
Abstract

Significance Statement
Arrested pneumatization is a developmental variant of the skull base that occurs during growth, often referred to as a “don’t touch” lesion due to its ability to mimic various pathologies on imaging. This condition can resemble fibrous dysplasia, osteomyelitis, bone metastases, or even malignant tumors such as chordomas, particularly in the clival region. Accurate diagnosis is essential to avoid unnecessary invasive procedures.
A 9 year-old female presented to the pediatric outpatient clinic with a history of vaginal bleeding that occurred once 4 months prior, along with ongoing headaches. Physical examination revealed no significant findings, and imaging studies were conducted to explore potential differential diagnoses. Suspecting early puberty, a contrast-enhanced brain MRI was performed to assess the possible central causes of precocious puberty. The MRI revealed a mass-like lesion in the clival region at the level of the sphenoid bone. On sagittal T1-weighted imaging, it appeared hypointense, while on T2-weighted imaging, it was heterogeneously hyperintense with partial heterogeneous enhancement post-contrast (Figure 1). Axial and coronal T2-weighted images showed internal septations extending toward the sphenoid wing (Figure 2). Although the lesion initially suggested a chordoma, the presence of septations and extension into the sphenoid wing indicated arrested pneumatization. Follow-up MRIs showed no change in the lesion’s size or characteristics, leading to the diagnosis of arrested pneumatization.
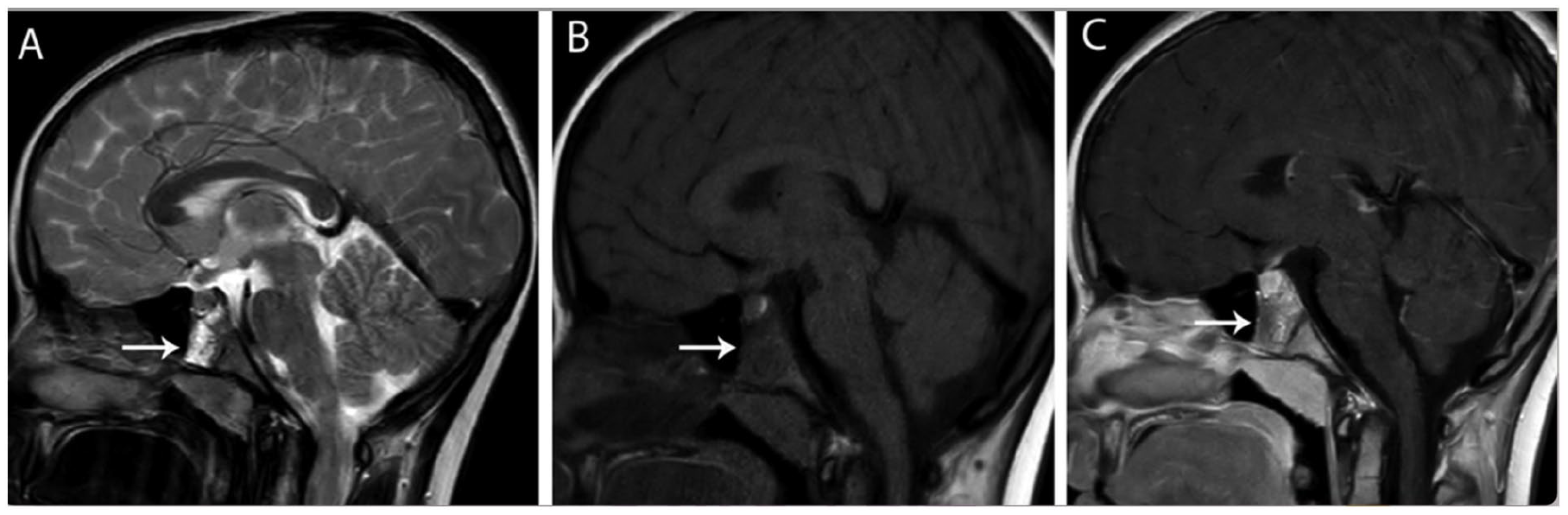
Sagittal T2-weighted image (A) demonstrates a heterogeneous hyperintense mass. The sagittal T1-weighted image (B) reveals a hypointense lesion. On the postcontrast sagittal image (C), a heterogeneous, partially enhancing mass lesion is observed at the sphenoidal level (arrows).
