
Abstract
Introduction:
Papillary thyroid microcarcinomas (PTMC) can exhibit invasive behavior with lymph node metastasis despite their small size. In some cases, they may present as cystic lymph node metastases, clinically and radiologically mimicking benign lesions such as branchial cleft cysts. These misleading presentations may delay the diagnosis of an underlying thyroid malignancy. We report a rare and atypical presentation of PTMC as a large contralateral cystic lymph node metastasis initially diagnosed as a branchial cleft cyst, highlighting the need to consider metastatic thyroid carcinoma in the differential diagnosis of lateral neck cysts.
Observation:
A 51-year-old woman presented with a left lateral cervical mass diagnosed as a second branchial cleft cyst. Surgical excision and histology revealed a metastatic lymph node from papillary thyroid carcinoma. Subsequent workup identified a 4 mm PTMC in the right thyroid lobe. The patient underwent total thyroidectomy, lymph node dissection, and radioactive iodine therapy.
Conclusion:
PTMC may behave aggressively and present with misleading cystic nodal metastases. Clinicians should include metastatic papillary thyroid carcinoma in the differential diagnosis of isolated cystic neck masses, even in the absence of an identifiable thyroid lesion on initial imaging.
Introduction
Papillary thyroid microcarcinoma (PTMC) is defined as a papillary thyroid carcinoma measuring ≤1 cm, typically exhibiting an indolent behavior with a low mortality rate (<1%). 1 Loco-regional spread occurs in approximately 2% to 6% of cases, while distant metastasis is observed in about 1% to 2% particularly in tumors larger than 5 mm. 2 The presence of large contralateral cystic lymph nodes may indicate a more aggressive tumor phenotype, making it far from an indolent tumor and suggesting the need for a more aggressive treatment approach with close monitoring. We report a rare case of PTMC presenting as a large contralateral cystic lymph node metastasis without prior detection of a primary thyroid tumor initially diagnosed as a branchial cleft cyst, highlighting the diagnostic challenges and therapeutic implications of this atypical presentation.
Observation
This case involves a 51-year-old female patient with a history of cholesteatomatous otitis media, sinonasal allergy, and penicillin allergy. She presented with a left laterocervical swelling that had been evolving for 1 year, without signs of compression. On examination, a renitent, painless left laterocervical mass measuring 5 cm was identified at levels III and IV, with intact overlying skin. The remainder of the clinical examination was unremarkable, revealing a free cavum, a mobile and normally-appearing larynx, and an uninvolved thyroid compartment.
