
Abstract
Retained nasal foreign bodies are commonly encountered in pediatric patients but can go unrecognized when symptoms mimic other chronic nasal conditions. We report the rare case of a 17-year-old female who presented with a 13-year history of unilateral nasal obstruction, purulent discharge, hyposmia, and sleep disturbances. Imaging revealed a metallic foreign body, consistent with a button battery, lodged in the right nasal cavity with associated fibrotic obliteration of the nasal vestibule. The patient underwent endoscopic surgical removal of the battery with favorable postoperative outcomes. This case underscores the importance of considering nasal foreign bodies in the differential diagnosis of chronic unilateral nasal symptoms, regardless of patient age, and highlights the critical role of imaging in prolonged or atypical presentations.
Introduction
Nasal foreign bodies are common in pediatric otolaryngology and often present with symptoms such as unilateral nasal obstruction, foul-smelling rhinorrhea, or recurrent infections. These cases are typically diagnosed early, but delayed recognition, particularly in the case of hazardous objects like button batteries, can result in severe complications. Button batteries pose a unique threat due to their ability to cause tissue damage through mechanisms such as chemical leakage, pressure necrosis, and electric discharge.1,2 The case also demonstrates the diagnostic value of imaging, specifically the “double ring sign” observed on computed tomography (CT) scans, which is crucial for identifying button batteries and differentiating them from other radiopaque objects. 3
Case Presentation
Patient History and Clinical Presentation
A 17-year-old female, with no significant medical or surgical history, presented to our hospital after years of intermittent symptoms. At the age of 4, she initially sought medical attention at a private hospital due to persistent unilateral nasal obstruction. This was accompanied by sleep disturbances, snoring, hyposmia, mouth breathing, recurrent infections, unilateral