
Abstract

Significance Statement
This case presents an extremely rare anatomical variation of the right common carotid artery, which intraoperatively followed an angled course overlying the trachea in the midline. A preoperative neck magnetic resonance imaging confirmed the presence of a high-riding brachiocephalic trunk, initially following a vertical ascending course before giving rise to its major branches. Recognising such variations through thorough clinical examination and preoperative imaging can prevent inadvertent injury and, ultimately, life-threatening complications.
Case Presentation
A 66-year-old Caucasian female with papillary thyroid cancer underwent total thyroidectomy with central and right selective neck dissection. Interestingly, during the dissection of the right carotid sheath, the right common carotid artery appeared to follow an unexpected, angled course overlying the trachea in the midline before continuing its expected course laterally (Figure 1). No further vascular anatomical variations of the right common carotid artery (RCCA) were encountered, as it bifurcated into the right external and internal carotid arteries, respectively, without providing any additional branches. The operation was completed successfully, and the patient had an uneventful recovery without any postoperative complications.
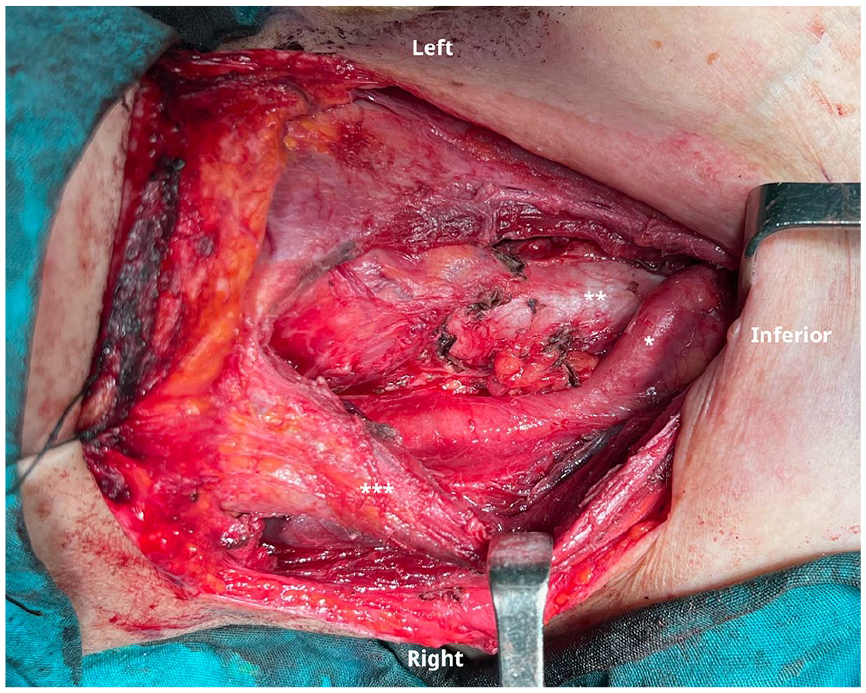
Intraoperative imaging showing the RCCA (*) overlying the trachea (**) after arising from the high-riding BCA and then following a right-sided course. The infrahyoid muscles (***) are retracted to improve surgical exposure. BCA, brachiocephalic artery; RCCA, right common carotid artery.
Postoperatively, the related anatomy was studied thoroughly on MRI, examining possible associated neurovascular or other anatomical variations. The imaging findings confirmed a high-riding brachiocephalic trunk, which was arising from the midline, following a vertical ascending course and then branching off to give the RCCA and the right subclavian artery (RSA). The RCCA arose from the midline and then followed a right-sided course, continuing in its expected anatomical position, as displayed in Figure 2. Otherwise, no further anatomical variations were identified.
