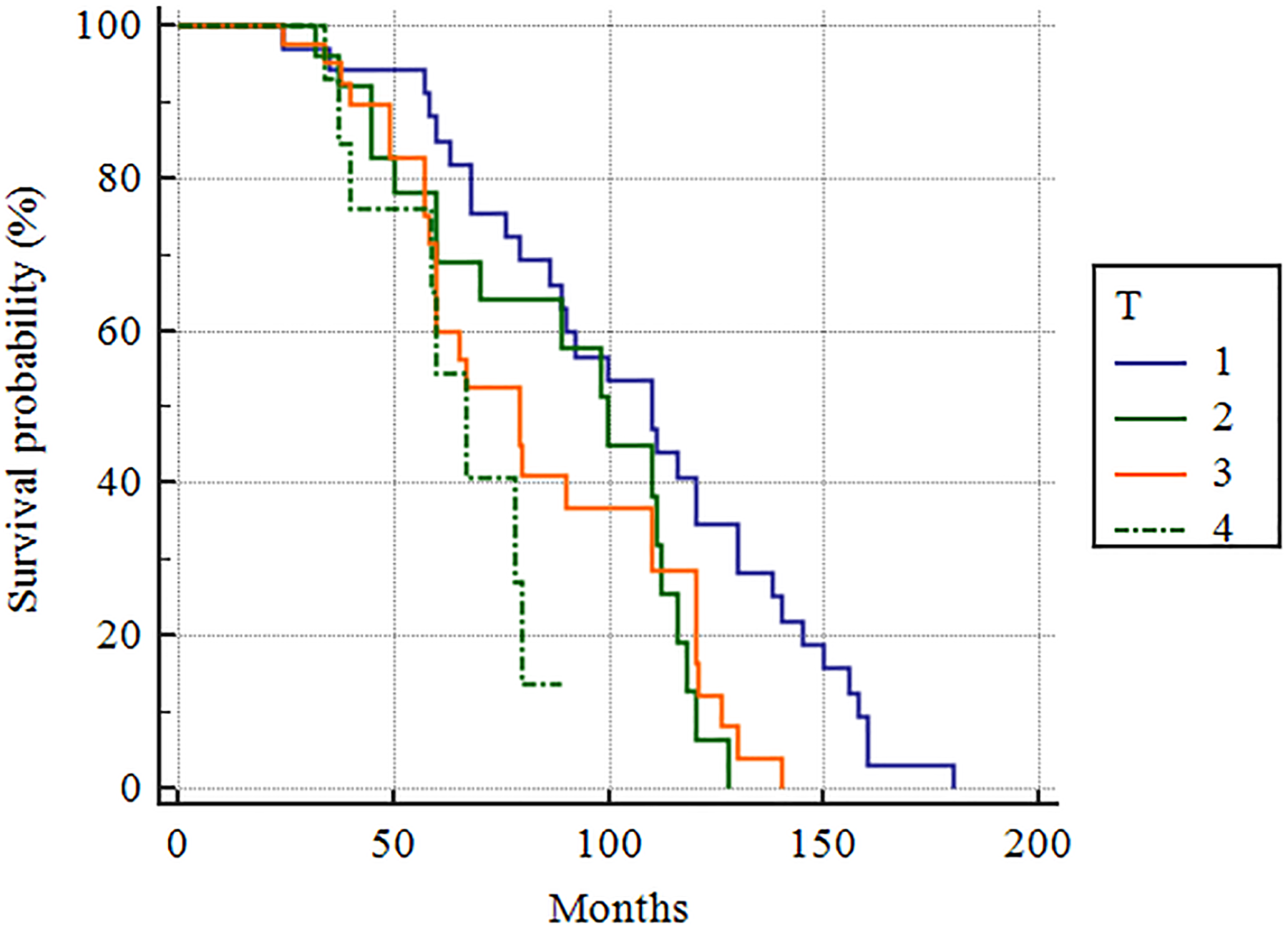
Survival distribution according to T categories in our patient cohort (Kaplan-Meier curve, Mantel log-rank test, P = .0045).
