
Abstract
Introduction:
Posttraumatic spondylodiscitis is an uncommon but serious complication of spinal trauma. It may lead to severe neurological impairment and systemic infection. Retropharyngeal abscess (RPA), typically associated with upper respiratory infections, is rarely reported as a complication of nontuberculous spondylodiscitis, especially in the context of cervical trauma. This rare association poses a dual threat: airway obstruction and spinal cord compression. Our work aimed to report a rare case of posttraumatic, nontuberculous cervical spondylodiscitis complicated by an RPA, leading to both respiratory and neurological compromise, and to highlight the importance of early multidisciplinary management.
Observation:
We present the case of a 45- year-old male with posttraumatic dorsal and cervical spondylitis following a road traffic accident. He developed progressive paraplegia and respiratory distress. Imaging revealed multilevel vertebral involvement with spinal cord compression and an RPA. The first transoral drainage was ineffective, and the recurrence within 48 hours necessitated a second external surgical approach. Cultures identified methicillin-resistant Staphylococcus aureus and Klebsiella pneumoniae. Broad-spectrum antibiotics and intensive care management led to gradual improvement.
Conclusion:
This case underlines the complexity and severity of posttraumatic spondylodiscitis with RPA. Prompt diagnosis and a multidisciplinary therapeutic strategy are vital to prevent life-threatening complications and improve patient outcomes.
Highlights
Rare association: This case describes an unusual combination of posttraumatic multilevel spondylodiscitis and retropharyngeal abscess (RPA) in an adult patient—an association seldom reported in the literature.
Life-threatening complications: The dual pathology posed a critical threat to both neurological function (due to spinal cord compression) and airway patency (from RPA expansion).
Diagnostic challenge: Early diagnosis was complicated by the delayed presentation and overlapping symptoms, emphasizing the need for high clinical suspicion in posttrauma patients with infection signs.
Multidisciplinary management: The patient required combined neurosurgical and ENT interventions, highlighting the importance of coordinated care in complex spinal infections.
Surgical complexity: Initial transoral drainage of the abscess failed, necessitating a second, external approach, underscoring that deep neck space infections of spinal origin may not respond to conventional drainage strategies.
Introduction
Posttraumatic spondylodiscitis is a serious complication that rarely occurs following spinal trauma, leading to severe neurological and infectious outcomes. The condition may result from hematogenous bacterial spread or directly from trauma, and infections can originate from distant sites or be secondary to surgical interventions. Staphylococcal species are among the most implicated pathogens. 1
Retropharyngeal abscesses (RPAs) secondary to spondylodiscitis are rare and most commonly occur in the context of tuberculosis. Their occurrence following cervical spine trauma is exceptional and represents a potentially-life-threatening condition if not promptly diagnosed and treated. While RPAs are typically associated with upper respiratory tract infections, their development in the setting of posttraumatic, nontuberculous infectious cervical spondylodiscitis is exceedingly rare in adults. This unusual association remains anatomically plausible due to the proximity between the cervical spine and the retropharyngeal space.
This dual pathology presents a complex clinical challenge: on the one hand, the risk of neurological compromise due to spinal cord compression, and on the other, the threat of airway obstruction from the abscess, with potential for mediastinal extension. Management in such cases is particularly demanding. Indeed, simple abscess drainage—usually sufficient in ENT-related infectious RPAs—may be inadequate due to the infection’s distinct pathophysiology and deeper origin.
We present the case of a multilevel posttraumatic spondylitis complicated by spinal cord compression resulting in paraplegia and associated with a parapharyngeal abscess that led to acute respiratory distress. The distress recurred after initial transoral drainage, underscoring the need for a comprehensive multidisciplinary approach involving neurosurgical, otolaryngological, and infectious disease expertise. This case report highlights the critical importance of early diagnosis and comprehensive management in preventing irreversible neurological damage and systemic complications.
Case Presentation
A 45- year-old male patient, known to be a hepatitis B carrier, was involved in a road traffic accident resulting in multiple traumatic injuries. The initial assessment revealed craniofacial fractures, comprising lung contusions, rib fractures, and a 40 × 20 mm prevertebral hematoma secondary to fractures at the D7 to D9 levels.
Initially, the patient was admitted to the neurosurgery department for observation. After 3 days of clinical stability, he was discharged. However, he returned 3 days later presenting with confusion, a fever of 38.8°C, paraplegia, urinary incontinence, and respiratory distress with oxygen saturation at 92%. His lactate level was elevated (2.15 mmol/L), prompting emergency imaging.
A brain computed tomography (CT) scan showed a left basifrontal hypodensity likely related to posttraumatic changes and a 30 × 18 mm retropharyngeal collection at the C3 to C4 level. Spinal MRI confirmed compression fractures at D7 to D9 with <50% height loss, a right paravertebral hematoma extending from D7 to D9 with spinal cord compression, and a retropharyngeal hematoma (Figure 1).
