
Abstract
Objectives:
There have been few studies on slightly-asymmetric sensorineural hearing loss (SASHL), and no study to date has reported on the longitudinal development of early-auditory ability in children with SASHL and wearing hearing aids (HAs). Thus, we explored the developmental trajectory of early-auditory ability of children with SASHL who wear HAs, and compared the differences in different types of SASHL (the mild-moderate, moderate-severe, and severe-profound).
Methods:
We performed a prospective, longitudinal study of 31 children with SASHL who were followed for 18 months. Their early-prelingual auditory development (EPLAD) was evaluated using the Infant-Toddler: Meaningful Auditory Integration Scale (ITMAIS), before wearing HAs and at the 1st, 3rd, 6th, 12th, and 18th month after implementing HAs. A spline function was implemented to describe the observed EPLAD trajectory. A cubic polynomial regression model was used to predict the change in the ITMAIS score over time, and nonparametric tests or the chi-squared test was used to compare differences between groups.
Results:
ITMAIS scores were statistically-significantly different between all subsequent follow-ups (P < 0.001). We constructed a highly-accurate predictive score of ITMAIS over time (r2 = 0.99) and show that sound detection was always faster than sound recognition. The EPLAD score of the severe-profound group was always lower than those of the moderate-severe group and the severe-profound group (P < 0.05).
Conclusions:
The EPLAD trajectory of the SASHL children was steepest during the first month after HA fitting and leveled-off gradually thereafter. The more severe the degree of hearing loss, the slower the EPLAD rate, which emphasizes the importance of early intervention. We recommend further longitudinal studies to elucidate the dynamics of the process and individual differences in early-childhood hearing ability.
Keywords
Introduction
Around 466 million people worldwide have disabling hearing loss. Of these, 34 million are children, with ~1 in 1000 newborns suffering from hearing loss. Different degrees of hearing loss between bilateral ears are encountered daily by clinical audiologists. Binaural hearing is very important for the development of normal auditory processing. However, the definition of asymmetric hearing loss (AHL) is not sufficiently clarified in audiology. AHL is a very broad term used to describe any grade of interaural asymmetry in hearing acuity. According to a round table discussion, Vincent et al defined interaural asymmetry as a difference of 30 dB hearing loss (HL) or more among pure-tone average (PTA) thresholds for 4 frequencies (ie, 0.5, 1, 2, and 4 kHz) in each ear, with >30 in the better ear and ≥60 dB HL in the poorer ear. 1 Different reports have used different definitions of AHL.2-5 Typically, one study has focused on extreme cases, termed single-sided deafness or those requiring lateral cochlear implants. 1
For some children with sensorineural hearing loss, bilateral hearing may be only-slightly asymmetrical. Slightly-asymmetric sensorineural hearing loss (SASHL) mainly refers to the degree of bilateral hearing loss distributed at different and adjacent levels, such as hearing loss that is moderate on one side and severe on the other. While extensive research exists on extreme AHL (such as single-sided deafness) and symmetric hearing loss, children with SASHL represent a distinct clinical population that warrants specific investigation. We hypothesize that children with SASHL may demonstrate unique patterns of early-prelingual auditory development (EPLAD) when wearing hearing aids (HAs) compared with those with symmetric hearing loss. This difference likely stems from the unique impact that slight interaural asymmetry has on central auditory system development, potentially resulting in different rehabilitation outcomes and developmental trajectories.
HAs provide marked benefits to deaf children, but rehabilitation assessment after HA fitting is also very important. Most previous studies in this context were cross-sectional, lacking longitudinal follow-up, and thus could not reveal development of the individual in real life. In addition, many previous studies have focused on auditory skills and speech behavior in pediatric unilateral hearing loss (UHL). For example, Purcell et al suggested that personal hearing devices should be included in management protocols for children with UHL aged 5 to 19 years. 6 Only few longitudinal studies have focused on the long-term follow-up of children wearing HAs. Similarly, a German study, recruited 32 children with UHL at a mean age of 5.5 years, found that UHL in children improved the auditory skills after wearing HAs for 2 years. 7 Despite recent advances in understanding various hearing loss profiles, a significant research gap exists regarding SASHL children. The clinical characteristics and intervention outcomes of these children may differ from both symmetric hearing loss and extreme AHL cases, potentially placing them on a unique developmental continuum. The absence of longitudinal data on SASHL specifically limits our ability to provide evidence-based clinical guidance for this distinct population.
Although recent studies have begun to focus on children with UHL, no longitudinal follow-up studies on EPLAD of SASHL children wearing HAs have been reported. Therefore, this study aimed to (1) investigate children with SASHL as a distinct clinical population; (2) assess the EPLAD of children with SASHL wearing HAs quantitatively and longitudinally rather than cross-sectionally, and (3) develop a predictive function for EPLAD progression based on the 18 month follow-up data.