Distribution of Breslow Thickness and Histopathologically Confirmed Regional Metastatic Disease According to Laterality.a
a Data are expressed as n (%).
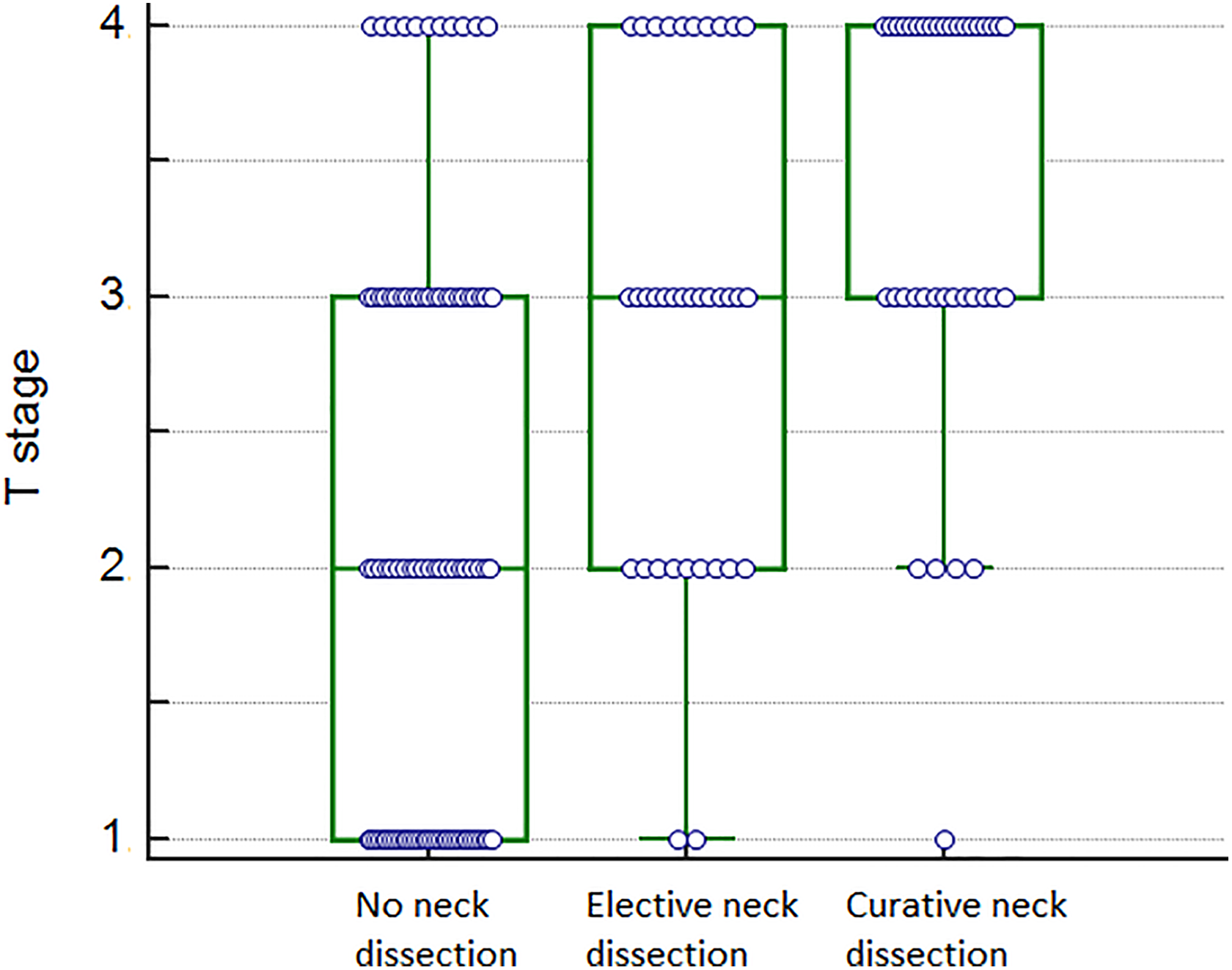
Relationship between rising T stage and performing an elective or curative neck dissection (Kruskal-Wallis test, P < .000001).