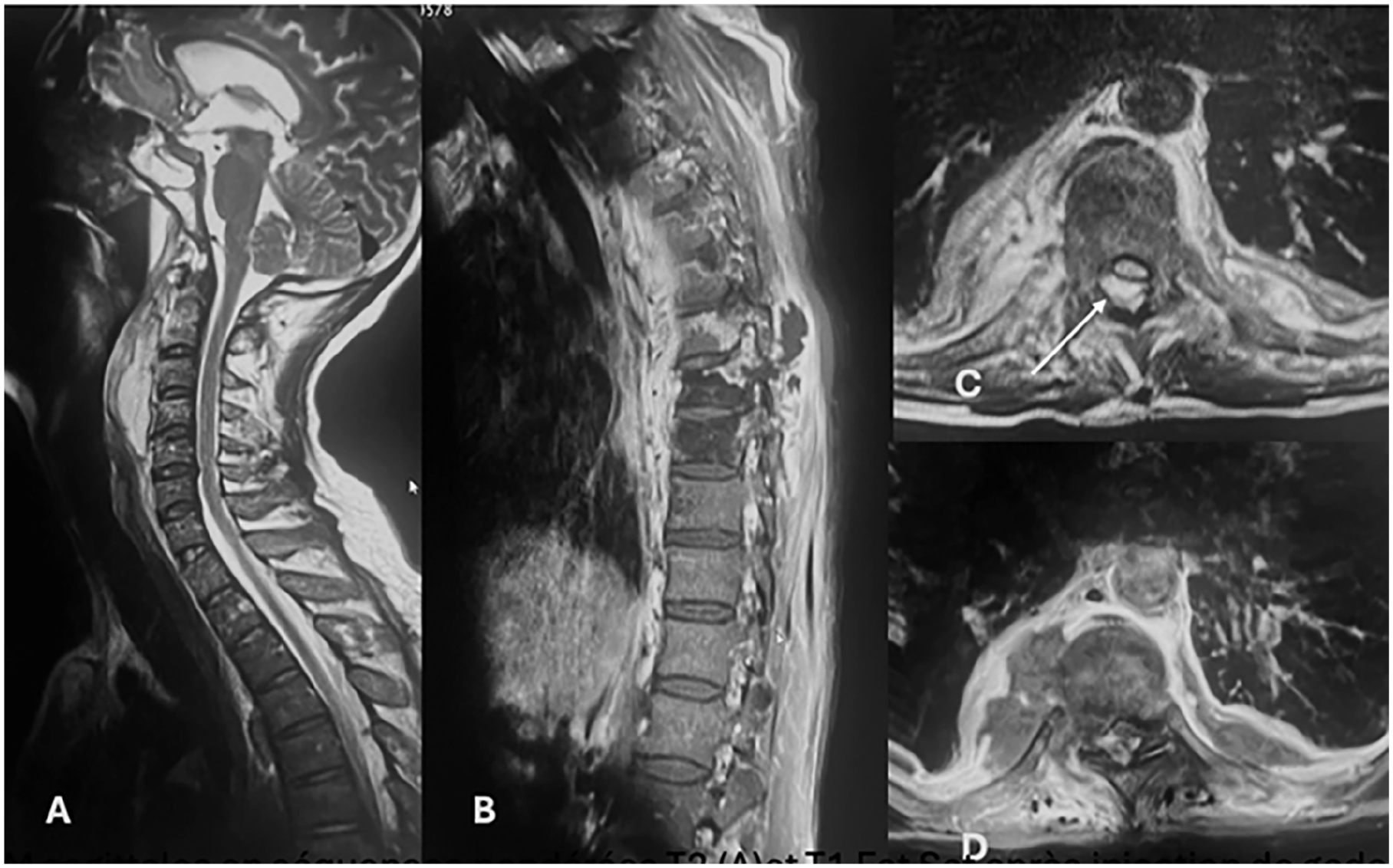
Sagittal and axial MRI images in T2-weighted sequences (A, C) and T1 Fat-Sat sequence after gadolinium injection (B, D): A retropharyngeal fluid collection extending from C2 to C5 (A), consistent with a retropharyngeal abscess. Thoracic spondylodiscitis at D8 and D9 with vertebral body abscesses (B), bilateral paravertebral abscesses (C, D), and intra-canal epidural extension (arrow in C) causing spinal cord compression.
Given the neurologic deterioration, urgent spinal decompression was performed with evacuation of an infected hematoma and a laminectomy from D7 to D10. Pus was collected for microbiological analysis. The patient was transferred to the intensive care unit, intubated, and ventilated. Empirical antibiotic therapy with imipenem (1 g IV every 6 hours) and vancomycin (4.25 g/day) was initiated due to suspected meningitis. He was extubated on the first postoperative day with a Glasgow Coma Scale score of 15 but exhibited persistent paraplegia with flaccid paralysis below D10 and partial sensory recovery consistent with ASIA grade A at T12.