purulent nasal discharge with an unpleasant odor, minimal nasal bleeding, and nasal tearing. There was no history of facial trauma, prior surgical interventions, or allergies to medications. Despite persistent symptoms, the initial diagnosis of a nasal foreign body was missed due to inadequate investigations, leaving the condition undiagnosed for 13 years.
Clinical Examination and Imaging
On examination, the left nasal cavity appeared patent with no masses or polyps. However, the right nasal cavity revealed complete obliteration of the nasal vestibule due to adhesive tissue and fibrosis. A CT scan of the paranasal sinuses revealed a metallic foreign body with a characteristic “double ring sign” in the right nasal cavity, indicating the presence of a battery (Figure 1). The scan also showed obliteration of the nasal cavity extending from the vestibule to the inner nasal valve. No polyps, masses, or sinus involvement were noted.
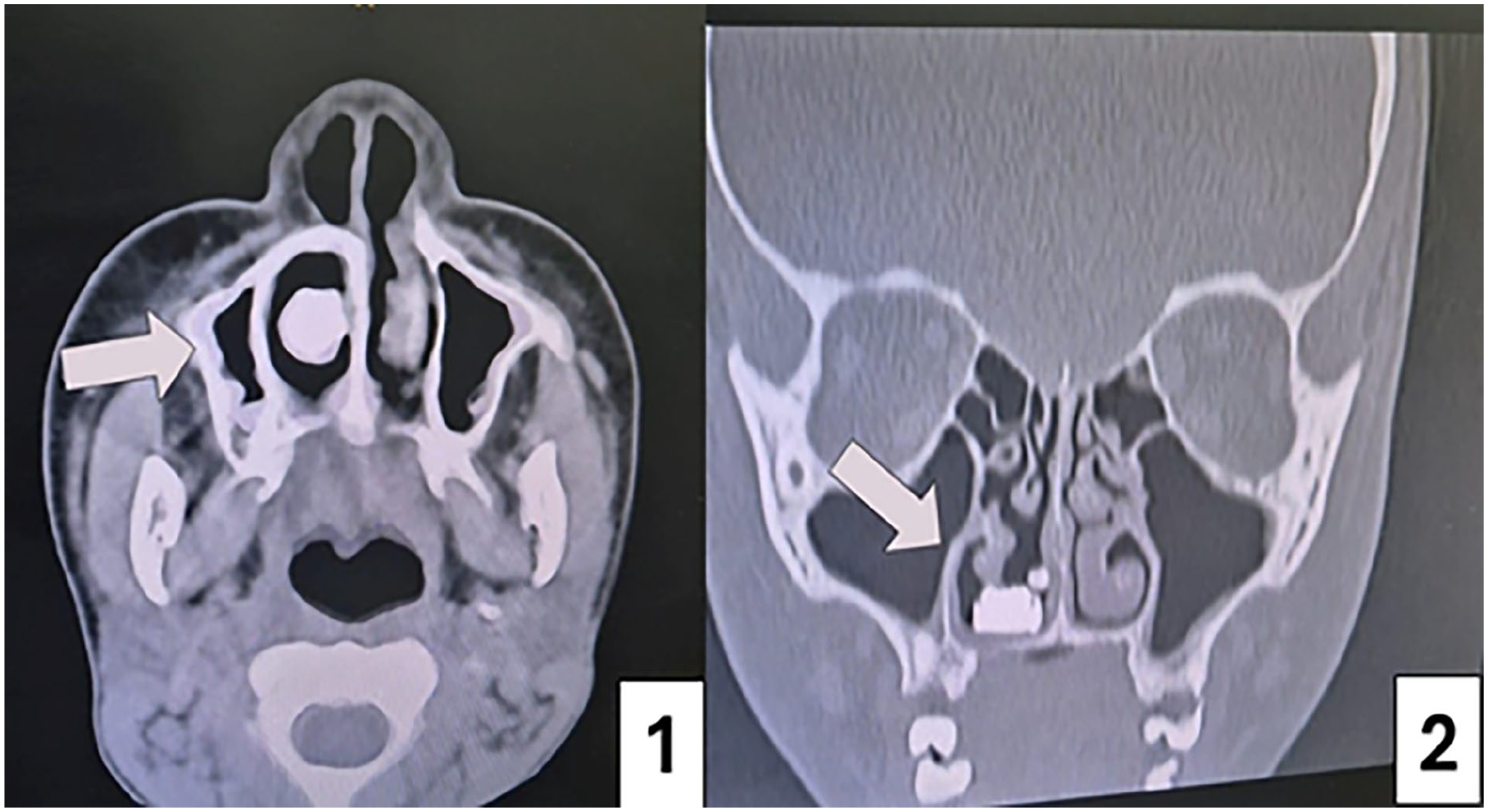
CT scan PNS. (1) Axial view illustrating the double-ring sign characteristic of a battery. (2) Coronal view of CT PNS, the retained battery in the right nasal cavity. PNS, paranasal sinuses.
Surgical Intervention and Postoperative Course
The patient underwent surgical intervention under general anesthesia. Intraoperative findings confirmed the presence of fibrosis and adhesive tissue at both the external and internal nasal valves. The obstructive tissue was meticulously dissected and removed to free the nasal skin and septum. A nasal endoscope was used to locate the battery, which was embedded on the floor of the right nasal cavity. The foreign body was successfully extracted, and bilateral nasal splints were applied to prevent the formation of synechia postoperatively.
At a 10-day follow-up, the splints were removed, and an endoscopic examination confirmed a patent right nasal cavity (Figure 2). Follow-ups at 3 and 6 months showed no synechia, and the nasal cavity appeared normal with no residual fibrosis or obstruction (Figure 2). The patient reported resolution of symptoms.