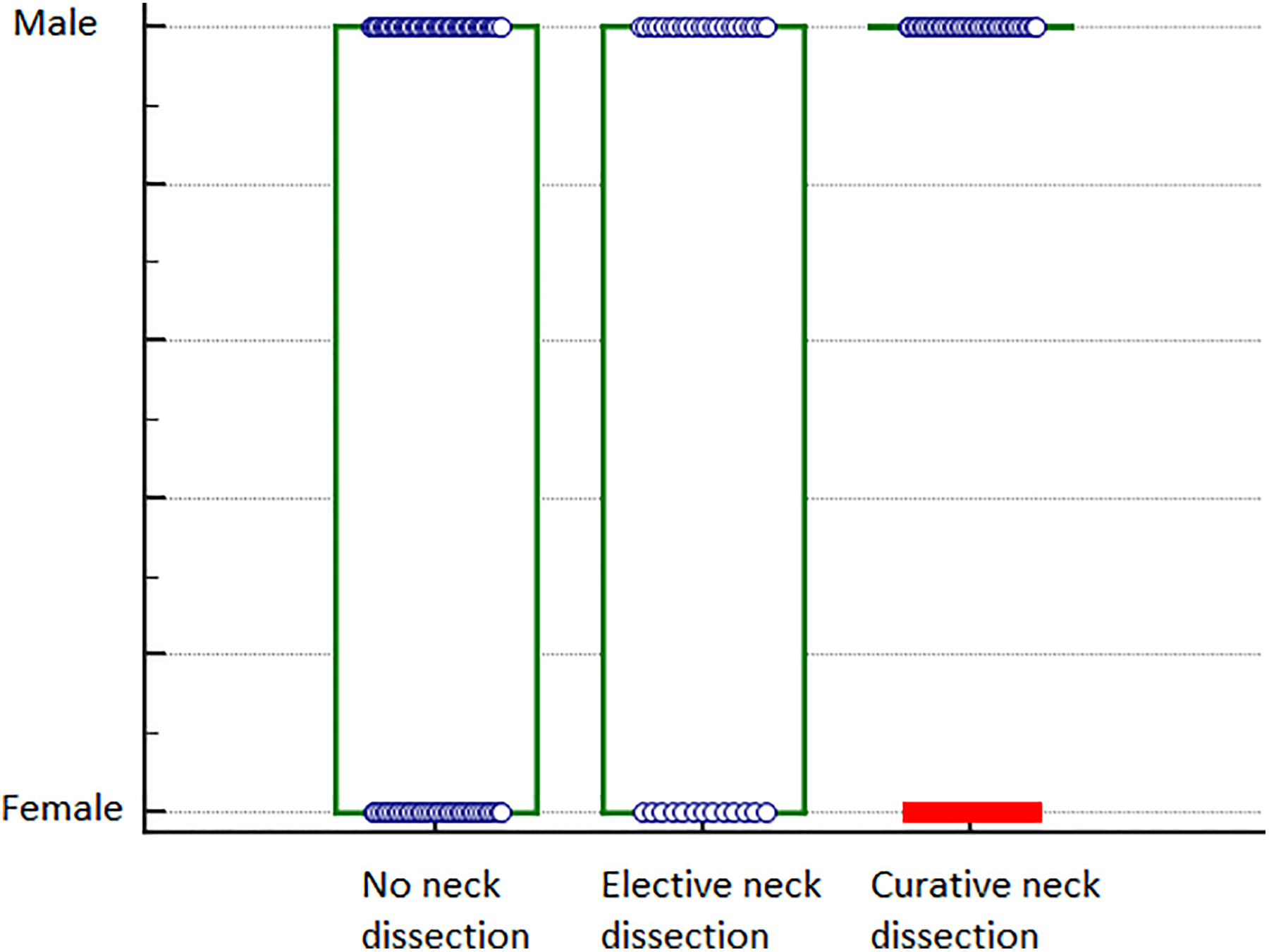
Relationship between sex and performing an elective or curative neck dissections (Kruskal-Wallis test, P = .041).