Cervical ultrasound revealed a 48 mm unilocular cystic lesion in the left lateral neck, suggestive of a second branchial cleft cyst, along with a few left jugulocarotid lymph nodes with preserved architecture. The thyroid appeared underdeveloped, harboring non-characterizable right-sided nodules. A cervical computed tomography scan (Figure 1) showed a left basal cervical cystic mass, subhyoid in location, positioned lateral and anterior to the jugulocarotid axis. The lesion measured 5 mm at its longest axis, displaced the left thyroid lobe, compressed the internal jugular vein, and was in contact with the internal carotid artery.
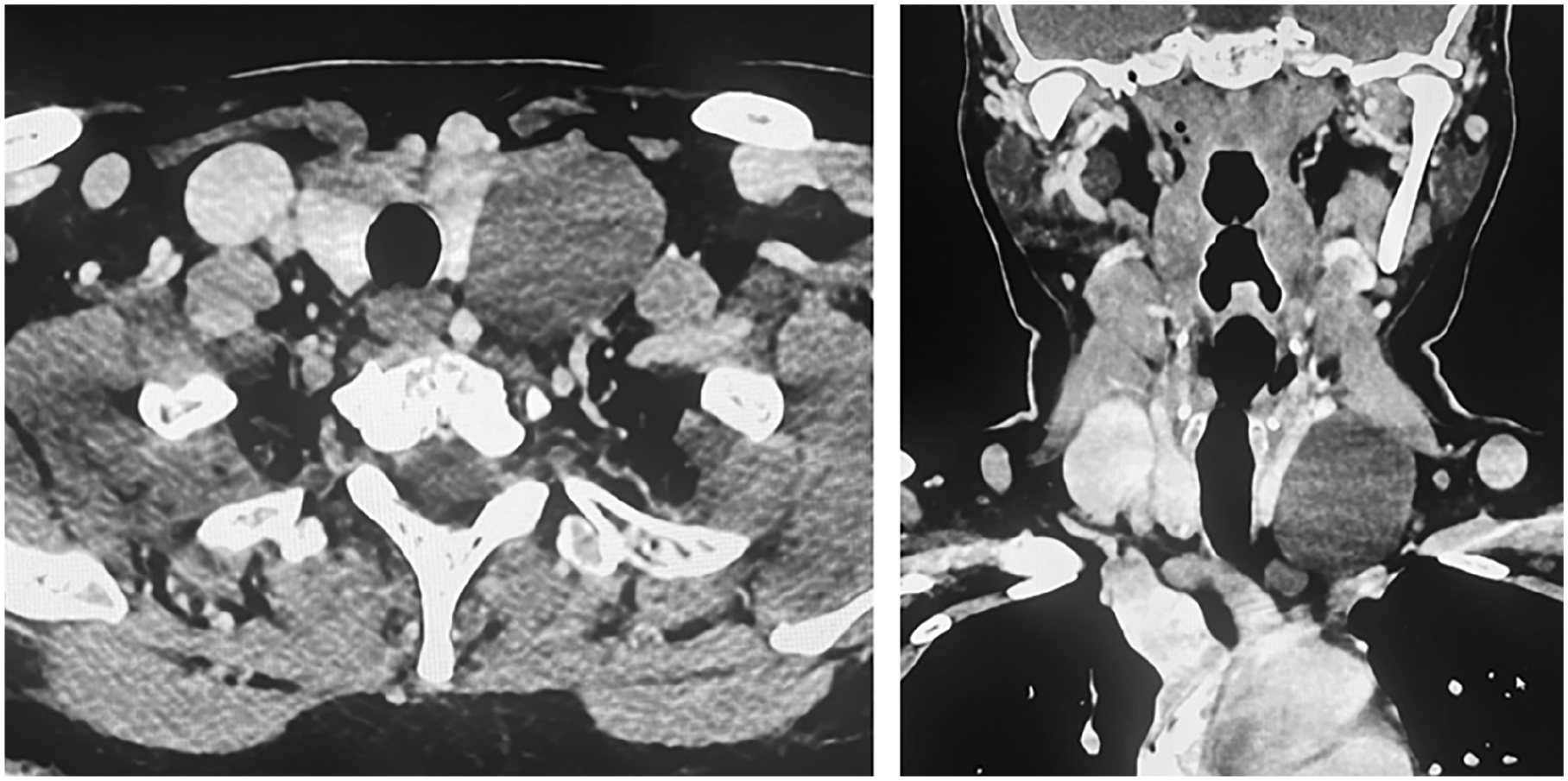
Axial and coronal CT scan sections showing a left basal cervical cystic mass, located lateral and anterior to the jugulocarotid axis, measuring 5 cm at its longest axis, displacing the left thyroid lobe and compressing the internal jugular vein. CT, computed tomography.
The patient underwent cervicotomy with excision of the mass, along with lymph node dissection of adjacent adenopathies (Figure 2). Histopathological examination revealed metastatic involvement of a lymph node from a papillary carcinoma (Figure 3). Immunohistochemistry confirmed thyroidal origin, as the cystic mass cells expressed thyroglobulin. The dissected lymph nodes also showed metastatic involvement.
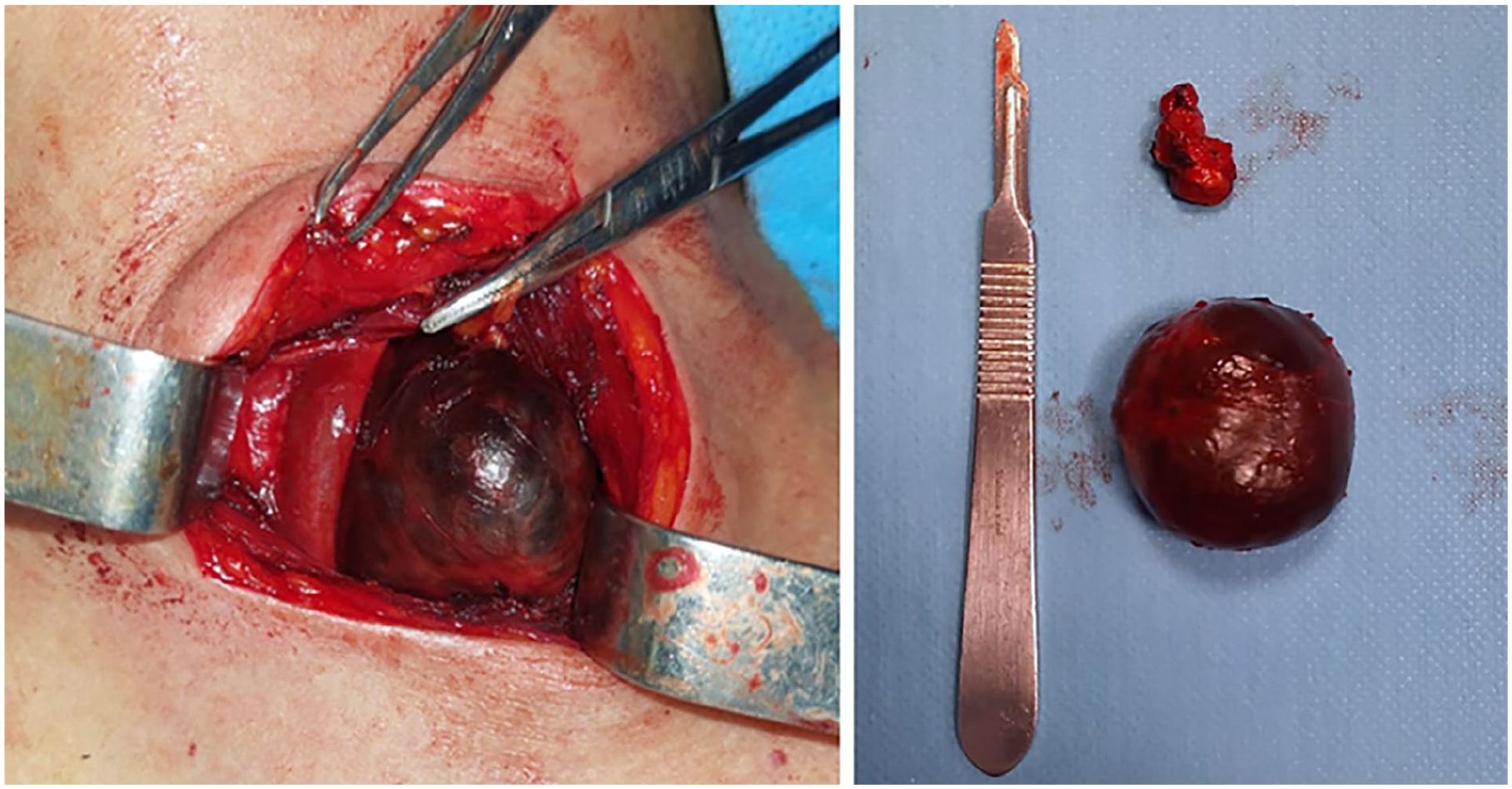
Intraoperative view revealing a smooth well-rounded cystic mass resembling a branchial cyst, with resection of a few adjacent lymph nodes.
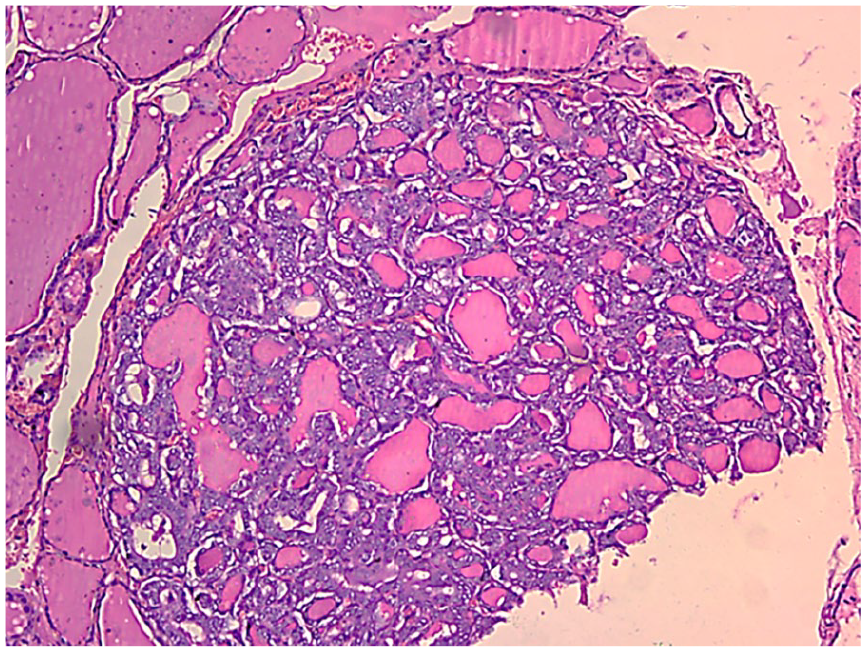
Histopathological analysis confirming a single 4 mm focus of intrathyroidal papillary microcarcinoma with capsular invasion but no vascular emboli.