Blood cultures identified methicillin-resistant Staphylococcus aureus, confirming bacteremic spondylitis. The antibiotic regimen was adjusted to include rifampicin (600 mg twice daily) in combination with vancomycin. The patient subsequently developed respiratory distress characterized by noisy, spontaneous breathing and dysphagia. Clinical and radiological assessment concluded to an increase in size of the RPA, which has become compressive on the oropharyngeal airway (Figure 2). A transoral incision and drainage were performed, and microbiological cultures identified Klebsiella pneumoniae. However, the abscess recurred 48 hours later, necessitating a second surgical drainage via a cervicotomy approach. A drainage tube was inserted, and targeted antibiotic therapy with colistin and fosfomycin was administered. The patient gradually improved following thoracoscopic drainage of a right parietal collection and was successfully weaned off oxygen therapy (Figure 3).

Second preoperative cervical spine MRI T2 Short TI Inversion Recovery (STIR) image showing increase in size of the retropharyngeal abscess, which has become compressive on the oropharyngeal airway and appearance of a hypersignal of the fourth cervical vertebral body in favor of infectious spondylitis.
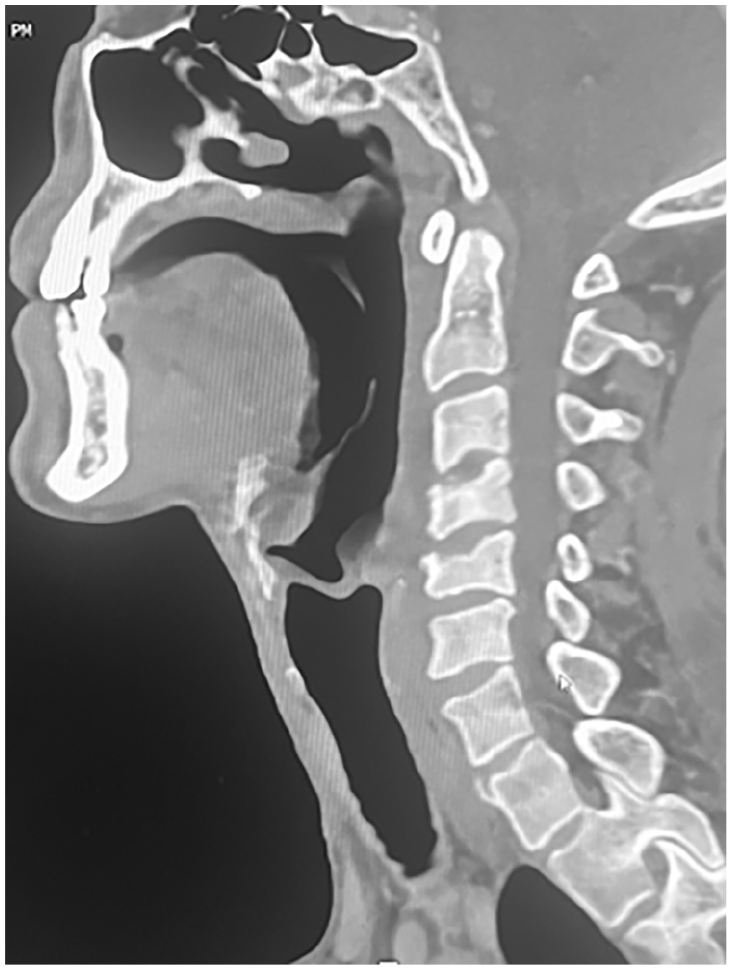
Postoperative cervical spine CT bone window image showing the destruction of the upper vertebral endplates of the fourth and fifth cervical vertebrae following infectious spondylitis.
Clinical and laboratory indicators progressively improved, with defervescence, normalization of C-reactive protein levels, and resolution of leukocytosis. The patient was eventually discharged with a follow-up appointment for spinal MRI imaging scheduled within 3 months.
Discussion
Posttraumatic spondylodiscitis is a relatively-uncommon but serious condition that can rarely occur following a spinal injury. It involves infection of the vertebral body (spondylitis) and an intervertebral disk (spondylodiscitis). The development of an RPA in the course of spondylodiscitis is uncommon and significantly worsens the clinical state, requiring urgent diagnosis and coordinated multidisciplinary management. 2
Several factors contribute to the development of infection in the posttraumatic setting. Spinal fractures can disrupt the normal protective barriers, allowing direct inoculation of bacteria into the disk space and vertebral bodies during the initial injury or subsequent surgical interventions. 3 Bacteria from a distant site of infection can spread through the bloodstream and colonize the injured spinal tissues, particularly if there is a hematoma present, as in our case. 4 The altered local vascularity at the fracture site can lead to blood stagnation and facilitate bacterial seeding. 4 Trauma creates a “locus minoris resistentiae,” a site of reduced resistance that is more susceptible to infection. 4 In the case of our patient, the traumatic injury led to multiple spinal fractures and a compromised immune system, creating a fertile ground for the development of infection.