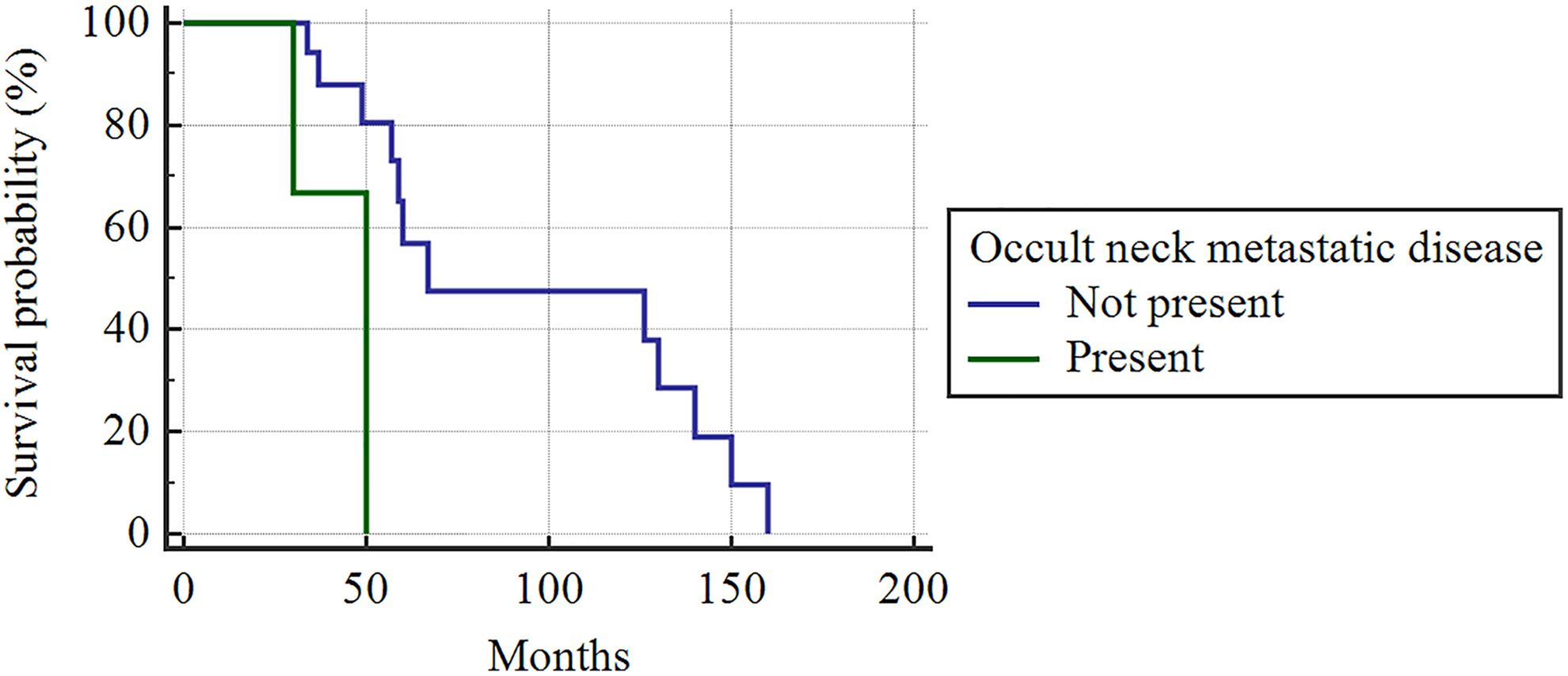
Survival in the group of patients who underwent elective neck dissections (Kaplan-Meier curve, Mantel log-rank test, P = .0270).