Materials and Methods
Subjects
This was a prospective, longitudinal cohort study. This study mainly included children with SASHL, who were fitted with HAs in the West China Hospital of Sichuan University, from January 2016 to January 2017. The hearing threshold was equal to the average value of PTA at 500, 1000, 2000, and 4000 Hz, and the degree of hearing loss was according to the hearing classification standard of WHO. 8 The degree of hearing loss in children may range from mild to profound: 26 to 30 dB HL is mild, 31 to 60 dB HL is moderate, 61 to 80 dB HL is severe, and over 81 dB HL is profound. 8 Inclusion criteria were as follows: sensorineural hearing loss that was asymmetric in the bilateral ears; the degree of hearing loss on both sides was distributed only at 2 adjacent classification levels (mild-moderate; moderate-severe; severe-profound), with a minimum threshold difference of >5 dB between the 2 ears; both ears wore HAs regularly; the unaided hearing threshold of these children showed no marked fluctuation (not exceeding 10 dB HL) during the follow-up period of 18 months. Exclusion criteria were as follows: middle-ear or inner-ear malformation; auditory neuropathy; acoustic neuroma; otitis media; aged over 5 years; and/or developmental abnormalities in terms of intelligence and cognition.
The children were followed up at 5 different time points. To ensure the validity of the data, we only allowed 1 missed follow-up. Due to the difficulty of collecting long-term longitudinal data and of follow-up, we finally included 31 subjects for analysis. According to the type and degree of hearing loss, these children were divided into 3 groups: the mild-moderate group, the moderate-severe group, and the severe-profound group (Figure 1).
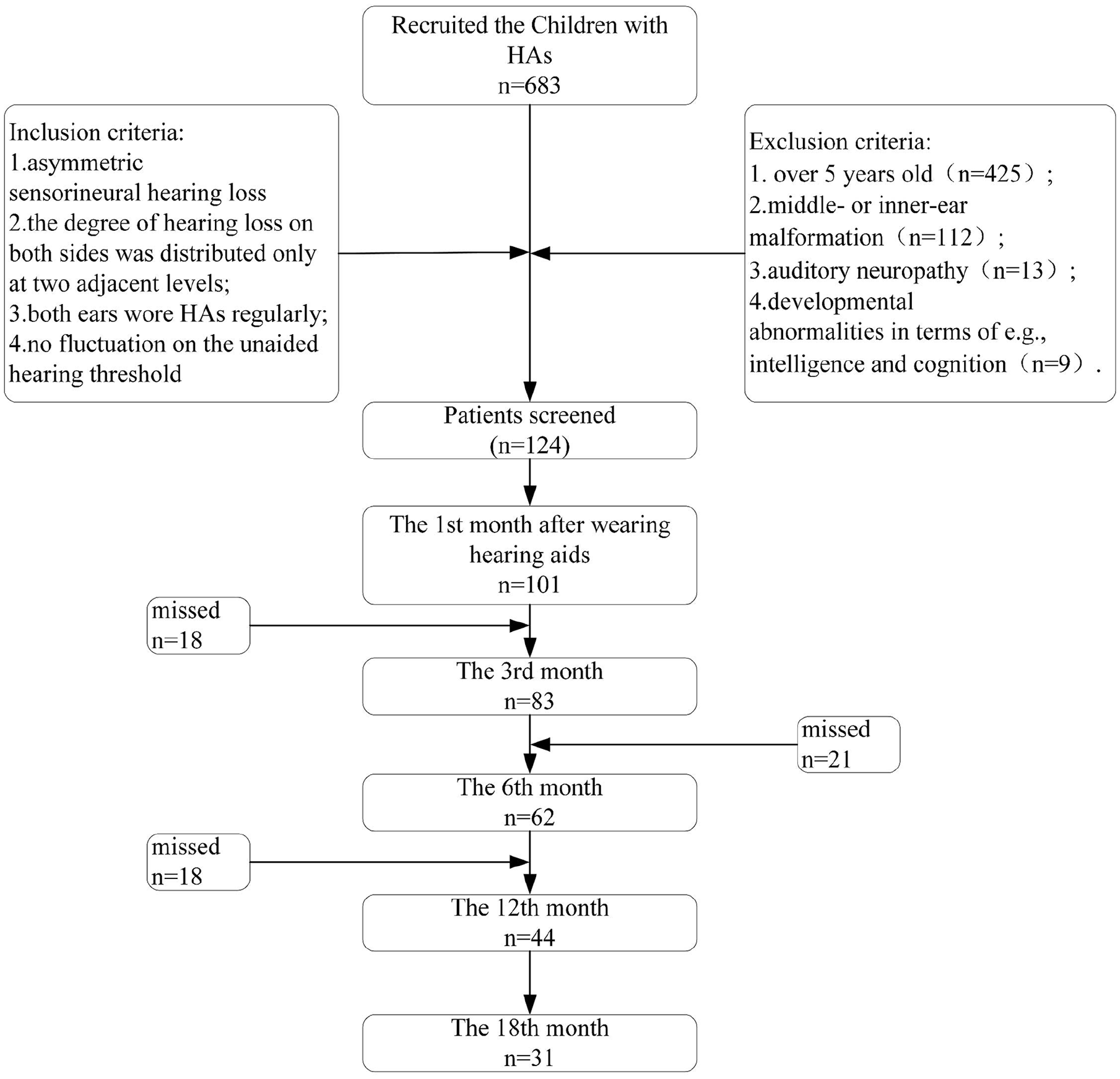
Process of collecting subject data.