RPA is a deep neck infection located in the retropharyngeal space, which extends from the skull base to the mediastinum. While RPA is more common in children, it can occur in adults, often with more severe consequences. 5 The development of RPA in conjunction with posttraumatic spondylitis is rare but can arise through several mechanisms. Infection from spondylitis, particularly in the cervical spine, can spread contiguously into the retropharyngeal space. 2 Trauma to the cervical spine can cause small mucosal lacerations in the oropharynx, a naturally-contaminated region, leading to secondary infection and osteomyelitis. 3 Immunocompromised individuals are more susceptible to developing RPA. 6 Conditions, such as diabetes mellitus, can increase the risk of infection.6,7 In our patient’s case, the infection spread from the cervical spine into the retropharyngeal space, resulting in an abscess that caused significant respiratory distress. The initial urgent endo-oral approach proved insufficient to control the abscess, as a recurrence occurred within 48 hours. This necessitated a second surgical intervention via an external approach, along with the placement of a drainage tube to ensure adequate evacuation.
Early and accurate diagnosis is crucial to prevent serious complications. Diagnostic modalities include imaging studies, laboratory tests, and, in some cases, tissue biopsy. MRI is the gold standard for diagnosing spondylitis or spondylodiscitis and associated complications, including epidural abscesses and RPAs. 8 MRI is also valuable for identifying spinal cord compression and other neurological complications. 2 CT scanning can be useful in the initial evaluation, particularly in trauma cases, to assess bony structures and identify fractures. 2 For our patient, MRI was pivotal in identifying both the spinal and retropharyngeal complications, which guided urgent treatment.
Management of posttraumatic spondylitis complicated by RPA requires a multidisciplinary approach involving otolaryngologists, neurosurgeons, infectious disease specialists, and other health care professionals. 2 The goals of treatment were to eradicate the infection, decompress neural structures, stabilize the spine (if necessary), and prevent complications. Broad-spectrum intravenous antibiotics should be initiated as soon as the diagnosis is suspected, even before culture results are available. 8 Empiric therapy should cover common pathogens such as S. aureus and streptococci. 4 Prolonged antibiotic therapy is typically required, usually for 6 to 8 weeks or longer. 8 In the case presented, our patient was started on broad-spectrum antibiotics, and his treatment was adjusted after microbiological cultures identified the causative pathogen.
Surgical intervention may be necessary in cases of spinal cord compression, spinal instability, large epidural or RPAs, or failure of conservative treatment. Surgical approaches may include anterior debridement and fusion, posterior stabilization, or a combined approach.4,9 Minimally-invasive drainage techniques may also be an option in some cases. 9 Surgical drainage of RPA is often necessary to relieve pressure on the airway and prevent further spread of infection. 2 Drainage can be performed through an intraoral or external approach. Our patient underwent multiple drainage procedures, both transoral and cervicotomy, to address the RPA and relieve respiratory distress, with a gradual improvement in his condition following these interventions.
RPA in the situation of posttraumatic spondylitis can lead to several serious complications, including sepsis, mediastinitis, airway obstruction, neurological deficits, and spinal instability. Prognosis depends on several factors, including the patient’s overall health, the severity of the infection, the causative organism, and the timeliness of diagnosis and treatment. Early diagnosis and aggressive multidisciplinary management are essential for improving outcomes. The prompt and aggressive treatment approach in our case led to a good clinical response, with the patient improving gradually over time, despite the severe nature of the complications.
Conclusion
Posttraumatic spondylitis complicated by RPA is a rare but potentially-life-threatening condition. A high index of suspicion, prompt diagnosis, and aggressive multidisciplinary management are essential for improving outcomes. MRI is the imaging modality of choice for diagnosis. Treatment includes intravenous antibiotics, surgical drainage of abscesses, and spinal stabilization if necessary. Clinicians should be aware of the potential complications of this condition and take steps to prevent them.
Footnotes
Consent for Publication
Written informed consent from the patient for the publication of this case report is available from the corresponding author upon reasonable request.
Author Contributions
Conception and design of study: Chiraz Halwani, Sana Boughariou, Sonia Esseghaier, Malek Khaskhoussi. Data analysis and/or interpretation: Chiraz Halwani, Sonia Esseghaier. Drafting of manuscript and/or critical revision: Chiraz Halwani, Sonia Esseghaier. Approval of final version of manuscript: Chiraz Halwani, Askri Haythem, Hedi Gharsallah.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.