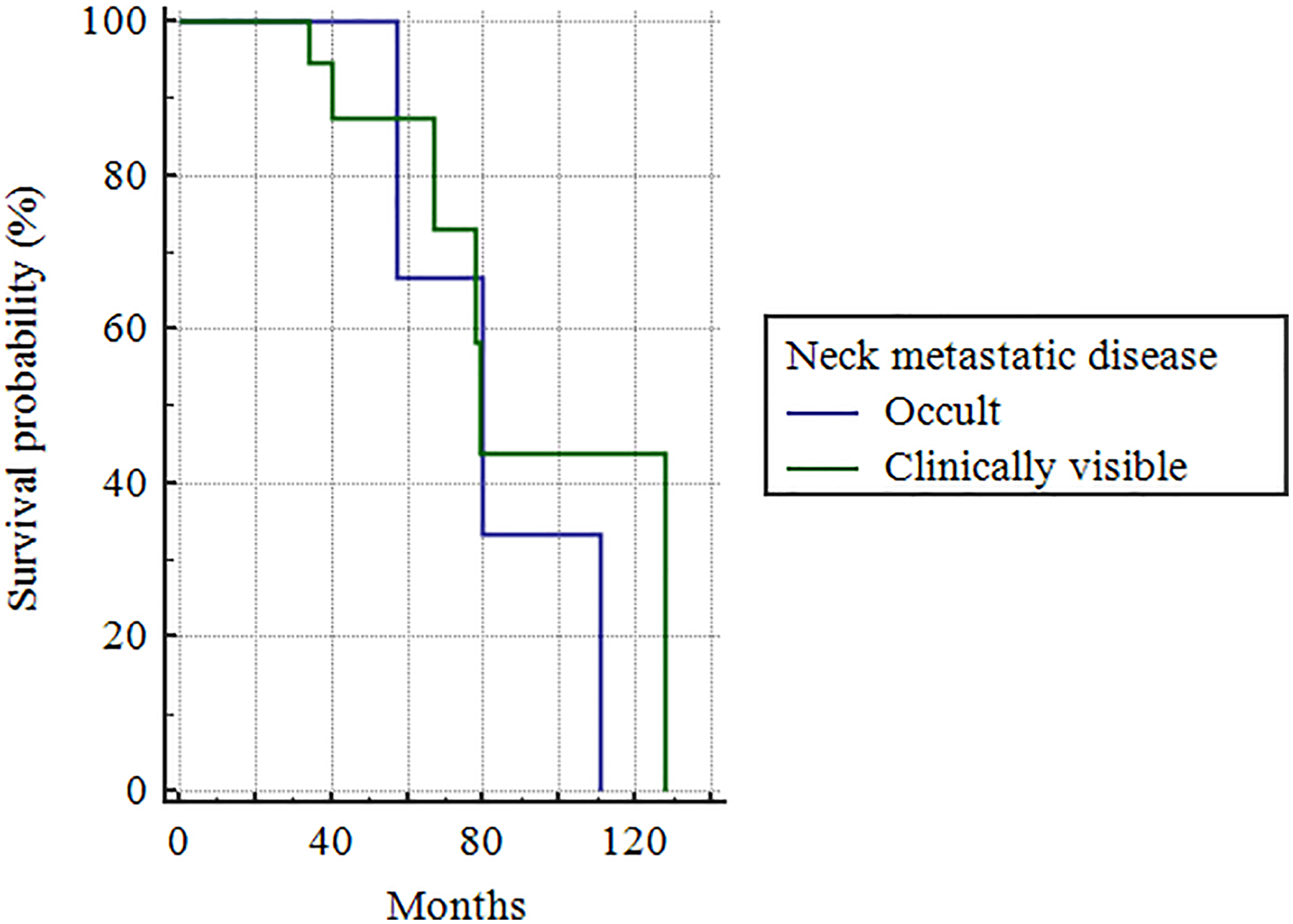
Survival in the group of patients with histopathologically identified regional metastatic disease (Kaplan-Meier curve, Mantel log-rank test, P = .6835).