Evaluation of EPLAD
Auditory ability assessments relied mainly on the Infant-Toddler: Meaningful Auditory Integration Scale (ITMAIS). This is a structured questionnaire, which contains 10 questions scored on a scale of 0 to 4 points each, with a total possible score of 40 points. The raw scores were converted to percentages [(actual score/40) × 100%] for easier interpretation. Higher ITMAIS percentage scores indicate better auditory integration abilities, with higher scores reflecting better sound detection and recognition capabilities. Among the 10 questions, 3 to 6 questions are used to evaluate children’s ability to detect sound, and 7 to 10 questions are used to evaluate children’s ability to recognize sound. We tested the EPLAD of these children before fitting HAs and at the 3rd, 6th, 12th, and 18th month after fitting HAs.
Hearing Test
For children under 0.5 years of age, we used behavioral observation audiometry, for children between 0.5 and 2.5 years, we used visual reinforcement audiometry, and for children between 2.5 and 6 years, we used conditioned play audiometry.
HA Fitting
When fitting children’s HAs, the real ear coupling cavity difference measurement was used to evaluate their hearing gain. The instrument used is FONIX 6500 Real Ear Analyzer (Frye Electronics, Tigard, OR, USA), and the testing process included system setup, coupling cavity measurement, and real ear measurement.
Statistics Analysis
To compare the differences among the 3 groups, analysis of variance or Kruskal-Wallis H tests were conducted according to the normality of continuous variables. For classified variables, if the theoretical frequency exceeded 5, Pearson’s chi-squared test was conducted; otherwise, Fisher’s exact test was used. Paired t-tests were used to compare the difference in the hearing threshold and EPLAD before and after HA implementation. Since ITMAIS scores were collected as repeated measurements over time, we applied mixed analysis of variance with repeated measures and used the Bonferroni correction to adjust the significance level. The overall trend in the ITMAIS, sound detection, and sound recognition scores was described as a smooth curve using a spline function. A cubic polynomial regression model was used to predict the change in the ITMAIS score over time. For all comparisons, 2-sided tests were applied with P < 0.05 considered the threshold for statistical significance. All statistical analyses were performed, and graphs drawn using R Studio 7.0 (R Studio PBC, USA) and Prism version 8.0 (GraphPad Software Inc., USA).
