
Abstract
Thymopharyngeal duct cysts are rare congenital lesions resulting from the persistence of the embryonic thymopharyngeal tract, typically presenting in pediatric populations. Adult cases are exceedingly uncommon and often misdiagnosed due to their rarity and nonspecific clinical features. We report the case of a 34-year-old woman who presented with a slowly-enlarging, painless left cervical mass initially suggestive of a thyroid pathology. Imaging revealed a well-defined cystic lesion at the lower pole of the thyroid gland. Surgical excision via a low cervicotomy was performed, and a left lobo-isthmectomy was carried out due to the lesion’s adherence to the thyroid. Final histopathological analysis confirmed a thymopharyngeal duct cyst. This case underscores the diagnostic challenges of lateral neck cysts in adults and highlights the importance of considering rare embryologic anomalies in the differential diagnosis, particularly when lesions mimic more common thyroid or branchial cleft pathologies.
Introduction
Cervical thymic cysts represent an exceedingly-rare cause of benign neck masses, accounting for less than 1% of all cervical lesions.1,2 Among them, thymopharyngeal duct cysts constitute a specific and even less common subtype, arising from incomplete involution of the thymopharyngeal duct during embryogenesis. 1 These cysts typically follow the migratory path of the thymus from the third pharyngeal pouch to the anterior mediastinum and can present anywhere along this descent, most often in the lateral neck. While frequently documented in children, particularly males, occurrences in adult patients are extremely rare and can pose significant diagnostic challenges. The clinical presentation is generally indolent, with nonspecific symptoms that may mimic other cervical pathologies such as thyroid cysts or branchial cleft anomalies.3,4 We report a rare case of a thymopharyngeal duct cyst in a 34-year-old woman, initially suspected to be a thyroid-related lesion, and ultimately diagnosed through surgical excision and histopathological examination. This case highlights the diagnostic pitfalls and emphasizes the importance of including congenital anomalies in the differential diagnosis of lateral neck masses, regardless of the patient’s age.
Case Report
A 34-year-old woman with no significant medical history presented with an anterior, basal cervical swelling that had been progressing over the past 8 months. The mass gradually increased in size without any associated symptoms, notably no dysphonia or dysphagia. On examination, a left-sided mass was noted, which was mobile during swallowing, firm, painless, and palpable at the lower pole. The remainder of the clinical examination was unremarkable, with no palpable cervical lymphadenopathy. Both vocal cords were mobile, and laboratory tests showed a normal TSH level.
Ultrasound examination revealed an enlarged thyroid, predominantly on the left lobe, with a well-defined, oval, cystic lesion measuring 6 × 4 cm at the lower pole, displacing the ipsilateral jugulo-carotid axis (Figure 1).
