
Abstract
Objective
Thymic cysts are rare benign neck masses, accounting for less than 1% of all cervical masses. This study aims to discern different presentations, investigations, and treatment options of thymic cysts in adults by reviewing prior published studies from January 2010 to October 2021 to bridge the knowledge gap since the last review by Michalopoulos in 2011. Moreover, we present a case of a 28-year-old male with a left cervical thymic cyst.
Data sources
Data were obtained from a literature search using the ScienceDirect, PubMed, ResearchGate, and Google Scholar databases.
Methods and results
This study retrospectively analyzes reported cases of adult cervical thymic cysts by collecting demographic data, patient presentation, duration, location, size, type of imaging, fine-needle aspiration, and surgical approach. Eighteen patients were included. Cysts were seen on the left (n = 9), right (n = 5), and midline (n = 4). The age of the patients ranged from 19 to 64 years. Most patients present with painless left-sided neck swelling. Computed tomography (CT) was the preferred imaging modality in most cases. Moreover, surgical excision was essential for therapeutic and diagnostic purposes. This study did not require institutional review board approval.
Conclusion
Adult cervical thymic cyst is a rare etiology. Nevertheless, a painless left-sided neck mass with no clear lower border should uphold thymic cyst as a differential diagnosis. MRI and CT scans are the preferred imaging modalities for preoperative planning. Surgical excision is mandatory for treatment and histological confirmation. As of October 2021, around 54 cases of adult thymus cysts had been reported to the best of our knowledge and review.
Introduction
The thymus, found in the superior mediastinum behind the sternum, 1 has been identified as an essential organ for immune system development. The thymus is highly active during the neonatal and pre-adolescent periods but gradually shrinks and is eventually replaced by fat following puberty. 1 Embryologically, the thymus originates from the bilateral ventral wings of the third and fourth pharyngeal pouches and descends during gestation from high in the neck to its destination in the mediastinum; thus, ectopic thymic tissue may be present at any point along the path of descent. 1,2 Three types of thymic tissue have been described, including aberrant solid thymic rests (ectopic) with no clinical importance, cervical thymoma, and cystic thymic tissue. 2 Most reported cases of cervical thymic cysts (CTCs) pertain to pediatric patients, with a prevalence of around 1%. 1,2 CTCs in adults are extremely rare. 2,3 In adults, CTCs are typically misdiagnosed preoperatively as another cystic neck pathology, 2 and they present as painless neck masses that enlarge over time without other symptoms. A systematic literature review by Michalopoulos in 2011 identified thirty-six adult patients with a thymic cyst since it was first described by Lane in 1960. 2 In this review, an appraisal of reported cases of adult CTCs occurring from January 2010 to October 2021 was conducted to bridge the knowledge gap since the last narrative review. 2 Furthermore, we present a case of a 28-year-old man with a neck mass diagnosed as a CTC.
Methods
The ScienceDirect, PubMed, ResearchGate, and Google Scholar databases were searched using the following keywords: adult cervical thymus cyst, CTCs, and thyropharyngeal duct cyst. Patients with CTCs aged ≥18 years were included. The reported cases of adult CTCs occurring between January 2010 and October 2021 were extracted. Demographics, presenting complaints, cyst site, symptoms duration, imaging modality, definitive histopathology, and follow-up period were extracted and examined. This study did not require institutional review board approval.