Results
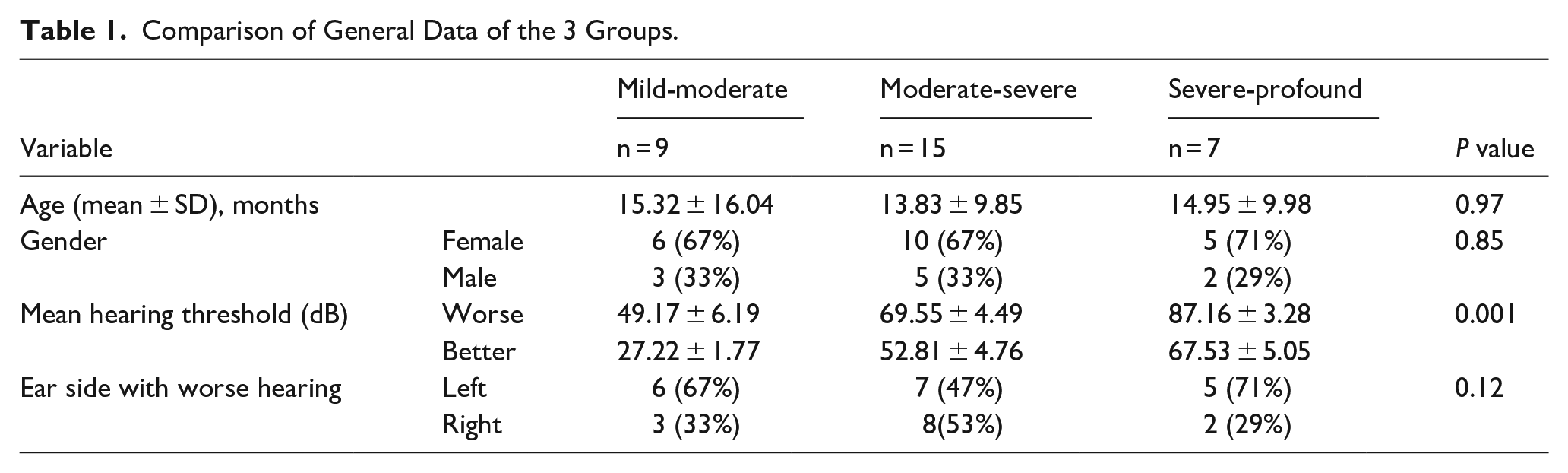
In this study, we included 31 subjects (10 male and 21 female). Their mean age at the fitting of the HAs was 14.45 ± 11.65 months, while their mean hearing threshold was 61.45 ± 16.71 dB HL in the left ear, and 57.61 ± 18.07 dB HL in the right ear. When analyzed by better and worse ear, significant differences were observed among the 3 groups (P = 0.001). For the mild-moderate group, the mean thresholds were 49.17 ± 6.19 dB in the worse ear and 27.22 ± 1.77 dB in the better ear. The moderate-severe group showed thresholds of 52.81 ± 4.76 dB in the better ear and 69.55 ± 4.49 dB in the worse ear, while the severe-profound group had 67.53 ± 5.05 dB in the better ear and 87.16 ± 3.28 dB in the worse ear. The mild-moderate group, the moderate-severe group, and the severe-profound group did not differ significantly in age, sex, and which ear had the worse hearing (P > 0.05; Table 1).
Comparison of General Data of the 3 Groups.
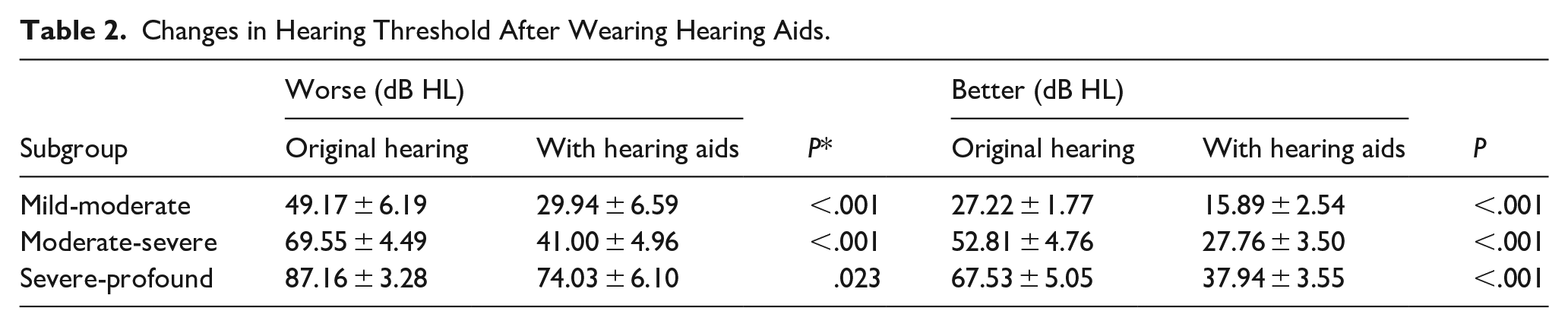
HAs significantly improved the hearing threshold of all 3 groups (P < 0.05). Details are shown in Table 2.
Changes in Hearing Threshold After Wearing Hearing Aids.
The EPLAD of the 3 groups increased continuously over the 18 months of wearing HAs. There was a trend for an initial rapid increase, which was then followed by a slow gradual approach to the maximum score. The milder the hearing loss, the higher trajectory of the EPLAD score. We optimized the models of the development curves of the mild-moderate group, the moderate-severe group, and the severe-profound group (r2 = 0.99; Figure 2). We also used a spline function to generate 3 groups of sound detection and sound recognition development trajectories and found that sound detection was always more accurate than sound recognition. The more severe the hearing loss, the lower the trajectory of sound detection and sound recognition. For the mild-moderate and severe-profound groups, the slope was actually steeper for sound recognition than for sound detection (Figure 3).