Discussion
Data are already available on sex-specific differences in increasing melanoma incidence, with a greater yearly increase of thin lesions in women and thick lesions in men (4.1% per year compared to 6.1% per year, respectively), and a correlation between different sun exposure patterns in men and women and different anatomical sites of primary lesion occurrence. 10,11 The correlation between sex and anatomic distribution of head and neck melanoma has long been considered as an inherent characteristic, but recent studies have shown that anatomic distribution can change over time, owing to changes in clothing and lifestyle. 12,13 Few studies have attempted to evaluate connections between sex and anatomic localization as possible risk factors in cutaneous malignant melanomas occurring in the head and neck region and extent of surgery for regional metastatic disease. The strength of this study are its population-based design and precise epidemiologic, histologic, and anatomic data considered in detail. In addition, this is the first study, to our knowledge, that described a significant positive relationship between patterns of regional metastatic disease spread, sex, and laterality. Although these data are suggestive of possible more complex but poorly understood underlying mechanisms, it is important not to overstate its implications in clinical decision-making when treating patients with head and neck melanoma.
Although the constantly increasing incidence of cutaneous head and neck melanoma can partially be attributed to earlier diagnosis, an additional factor of increased UV radiation exposition in both sexes should be investigated. When considering UV radiation, it is important to note that differences in head and neck skin exposure due to sex-specific patterns of face coverage, use of indoor tanning devices, and hair style are clearly present. 14
It is important to note that several studies have previously noted a higher incidence of malignant melanoma on the left side of all body surfaces and hypothesized that it could be related to UV exposure and driving, but the same pattern was noted in countries with right-sided cars as well. 15,16
Other hypotheses were proposed, such as differential neural crest melanocyte migration during embryogenesis or circulatory system asymmetries in angiogenesis and response to DNA damage, but a satisfactory explanation on this asymmetry is lacking. 17,18
The average age of diagnosis in our patients was 58.12 years, with the majority of head and neck melanomas occurring in the age-group of 61 to 80 years, followed by the age-group of 41 to 60 years, which is consistent with published results. 5 There was no statistical difference in average age at primary lesion occurrence between sexes, which can be attributed to a comparable dose of lifelong UV irradiation among both sexes, but men are affected significantly more often than women (P < .001), which corresponds to known trends. 12 This study compared laterality between sexes, noting that men develop primary lesions significantly more frequently than women in the left peripheral regions of the head and neck (P = .0364). These results reinforce the findings of the few similar earlier studies on the subject. 8,9,11,14,15 -17 Some studies connect head and neck cutaneous melanomas with chronic patterns of sun exposure, while truncal melanomas correlate with intermittent patterns of sun exposure. 8 When observing data from the National Cancer Institute’s Surveillance, Epidemiology and End Results Program, rates of invasive cutaneous melanoma of the ear were found to be 7-fold higher in men. In addition, a 3-fold higher rate of scalp and neck melanoma incidence compared with a less than 2-fold higher incidence rate of melanoma on the face was observed. 1 The systematically higher incidence of invasive melanoma on the ear, scalp, and neck compared with the central face in males and females is consistent with results that promote the importance of hair cover in long-term UV protection of the skin. 5,13
Cutaneous head and neck melanoma has a relatively high metastatic rate to regional lymph nodes, but the extraordinarily well-developed neck lymphatic system poses a strong barrier to further metastatic spread. 19 Bearing that in mind, local and regional disease control is essential in improving survival. The results of surgical treatment are excellent when undertaken in stages I and II, but in patients who develop regional, and especially systemic metastatic, disease, survival is adversely affected. 20
Lymphatic metastases were identified in 28% of our patients, which is slightly higher than previously reported rates of 20%. 19,20 The incidence rate reflects the practice environment of the authors, since the patients referred to our National Referral Center for Head and Neck Melanoma are more likely to have aggressive or advanced disease. Our results show Breslow thickness to be significantly higher in both sexes in the left lateral head and neck regions versus the medial and right regions (P = .001). Further analysis of the relationship between N stage and histopathologic data reveals a positive correlation between desmoplastic and nodular melanoma types and an increasing number of elective and curative neck dissections (P < .000001), which is to be expected considering they are the most aggressive and have a propensity for developing early metastatic disease. Increasing Breslow thickness also correlated with increasing N stage (P = .0003), confirming the importance of lesion thickness as the most important prognostic factor for melanoma, with thicker lesions leading to earlier and farther regional and systemic disease dissemination. 