Case Report
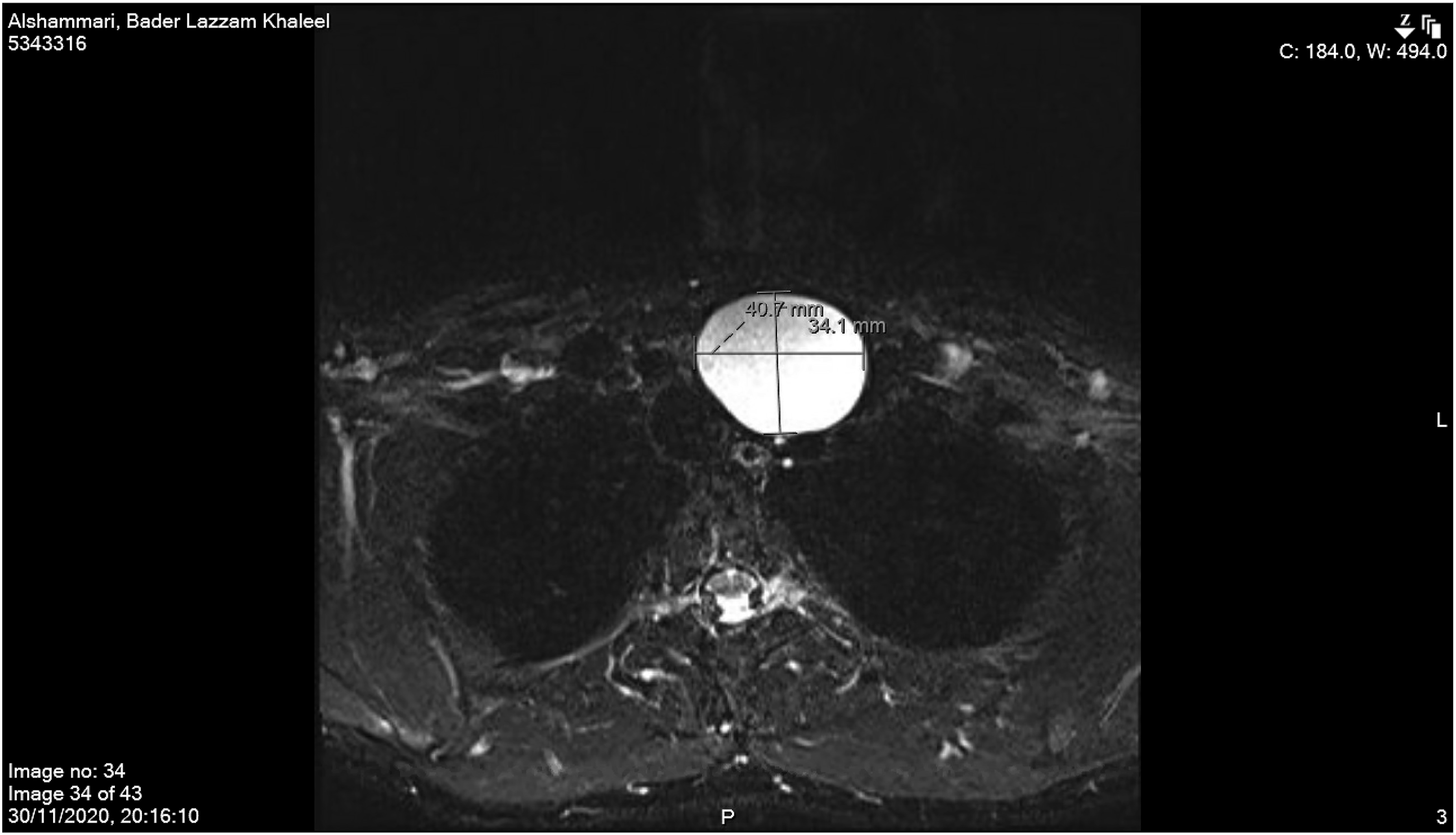
A 28-year-old man, with a history of eczema and ectopic dermatitis, was referred to King Faisal Specialist Hospital with a 2-year history of neck swelling on the left side. On referral, the patient reported that the swelling had stabilized in size and symptoms. The patient smokes 1 pack per year. The history was negative for pain, fever, dysphonia, hoarseness, dysphagia, odynophagia, loss of appetite, weight loss, constitutional symptoms, and significant family history. Physical examination revealed a firm left supraclavicular mass with no fixation, tenderness, or skin changes. It was deep to the sternocleidomastoid muscle with an unclear lower border. Flexible endoscopy of the nasal cavity, nasopharynx, oropharynx, and hypopharynx was normal. A non-contrast computed tomography (CT) performed at the referring hospital revealed a mass measuring 5.5 × 4.5 × 3 cm, containing a cyst filled with clear serous fluid (Figure 1). Gadolinium-enhanced-magnetic-resonance-imaging (MRI) confirmed a well-defined, homogeneous fluid-filled cyst centered deep in the peritracheal space, near the left thyroid lobe, with a clear claw-sign along its outer margin. Gadolinium-enhanced MRI also showed homogeneous T1-hyperintensity and T2-hyperintensity with no central enhancement, a mild mass effect, and a rightward tracheal shift. There were no signs of aggression or invasion. The mass dimensions were 