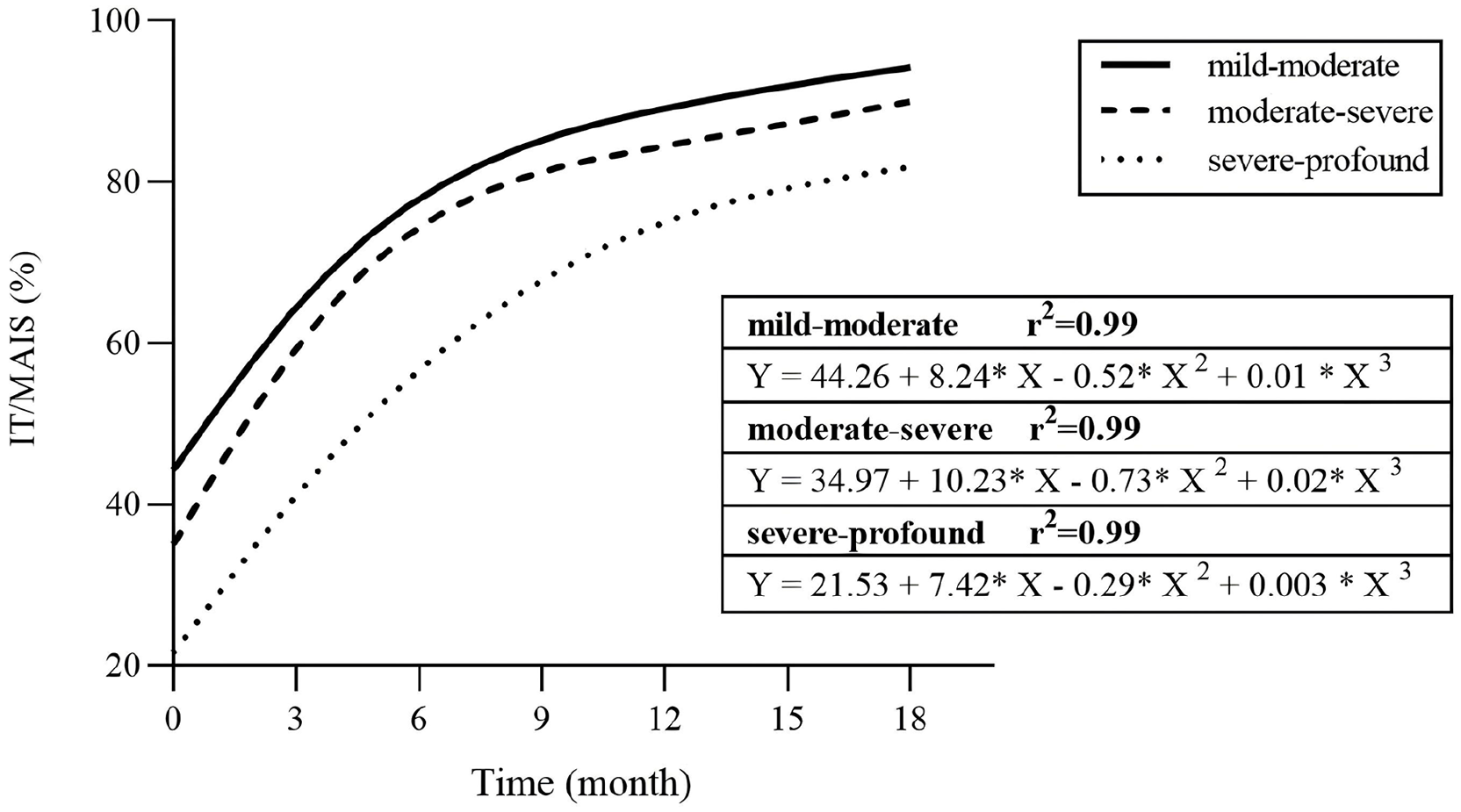
ITMAIS score changes over time for children with different degrees of hearing loss. ITMAIS percentage scores over 18 months after hearing aid fitting for children with mild-moderate, moderate-severe, and severe-profound SASHL. All groups showed improved auditory integration abilities over time, with the mild-moderate group achieving the highest scores. Third-order polynomial regression models (r² = 0.99) demonstrate excellent fit for the developmental trajectories in each severity group. ITMAIS, Infant-Toddler: Meaningful Auditory Integration Scale; SASHL, slightly-asymmetric sensorineural hearing loss.