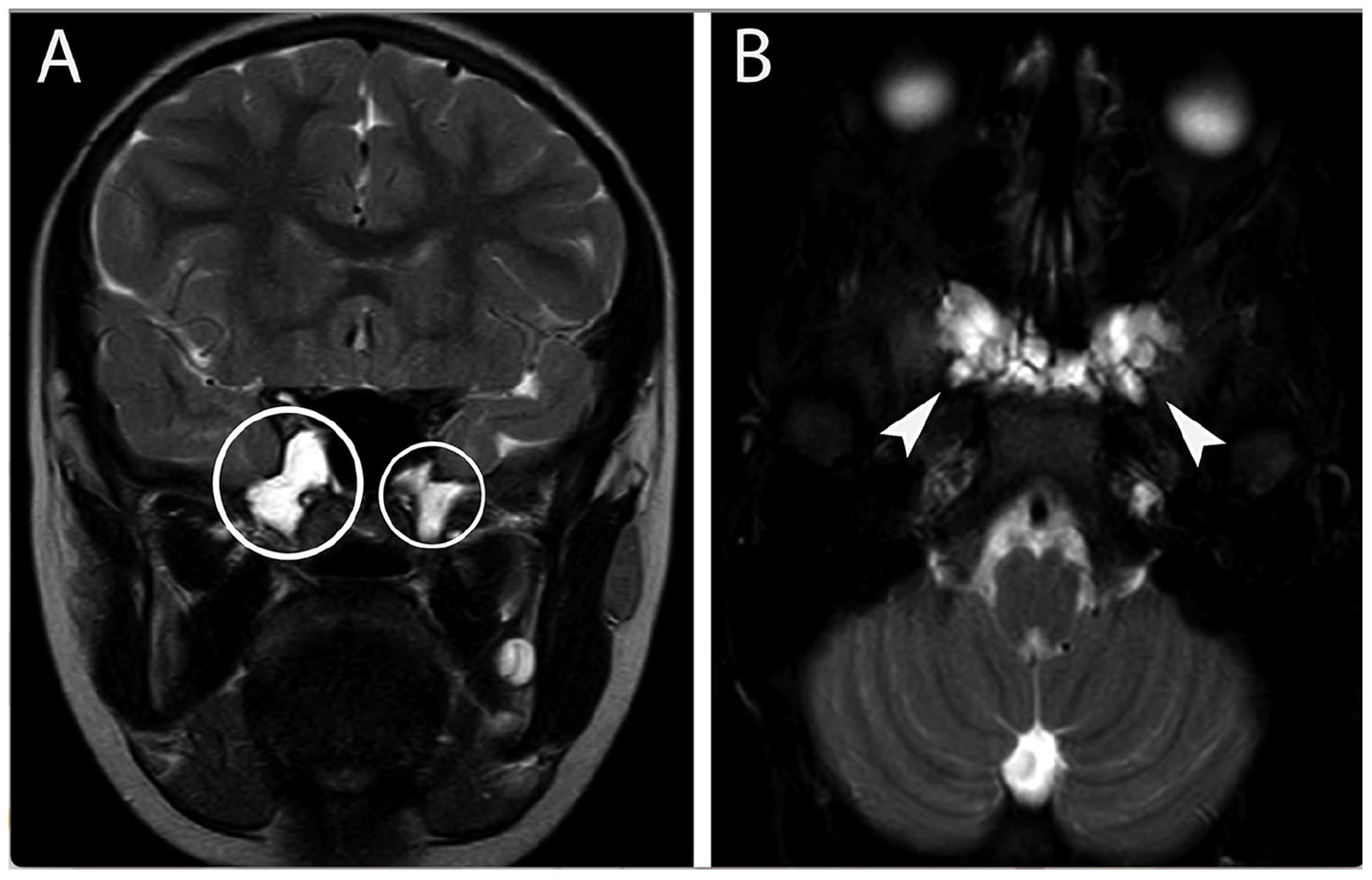
Coronal T2-weighted image with fat suppression (A, circled) and axial T2-weighted image (B, arrows) demonstrate septations and their extensions into both sphenoid wings.
Arrested pneumatization is characterized by the failure of normal pneumatization in the paranasal sinuses and mastoid air cells, resulting in the persistence of marrow instead of air. It is typically discovered incidentally and may be misinterpreted on imaging if not correctly identified. Imaging criteria for arrested pneumatization include its location within expected pneumatization areas, the presence of internal sclerosis and septations. These lesions often show little or no enhancement on contrast-enhanced imaging, which helps distinguish them from neoplastic processes like chordoma.1,2
Chordomas, rare malignant bone tumors originating from notochordal remnants, typically present as destructive, T2-hyperintense masses with strong contrast enhancement. 3 They require surgical resection, which can be challenging due to the tumor’s proximity to vital structures. Arrested pneumatization, however, is a benign anatomical variant and does not require treatment. These lesions are categorized as “don’t touch” lesions, meaning they should not be subjected to invasive procedures. 4 Thus, distinguishing between arrested pneumatization and chordoma is crucial for appropriate management.
In this case, despite initial concerns about chordoma, the absence of aggressive features and the presence of septations led to a diagnosis of arrested pneumatization. Radiological follow-up revealed no changes, confirming this diagnosis. In conclusion, arrested pneumatization should be considered in the differential diagnosis of clival lesions and must be ruled out before any interventional procedures are undertaken.
Footnotes
Consent for Publication
We declare that written informed consent for the publication of patient information and images was provided by the patient’s legal representative.
Author Contributions
Gökhan Polat: writing—review and editing (lead). Fatma Atılgan: writing—review and editing (supporting). Esin Aslı Aybayar: writing—review and editing (supporting).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.