34 mm (anteroposterior) × 41 mm × 55 mm (Figure 2). The main differential diagnoses were thyroid/parathyroid cyst and branchial-cleft cyst type III/IV, with the least likely being epidermoid cyst and lymphatic malformation. Subsequently, the patient underwent left neck exploration and cyst removal via a transcervical approach through a horizontal incision. Intraoperatively, the cystic mass extended from the lower border of the inferior aspect of the left thyroid lobe to the upper mediastinum. The mass was superiorly dissected and separated from the left thyroid lobe without the need for thyroid vessel ligation. The dissection continued to the upper mediastinum, where the cyst was separated from the thymus and completely resected. The patient was admitted postoperatively for observation and drain monitoring. He was discharged on the third postoperative day following drain removal (25 cc/24 h). The final histopathological report showed a thymic cyst with unremarkable thymic gland tissue. He had a follow-up 3 months postoperatively with no complications or recurrence. Computed tomography of the head and neck (non-contrast) depicts a coronal section illustrating the craniocaudal extent of the cyst. Magnetic resonance imaging of the head and neck T2-signal, with hyperintense mass and clear margins.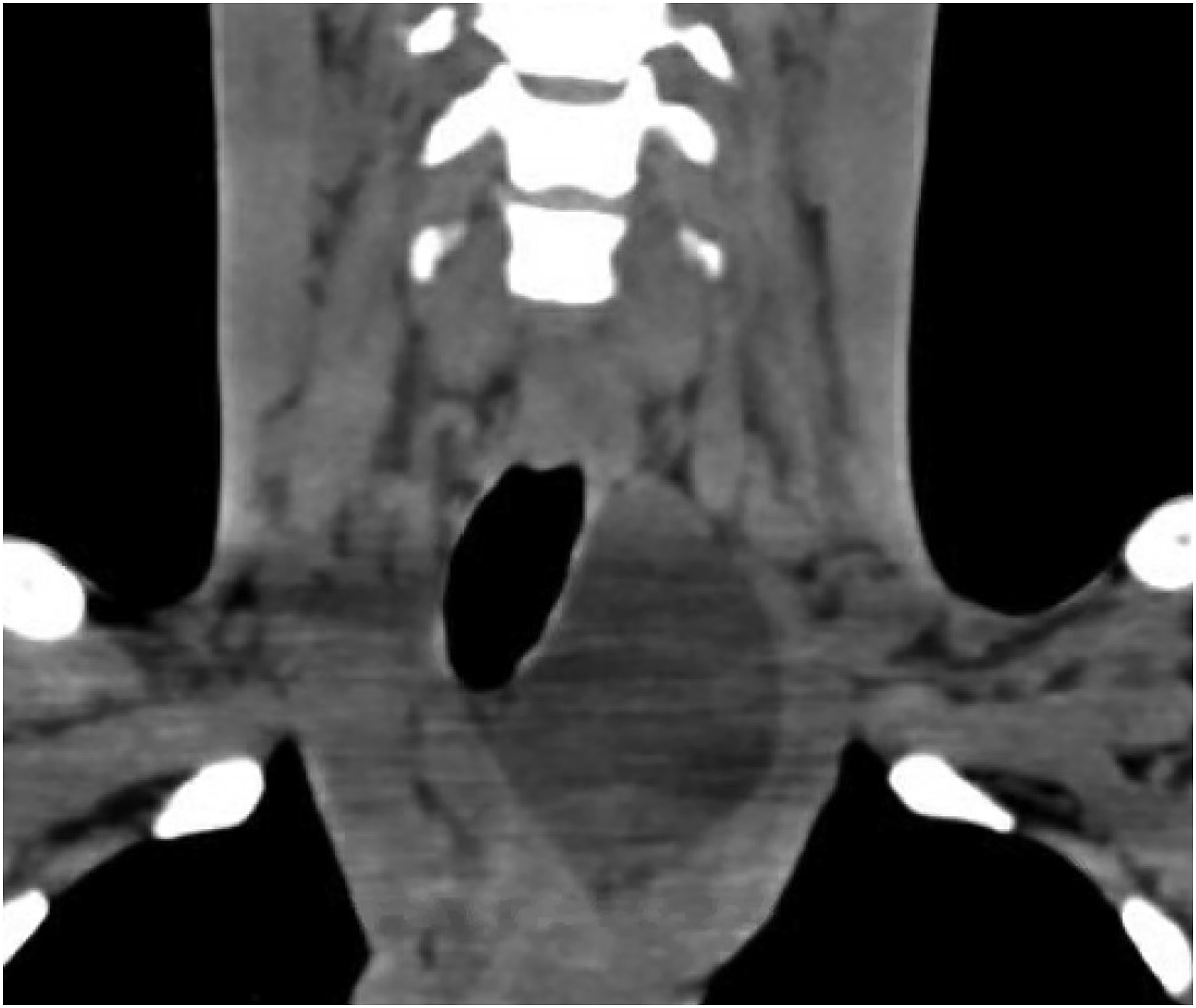
Results
A review of cases of cervical thymic cysts in adults from January 2010 to October 2021.