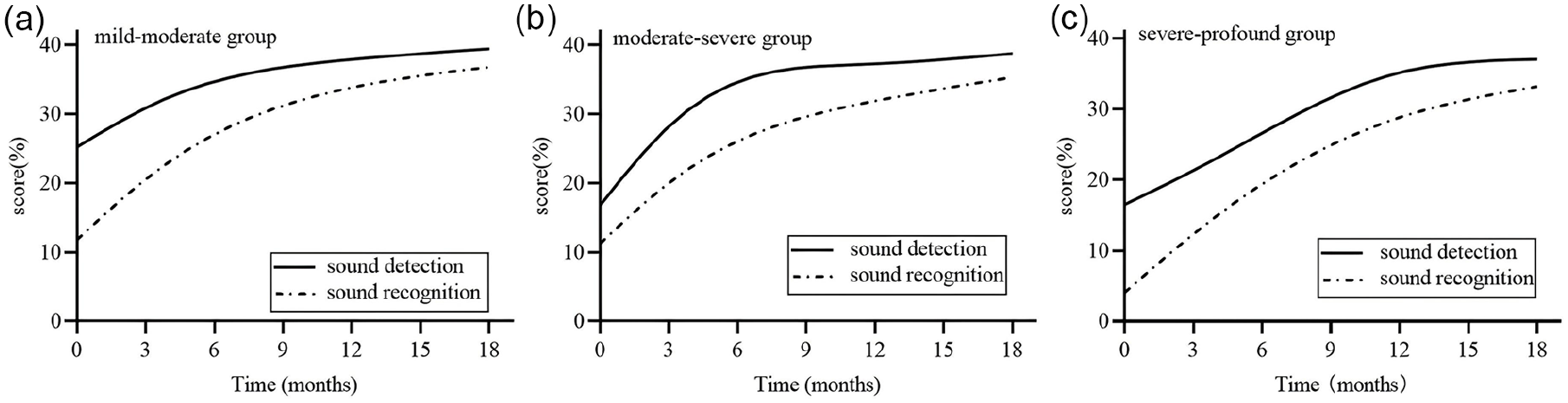
Changes in sound detection and recognition abilities over time in children with different degrees of hearing loss. This figure shows the changes in sound detection (solid line) and sound recognition (dashed line) abilities over 18 months after hearing aid fitting in children with mild-moderate (a), moderate-severe (b), and severe-profound (c) SASHL. Sound detection abilities were superior to sound recognition abilities in all 3 groups, and both abilities improved continuously over time. SASHL, slightly-asymmetric sensorineural hearing loss.
The ITMAIS score of the mild-moderate group, the moderate-severe group, and the severe-profound group at the fifth follow-up is shown in Table 3. There were significant differences among the 3 groups (P < 0.001). We also found that HAs significantly promoted moderate-severe group’s EPLAD, which had lagged significantly behind that of the mild-moderate group before HA fitting (P < 0.05). During the continued follow-up, there were no significant differences in the EPLAD of these groups (P > 0.05), although the EPLAD score of the severe-profound group was always lower than that of the other 2 groups (P < 0.05; Table 3 and Supplementary Figure 1).
ITMAIS Scores (Mean ± SD) in the 3 Groups at Different Follow-Up Times.
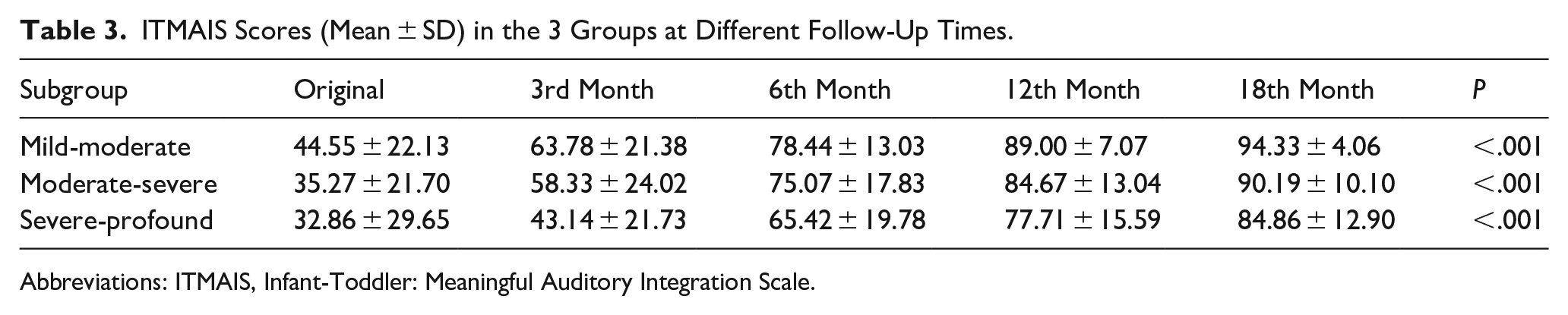
Abbreviations: ITMAIS, Infant-Toddler: Meaningful Auditory Integration Scale.