A follow-up thyroid ultrasound identified a 6 mm nodule in the right upper thyroid lobe, classified as EU-TIRADS 5 (very hypoechoic with microcalcifications), along with 2 potentially-metastatic lymph nodes at left level IIa. thyroid-stimulating Hormone (TSH) levels were within normal limits.
The patient subsequently underwent a total thyroidectomy with bilateral central and left functional neck dissection. Histopathological analysis confirmed a single 4 mm focus of intrathyroidal papillary microcarcinoma with capsular invasion but no vascular emboli. Left central and lateral neck dissection confirmed metastatic lymph node involvement, whereas the right central neck dissection showed no metastatic disease.
Postoperatively, the patient received metabolic irradiation with 100 mCi of radioactive iodine (RAI). Posttreatment scintigraphy demonstrated a large intensely-avid midline cervical area corresponding to residual thyroid tissue. The stimulated thyroglobulin level was 7 μg (TSH >46 IU).
She was placed on suppressive therapy with
Discussion
PTMC is traditionally considered an indolent tumor with low morbidity and mortality. 1 However, in certain cases, it can exhibit aggressive features, including lymph node metastasis and extrathyroidal extension, which significantly alter both prognosis and management strategies. Our case highlights an unusual and deceptive presentation of PTMC, initially diagnosed through a large contralateral cystic lymph node metastasis in the absence of a detectable primary thyroid lesion. This rare presentation challenges the conventional perception of PTMC as a low-risk entity and underscores the importance of comprehensive preoperative assessment to avoid underestimating disease severity.
Although lymph node metastasis in PTMC is relatively uncommon (2%-6%), it typically involves ipsilateral cervical nodes, particularly at levels VI and III. 2 The presence of a large cystic metastatic lymph node in the contralateral neck, as observed in our patient, is suggestive of a more aggressive tumor phenotype and necessitates a tailored therapeutic approach. The absence of an initially-identifiable primary thyroid tumor further reinforces the need for a systematic and meticulous evaluation of the thyroid in all patients presenting with suspicious lateral neck masses.
Importantly, cystic lymph node metastases from papillary thyroid carcinoma (PTC) are frequently misdiagnosed as benign lesions, such as second branchial cleft cysts, leading to potential delays in appropriate management. Thus, in the presence of an isolated large cystic neck mass, particularly in adults, a malignant etiology must always be considered. 3 Sagit et al highlighted this diagnostic pitfall in a report describing a case of PTC entirely confined within a lateral cervical cyst initially presumed to be a branchial cleft cyst. 4
Moreover, the involvement of contralateral lymph nodes is associated with a higher risk of disease recurrence and warrants a more aggressive surgical approach. In such cases, total thyroidectomy combined with comprehensive neck dissection becomes necessary to achieve optimal disease control. 5
Our case underscores the need for an individualized approach in the management of PTMC. Although the American Thyroid Association guidelines endorse conservative strategies such as active surveillance for low-risk PTMC, our patient did not qualify for this approach due to the presence of nodal metastasis and capsular invasion.
The therapeutic plan included total thyroidectomy with neck dissection, justified by the contralateral lymph node involvement and aggressive histopathological features. Comprehensive lymphadenectomy was performed due to the extensive nodal spread. Postoperative RAI therapy was administered at a dose of 100 mCi, and post-RAI scintigraphy confirmed residual cervical uptake, supporting the need for close long-term surveillance. Follow-up also included suppressive therapy with levothyroxine to maintain TSH suppression, alongside stimulated thyroglobulin monitoring for early detection of recurrence. 6
Conclusions
This case underscores that PTMC, despite its small size, can present with aggressive features, particularly when associated with contralateral large cystic lymph node metastases. Such cases should be managed with total thyroidectomy, neck dissection, RAI therapy, and close follow-up to optimize long-term outcomes. Recognizing atypical presentations of PTMC is crucial to ensuring timely diagnosis and appropriate treatment, thereby reducing the risk of recurrence and metastasis.
Footnotes
Consent to Participate
Written informed consent from the patient for the publication of this case report is available from the corresponding author upon reasonable request.
Author Contributions
Conception and design of the study: Chiraz Halwani, Ammar Anas. Data analysis and/or interpretation: Salma Elbessi, Tlili karima, and Sonia Besseghaier. Drafting of the manuscript and/or critical revision: Chiraz Halwani. Approval of the final version of the manuscript: Chiraz Halwani and Khemaies Akkari.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.