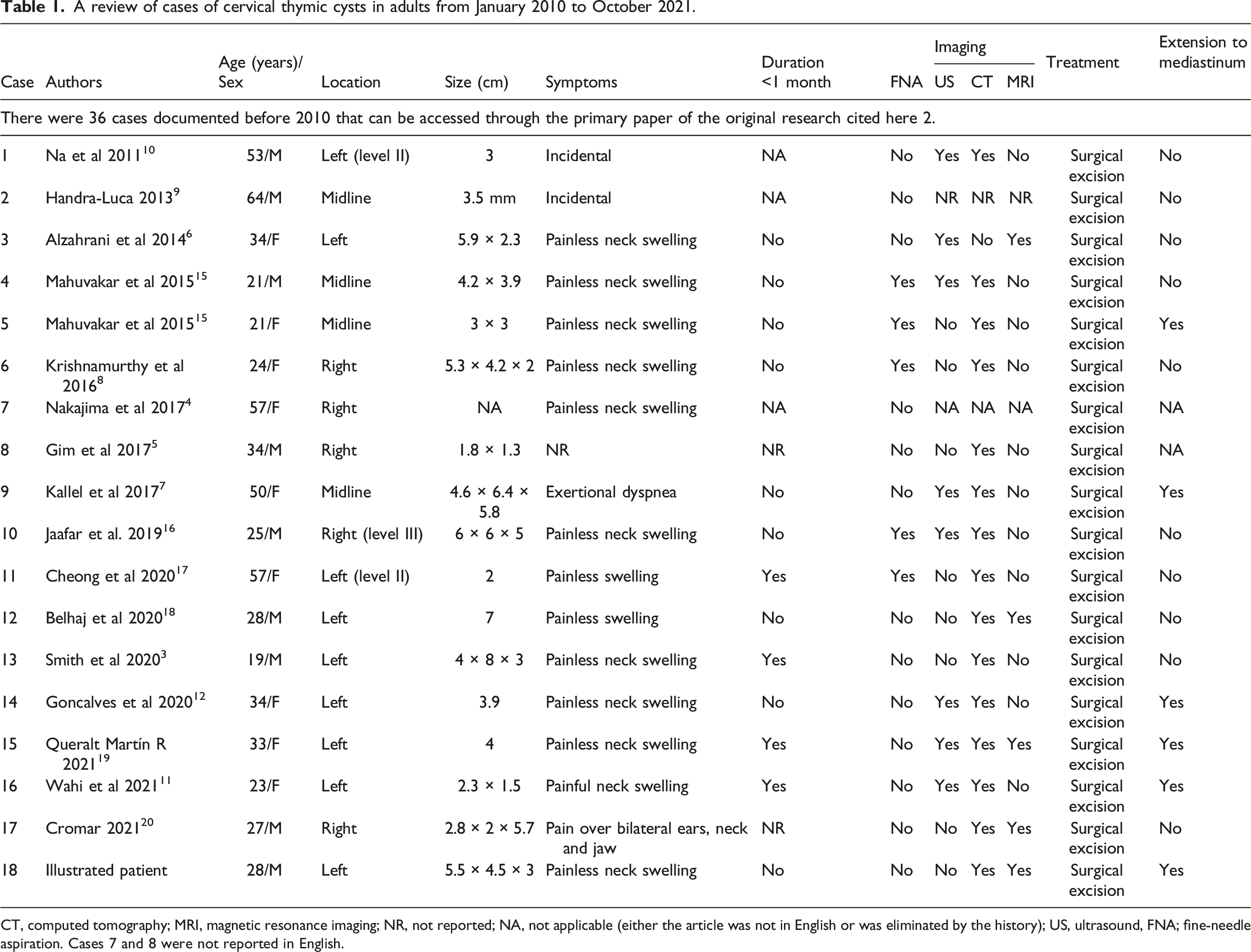
CT, computed tomography; MRI, magnetic resonance imaging; NR, not reported; NA, not applicable (either the article was not in English or was eliminated by the history); US, ultrasound, FNA; fine-needle aspiration. Cases 7 and 8 were not reported in English.