Discussion
Among the various types of hearing loss, AHL is a frequent audiometric finding, and deciding which definition of asymmetry is the most clinically meaningful requires careful consideration. 5 The impact of AHL on the developing auditory system and on speech recognition and perception have often been underestimated. While recent studies have increasingly focused on children with UHL, there is no standardized definition of SASHL and the speech and language development of children with SASHL who had been fitted with HAs remain unstudied. As prospective, longitudinal cohort studies can demonstrate individual differences and trends in development more clearly, we sought to provide evidence of the EPLAD of children with SASHL within 18 months after intervention to treat hearing impairment with HAs. We sought to identify changes in early-prelingual auditory ability and in the development of early speech and language. We found statistically-significant improvements in the hearing threshold in both ears for all groups, between original and aided hearing. This study specifically focused on SASHL rather than symmetric hearing loss because children with SASHL present a unique clinical profile that requires more specialized investigation. Compared with symmetric hearing loss, SASHL poses distinct challenges to auditory processing, such as unbalanced binaural input, which may lead to reorganization of central auditory pathways. These physiological impacts may potentially influence the outcomes of HA intervention differently compared with those with symmetric hearing loss. Moreover, clinical practice has shown that SASHL is more often overlooked or mismanaged due to being perceived as less severe than UHL or profound hearing loss, despite the potential for long-term effects on speech and auditory development. Therefore, our study aimed to address these knowledge gaps and provide data specific to this underexplored population.
Early intervention with HAs can provide adequate benefit to children with SASHL. Recent studies in animal models of deafness9,10 and in children with different hearing loss11-13 consistently showed that AHL in early childhood reorganizes the developing auditory pathways toward the hearing ear, with weaker central representation of the deaf ear. Delayed therapy consequently compromises benefit for the deaf ear, with slow rates of improvement measured over time. Therefore, asymmetric hearing needs early identification and intervention. Early-auditory stimulation underpins the development of binaural hearing skills 14 and language development. 15 Better language has been associated with better speech perception. 16 Speech cannot be understood if it cannot be heard. Therefore, higher audibility would be expected to be associated with better performance outcomes. To date, treatment approaches for UHL range from “watchful waiting” to hearing rehabilitation by means of a variety of hearing devices, depending on the children’s age, degree, and type of hearing loss, and listening environment. 14 The most common auditory prosthetic is the HA, which primarily amplifies sound so that it becomes audible to the impaired ear and has the potential of providing bilateral stimulation. 14 It has been widely accepted that provision of amplification is a crucial component of early intervention for children with permanent childhood hearing loss. 17 HAs can better compensate low-frequency sound information and provide basic hearing. In a study, behavior indicative of EPLAD, as measured with the ITMAIS, has been found to provide evidence of the benefit of using HAs in early-intervention programs. 18 The use of HAs had a significant positive effect on auditory ability in children with mild-moderate, moderate-severe, and severe-profound hearing loss, including their aided sound-field thresholds and EPLAD.
It is most important to note the pattern of EPLAD pediatric subjects with SASHL after HA fitting. In our study, 3 groups exhibited increases in the ITMAIS score at the 3rd, 6th, 12th, and 18th month after hearing-aid fitting, regardless of the severity of hearing loss, in which the largest statistically-significant improvements were seen in the first 6 months for all groups. In other words, within 6 months, children achieved a better level of EPLAD than at baseline, regardless of the severity of their hearing losses. HAs could facilitate EPLAD in these children with SASHL during the early period after intervention. The same pattern of results had been seen in previous studies for groups of children with binaural hearing losses. Likewise, Gang et al reported that the EPLAD of profound sensorineural hearing-impaired children fitted with HAs at the age of 1 to 2 years improved significantly within the first 0.5 year after HA fitting. 19 In the study by Zheng et al, 18 among 45 pediatric patients initially fitted with HAs between the ages of 1 and 5.5 years, both moderate-severe and profound hearing loss groups exhibited statistically-significant increases in EPLAD within 6 months of HA fitting. The trajectory of each of the 3 groups in our study was steepest during the early months after fitting and leveled-off gradually during later months. After a few months the trajectories began to approach different asymptotic values, indicating a “ceiling effect,” in which the EPLAD did not improve any more. This may be related to the limitations of the ITMAIS.
Taken together, the EPLAD trajectory after fitting HAs appeared to be highly similar to that after early-cochlear implantation. 18 Regardless of the differences across hearing loss of different severities, 18 months after HA intervention, recipients reached an average EPLAD score of about 80%, approximately the score achieved by an 18 month-old child with normal hearing. 20 These observations suggest that the auditory input provided by HAs is adequate to facilitate EPLAD. Moreover, comparing 3 groups of children showed that those with a less severe hearing loss had more rapid auditory development (steeper slopes), while children with more severe hearing loss had slower auditory development (shallower slopes). We also derived predictive function for the 3 groups (Figure 2), with an r2 value of 0.99, which indicated that the prediction efficiency was excellent.