20 This, in turn, leads to a significantly more frequent occurrence of clinically apparent and occult regional metastatic disease when the primary lesion is in the lateral left regions in men (P = .0138). The role of elective neck dissections in patients with high risk for developing regional metastatic disease is controversial. Theoretically, removing occult metastatic disease should improve survival, with several studies confirming this idea in patients with occult regional metastatic disease. Unfortunately, there are no established criteria in deciding which patients should be treated with elective neck dissections or describing their extent. One meta-analysis has shown that not all patients benefit equally from an elective neck dissection, with the most benefit observed in patients with primary lesion thickness <2 mm. Survival was significantly improved in patients who had clinically occult regional metastatic disease, which is consistent with the goals of our study. 19,20
An additional reported finding to consider is the higher rate of regional metastatic disease reccurrence in T3 and T4 tumors postsurgery than compared to other body areas, such as the axilla or inguinum, which emphasizes the need for adequate risk assesment when considering surgery and planning its extent. 20
We performed elective neck dissections in all patients with stage T3b, T4a, and T4b who had a clinically negative neck. The patients with positive SNLB were included in the clinical N0 group but were excluded from comparison between patients with clinically positive and negative neck metastatic disease, since grouping them alongside cN0 or pN+ patients would influence the statistical analysis of high-risk patients undergoing elective neck dissections, who were a group of interest for this study. All of the 15 patients with positive SNLB underwent complete modified radical neck dissection, but in a separate surgery, after definitive histopathologic results were confirmed. These patients were least likely to influence the statistical analysis if excluded from analysis, although they do not differ in disease-specific mortality from pN+ patients. 21 The strategy of performing elective neck dissections in high-risk patients identified additional 8 (17.8%) male patients with occult metastatic disease of the 45 patients who were histopathologically positive for regional metastatic disease. This is a relatively high percentage that should call further attention to the need of adapting our surgical strategy when assessing a male patient with a high-risk primary lesion situated on the left lateral head and neck region. The average lesion thickness in the group of patients with occult metastatic disease was 2.75 mm, and T stage also correlated well with the chances of performing an elective or curative neck dissection (P < .000001), supporting our surgical strategy of treating patients with high-risk primary tumors and without clinically visible regional metastatic disease with elective neck dissections. In addition, both elective and curative neck dissections were performed more often in male patients, emphasizing the importance of considering sex-related differences in distribution of high-risk primary lesions and the possibility of regional metastatic disease when planning surgical treatment. Our results showed that in the group of patients treated with elective neck dissections, patients with occult regional metastatic disease had a worse prognosis than patients without regional metastatic disease. There was no difference in survival between the group of patients with occult regional metastatic disease and clinically visible regional metastatic disease (P = .6835), which suggests there is no therapeutic benefit to performing elective neck dissections but rather provides prognostic information for the patient, without changing treatment recommendations for high-risk patients with histopathologically proven N0 disease. However, the decision to recommend adjuvant radiotherapy and chemotherapy with immune checkpoint and BRAF-targeted inhibitors in our patient cohort was impacted by identifying patients with occult neck disease (stage III patients). This is a valuable argument supporting continued use of elective neck dissections in high-risk patients, since it may confer additional therapeutic benefit on a subgroup of patients who would otherwise remain untreated. 22
The systematically higher incidence of invasive melanoma in the left peripheral head and neck areas in men and its increased metastatic potential may have practical implications, since left-sided disease in male patients seems to be an additional risk factor in cutaneous head and neck melanoma but should be primarily targeted at disease prevention and patient education, since treatment-related decisions for patients with head and neck melanoma should rely on already well-documented data.
In summary, performing elective neck dissections for high-risk primary lesions defines a subgroup of patients with more favorable prognosis but does not conclusively argue for the therapeutic benefit of neck dissection in these patients.
Footnotes
Authors’ Note
This manuscript was approved by the University Hospital Centre Sestre milosrdnice, Zagreb, Bioethical Board adhering to the Helsinki Declaration of 1983. Full written informed consent was obtained from the patients in using their data. All of the authors have read and approved the manuscript, and all authorship contributions have been verified to adhere to ICMJE guidelines.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.