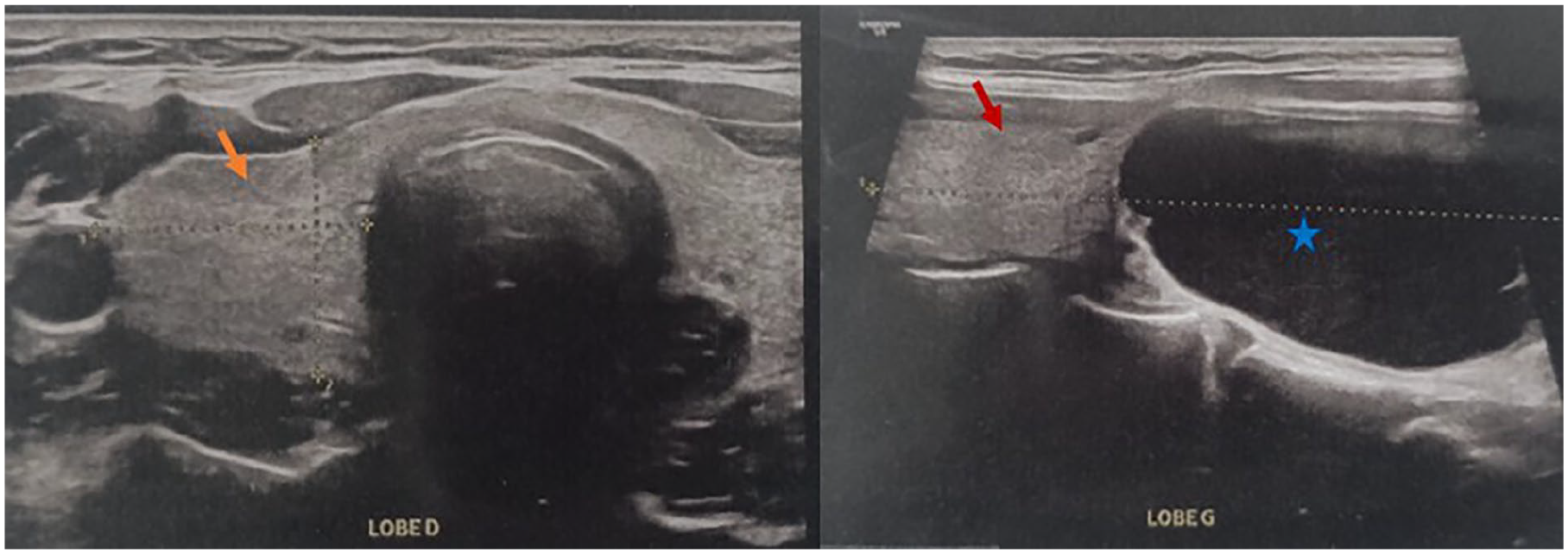
Cervical ultrasound. The right lobe (orange arrow) is non-nodular, whereas the left lobe (red arrow) is continuous with a unilocular cystic formation (blue star).
The patient underwent an exploratory cervicotomy. The surgical approach consisted of a low horizontal cervicotomy of the Kocher type. Intraoperatively, a left para-tracheal cystic mass adherent to the thyroid gland was identified (Figure 2), prompting the performance of a left lobo-isthmectomy. The lesion appeared as a cystic formation adjacent to the left thyroid lobe and ruptured during manipulation, which precluded the acquisition of intraoperative photographs. Based on its macroscopic appearance, the mass was initially suggestive of an exophytic thyroid nodule. Frozen section analysis first indicated a benign lesion. Final histopathological examination confirmed the lesion as a benign thymopharyngeal duct cyst (Figure 3). The postoperative course has been uneventful, with no recurrence observed after 2 years of follow-up. The patient did not require thyroid hormone replacement therapy.
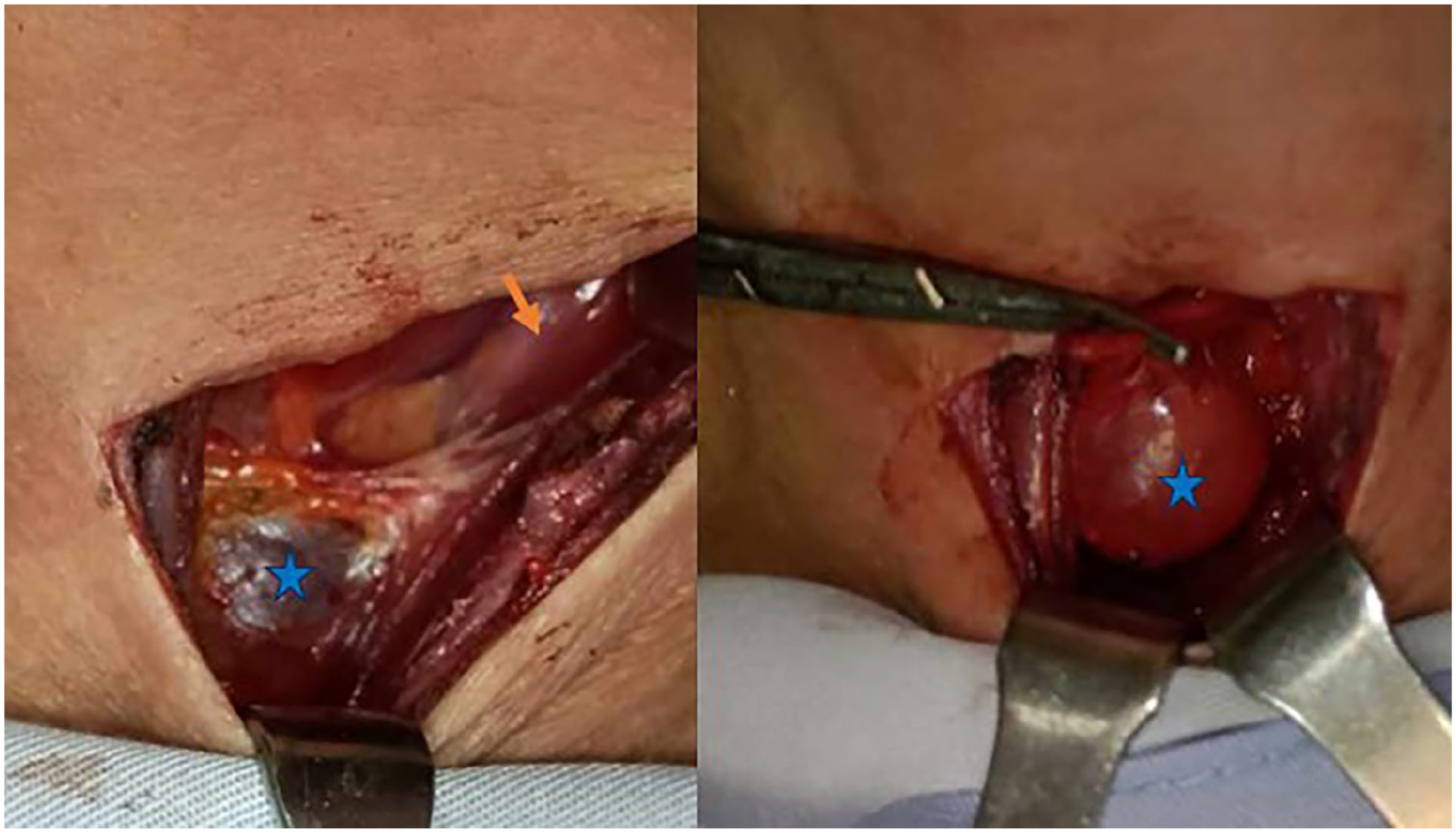
Per-operative view. A bluish pigmented left para-tracheal cystic mass (blue star) adherent to the left thyroid lobe (orange arrow).
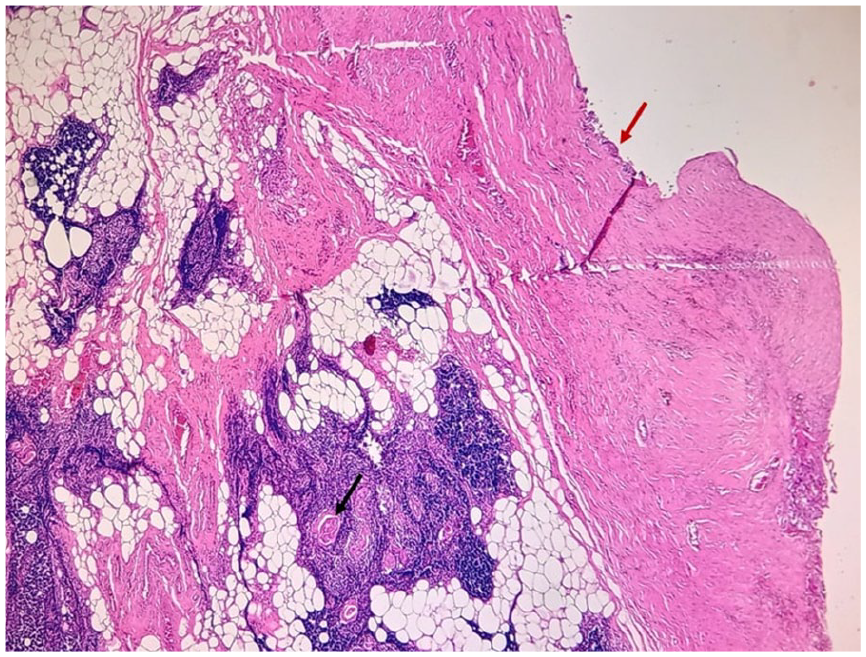
The cyst wall is lined by a flattened epithelium (red arrow). It contains remnants of thymic tissue with recognizable Hassall corpuscles (black arrow) (hematoxylin and eosin stain, original magnification 10×).