A recent study also concluded that the ITMAIS could be used as a measure of EPLAD for initial classification of the severity of hearing loss in children. 21 The ITMAIS scores that define EPLAD trajectories would necessarily increasing at different rates, depending on the severity of the hearing loss, before reaching different asymptotic values. All these developmental trajectories fit a logarithmic regression function. Pairwise comparison of the early-auditory ability of the 3 groups at different times showed no statistically-significant difference, except for a baseline difference between the mild-moderate and moderate-severe groups. These 2 groups also had similar trajectories of ITMAIS score. However, statistically-significant differences in the EPLAD were seen between the moderate-severe and severe-profound groups at baseline and at each of the follow-up time-points after initial fitting. This indicated that the benefit obtained from HAs by the former 2 groups was similar and greater than that obtained by children in the severe-profound group. These results also showed how the severity of hearing loss treated with HAs affects EPLAD. These findings have several potentially-useful practical consequences for the clinical management of young children after early-HA intervention. HAs could improve the EPLAD of pediatric SASHL patients, particularly those with mild-moderate and moderate-severe SASHL. This finding is in accordance with very recent research, which showed that, although both cochlear implants and HAs could improve EPLAD of profoundly-deaf children, the EPLAD of children who received cochlear implants improved faster in the first year after intervention. 22 It is worth noting that although the developmental trajectory of SASHL children shares similarities with children with symmetric hearing loss in previous studies (eg, exhibiting improvements in early-auditory development within months of HA fitting), children with SASHL may experience unique rehabilitation challenges due to the lack of balanced auditory input. Our findings highlight the need for early-targeted interventions in this group to maximize auditory and speech development outcomes.
The results are reported for the ITMAIS 4-item sound-detection scale and the 4-item sound-recognition and sound-discrimination scale. Figure 3 displays the trajectory of sound detection and recognition scores of children with mild-moderate, moderate-severe, and severe-profound hearing loss. The developmental trajectories for each of the scales fit the logarithmic regression equations equally well. The behaviors described by the detection scale exhibited the most rapid development. The behaviors comprising the sound-recognition scale are more complex, and include meaningful recognition and discrimination of sounds, which developed more slowly. We found that the detection of and responsiveness to sound precedes meaningful recognition and discrimination of sound, similar to children with cochlear implants. 23 Moreover, the more severe the hearing loss, the slower the development of detection and recognition of sound. When these 2 scales are combined to produce the overall ITMAIS score, the developmental trajectory fits a logarithmic regression function that reaches its maximum at some months of age well. This implies that these children with SASHL will always detect and respond spontaneously to sounds and will always recognize and discriminate meaningful sounds. Previous research has shown that EPLAD and early-speech recognition are 2 different auditory abilities, which are thought to be interrelated hierarchically, with EPLAD preceding early-speech recognition. 24 A previous study found that nonverbal IQ and language abilities were significant predictors of speech recognition in babble in children using HAs, with the effect size of speech ability almost double that of nonverbal IQ. 25 These findings lend support to the importance of focusing on speech recognition development by early intervention.
Conclusion
The EPLAD trajectory of children with SASHL was steepest during the early months after HA fitting and leveled off gradually during subsequent months. The more severe the degree of hearing loss, the slower the development of EPLAD. These findings have practical implications for the clinical management of young children with SASHL and suggest that HA intervention could improve the sound perception of pediatric SASHL patients sufficiently to benefit EPLAD.
Supplemental Material
sj-jpg-1-ear-10.1177_01455613251345683 – Supplemental material for Longitudinal Study on Early-Auditory Development in Children Who Have Slightly-Asymmetric Hearing Loss and Are Wearing Hearing Aids
Supplemental material, sj-jpg-1-ear-10.1177_01455613251345683 for Longitudinal Study on Early-Auditory Development in Children Who Have Slightly-Asymmetric Hearing Loss and Are Wearing Hearing Aids by Xiao-yun Zhang, Wei-li Kong and Ning-ying Song in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
We thank Dao-hong Meng, Professor of Public Health and Epidemiology in University of South Florida, for his suggestion on the study and discussion of the results. We also thank Dong-yang Yang, Department of Biostatistics at Dalla Lana School of Public Health, University of Toronto, for her contribution on the data analysis.
Ethical Considerations
The study adhered to the principles of the Helsinki Declaration and received approval from the Medical Ethics Committee of West China Hospital (approval number 2016-167).
Consent to Participate
The informed consent was provided by the parent/guardian.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data presented in this study can be obtained from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.