Discussion
Clinical presentations
Thymoma, ectopic tissue, and cysts are possible clinical manifestations of the thymus and thymic tissue in the neck. 2 Multiple explanations for CTC pathogenesis have been proposed. However, the two most accepted theories indicate a congenital origin due to the persistence of the thymopharyngeal ducts or an acquired form of Hassall’s corpuscle degeneration with ectopic thymic remnants. 2,3,6 -8
Thymic cysts are extremely rare causes of benign neck masses that are undetected before surgery. 2,3 The presentation is often a painless, enlarging neck mass during the first decade of life. 1 While most patients are asymptomatic, cyst abutment against local structures induces several symptoms, including respiratory distress, dysphagia, and hoarseness. 1 CTCs in children, if symptomatic, are more severe than those in adults. 2
In adulthood, the presentation is different; most patients in the reviewed cases sought medical attention for painless enlarging neck masses, with only a few reporting dyspnea, dysphagia, or hoarseness. 2 Most adult CTCs present on the left side of the neck, and the average age of presentation is 36 years. 2
Although CTCs have been well characterized in previous case reports, they are commonly misdiagnosed prior to surgery; the conclusive diagnosis is predicated on histological findings. 1 -3,6 -12 Achieving a correct preoperative diagnosis is difficult, and there is no diagnostic measure that can accurately identify a thymic cyst yet. 1 -3,6 -12 Therefore, many surgeons are not sufficiently familiar with CTCs and fail to include them as a differential diagnosis. 3,8 CTCs are commonly confused with other cystic masses, including thyroglossal duct cysts, branchial cleft cysts, cystic hygromas, dermoid cysts, epidermoid cysts, thymic cysts, bronchogenic cysts, and laryngoceles. 1 -3,6 -12
Diagnostic methods
The imaging modalities reported for identifying CTCs are US, CT, and MRI. US is an effective initial modality for differentiating solid cystic masses from hypoechoic CTCs with few septa and internal echoes. 1 -3,6 -12 Contrast-enhanced CT delineates the cyst more clearly and determines its relationship with other anatomical landmarks for precise preoperative planning. CT illustrates homogeneity, hypodensity, and minimal rim enhancement. 1 -3,6 -12 As a complementary modality, MRI can provide more comprehensive details regarding adjacent anatomical structures that facilitate the exclusion of differential diagnoses. 1 -3,6 -12 If a thymus cyst is suspected preoperatively, MRI is the most appropriate choice for identifying the presence of normal thymus tissue, particularly in children. 2 Adults may have persistent thymus tissue in the neck, although this tends to shrink with age. However, persistent thymus tissue should not be confused with pathology. 13 The malignant transformation of CTCs is extremely rare in adults and has not been reported in children. 3 In adults, malignant mutations of CTCs include squamous cell carcinoma cases and basaloid thymus carcinoma. 2,14
Surgical approaches
Surgery via transcervical approach with neck exploration has been the standard procedure. 1 -3,6 -12 Additionally, an approach involving a vertical incision along the sternocleidomastoid muscle has been reported. 1 -3,6 If an extension is noticed deep within the mediastinum upon limited exposure, a sternotomy can be performed according to current experts’ opinion. 1 -3,6 -12 In pediatric patients, avoidance of removing normal thymus tissue is essential for the development of the immune system. 1 -3,6 -12
Limitations
The limitations of this study include the retrospective design, which cannot eliminate publication bias, including an inadvertent subjective selection of data. The review is strengthened by compiling easily accessible data regarding a rare disease, which can help researchers analyze tabulated and pooled data for future studies.
Implications for Practice
As there is currently no diagnostic test that can reliably identify thymic cysts, diagnosis requires a thorough review of the clinical presentation, diagnostic imaging, surgical findings, and histologic characteristics. Thus, in patients with a neck cystic mass mainly on the left side with an unclear lower border, CTCs should be considered a differential diagnosis. This research will provide physicians with an accessible reference for clinical decision-making in an adult patient with a cervical thymic cyst.
Footnotes
Author contributions
Hesham Saleh Almofada: primary author (literature review, data collection/organization, writing of the manuscript and case report, and supervision). Norah Ibrahim Almedemgh: literature review and writing the case report. Eyas Othman: supervision and primary surgeon.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.