Discussion
Cervical thymic cysts, including their variant known as thymopharyngeal duct cysts, are rare developmental anomalies that arise from remnants of the thymopharyngeal tract. These lesions account for less than 1% of all cervical masses and are predominantly reported in children, making adult presentations particularly unusual and diagnostically challenging.1,5-7
The thymus originates from the third pharyngeal pouch, occasionally from the fourth, and migrates caudally during embryogenesis to its final location in the anterior mediastinum. Along its path of descent, thymic tissue may become sequestered, giving rise to ectopic thymic remnants or cysts anywhere along this trajectory, particularly in the lateral neck. A failure of involution or persistence of the thymopharyngeal duct may result in cystic formations, known as thymopharyngeal duct cysts.4,6 These cysts are generally unilocular or multilocular, and may extend deep into the mediastinum.
Although most reported cases occur in pediatric patients, typically males between 5 and 7 years of age, adult presentations have been documented sporadically, with no clear sex predominance.2,5 In adults, the clinical presentation is often insidious. Most patients report a painless, slowly-enlarging mass, commonly located on the left side of the neck, as seen in our case. The absence of compressive symptoms such as dysphagia, dyspnea, or hoarseness often delays diagnosis. 1
Radiologic findings are nonspecific and often suggest other cystic neck lesions such as thyroglossal duct cysts, branchial cleft cysts, lymphangiomas, or thyroid or parathyroid cysts.3,8 In our patient, the lesion’s proximity to the thyroid and its cystic nature raised the suspicion of a thyroid-related pathology. It was only through surgical excision and definitive histopathologic evaluation that the diagnosis of a thymopharyngeal duct cyst was established.
Histologically, these cysts are characterized by a cyst wall lined by stratified squamous or columnar epithelium, with the presence of thymic tissue often including Hassall’s corpuscles within or adjacent to the wall, which is the diagnostic hallmark.1,4 Surgical excision remains the treatment of choice and is generally curative. Complete resection is essential to prevent recurrence and to rule out malignancy.1,4,5
Conclusion
This case highlights the importance of considering rare congenital anomalies such as thymopharyngeal duct cysts in the differential diagnosis of lateral neck masses, even in adults. In our case, the cyst mimicked a thyroid lesion, further complicating the clinical picture. Accurate diagnosis depends on a high index of suspicion and careful histopathological assessment, especially given the frequent misidentification with more common entities like branchial cysts or lymphangiomas. Surgically, the potential extension of the cyst into the thoracic cavity poses additional challenges, emphasizing the need for meticulous preoperative evaluation and surgical preparedness.
Footnotes
Ethical Considerations
Our institution Faculty of Medicine of Sousse’s Ethics Committee does not require ethics approval for reporting individual cases or case series since we anonymously reported clinical and imaging information concerning our patient’s case.
Statement of Informed Consent
Written informed consent was obtained from the patient legal guardian for his anonymized information to be published in this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available on request