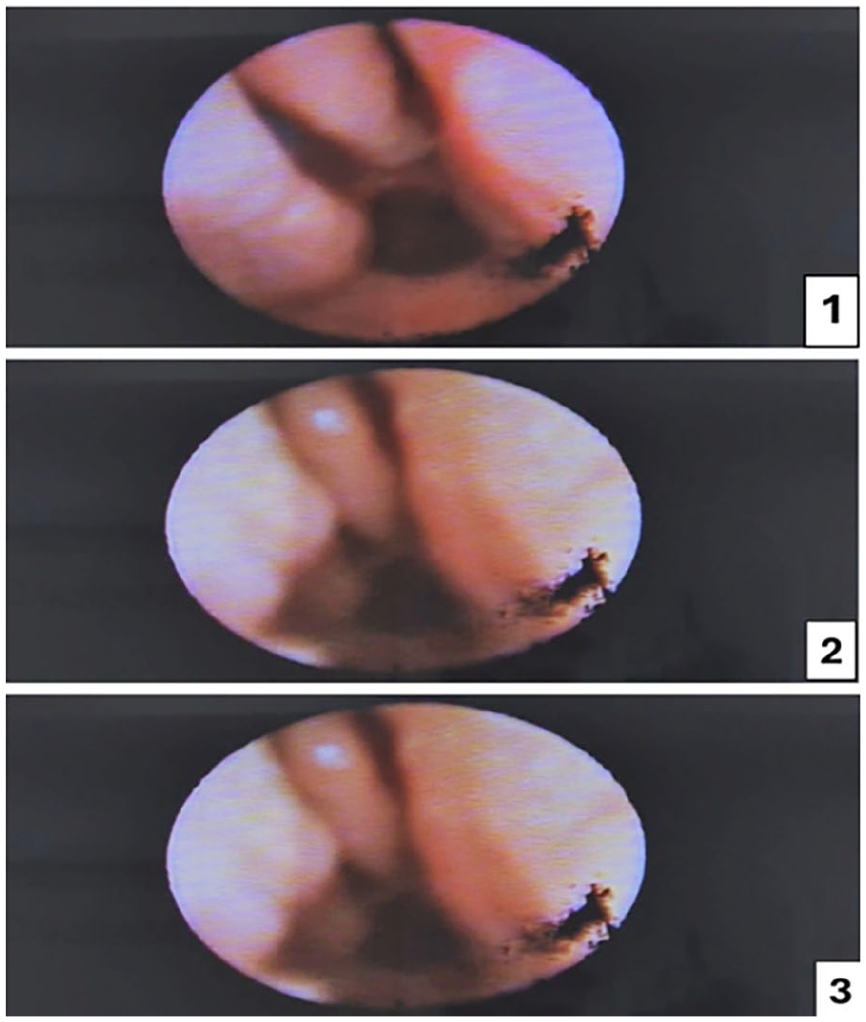
Postoperative rigid scope of the right nasal cavity. (1) Two-week postoperative rigid scope of the right nasal cavity. (2) Three months postoperative rigid scope of the right nasal cavity. (3) Six months postoperative rigid scope of the right nasal cavity.
Discussion
Neglected nasal foreign bodies, particularly button batteries, present a significant clinical challenge due to their potential for leakage, causing corrosive effects leading to rapid tissue damage, especially in delayed removal. Early diagnosis and intervention are critical to avoid severe complications requiring surgical treatment, including nasal deformities, infections, inflammation, tissue necrosis, and septal perforation.4,5 Proper imaging is recommended for accurate diagnosis and timely intervention to avoid serious outcomes.6,7
The literature underscores that button batteries, unlike inert objects, are hazardous due to their ability to generate an electrical current, leading to rapid tissue necrosis and chemical burns. Early intervention through prompt endoscopic removal is vital to minimize morbidity. Delayed diagnosis often occurs in asymptomatic cases or when immediate medical consultation is not sought. 8
In summary, nasal button batteries are a medical emergency requiring immediate removal to prevent irreversible tissue damage. Awareness among caregivers and clinicians regarding the dangers of button batteries is essential, along with strategies for early diagnosis.
Conclusion
This case underscores the importance of thorough evaluation and imaging in children with persistent nasal symptoms. Neglected foreign bodies, particularly batteries, can lead to long-term complications if not identified early. Foreign body retention should not be ruled out based on patient age alone, especially in cases of unilateral nasal obstruction. Timely surgical intervention and proper postoperative care are essential for restoring normal nasal function and preventing further complications.
Footnotes
Ethical Considerations
Institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Written informed consent was obtained from the patient’s parent/guardian for the publication of this case report and any accompanying images. The authors affirm that the patient’s identity has been protected and that all necessary steps have been taken to ensure anonymity.
Author Contributions
All authors substantially contributed to conception or design of the case reports. Mohammad Jalaladdin is the corresponding author, who was involved in drafting the case reports with assistance of Saud T. Alaidarous. Ahmed Althqafi and Alaa A. Babkour were involved in revising the manuscript. All authors have approved the final version prior to submission.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials. Further information can be obtained from the corresponding author upon reasonable request.