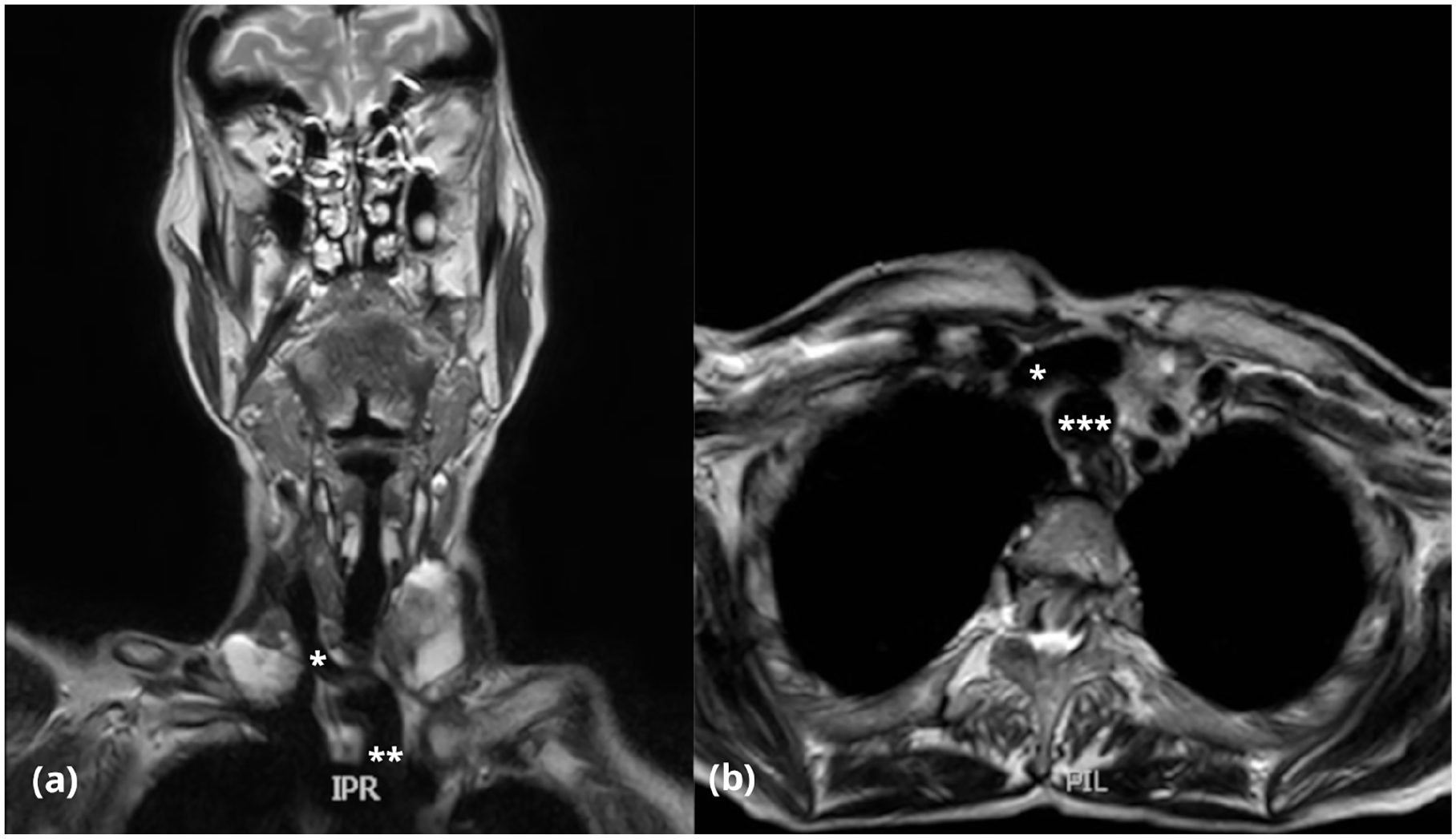
Coronal (a) and axial (b) view of T2-weighted MRI showing the course of RCCA (*) and BCA (**), related to the trachea (***). MRI, magnetic resonance imaging; RCCA, right common carotid artery.
The anatomy of the great vessels in the neck is considered quite consistent. A study reviewing aortic arch variations in 1.266 patients using angiographic and computed tomography imaging, revealed that 74.72% had normal vascular anatomy, with a typical left-sided aortic arch, and only 3 main branches: the brachiocephalic artery (BCA), the left common carotid artery (LCCA) and the left subclavian artery. 1 The most common anatomical variations of the major aortic arch branches include the common origin of BCA and LCCA, the LCCA arising as a branch of the BCA, a bi-carotid trunk, an aberrant RSA, and an anomalous origin of the vertebral artery. 2
Embryologically, the BCA develops from the right horn of the aortic sac and the proximal right fourth aortic arch, while the RCCA and right internal carotid artery (ICA) develop from the right third aortic arch. In our case, apart from the BCA and RCCA, the remaining neurovascular structures, including the right ICA, followed a normal anatomical course without giving rise to additional branches. Although vascular anomalies are often attributed to false embryogenesis, the absence of other associated vascular anomalies makes a definitive embryological explanation challenging.
Interestingly, a study assessing the prevalence of major vessels overlying the trachea reported that the most common vessel encountered was the BCA, accounting for 33.4% of cases, followed by high-riding innominate veins. 3 The right carotid artery was found to overlap more than 50% of the trachea in 3.2% of cases, even though whether that was regarding the common, external, and/or ICA and what the related anatomical variations were not clearly stated.
Anatomical variations of major cervical vessels, particularly involving the RCCA, are rare but clinically significant. Among the very few reported cases of an RCCA overlying the trachea and crossing the midline of the neck, to our knowledge, this is the only case report describing an RCCA arising from the midline from a high-riding BCA in an otherwise healthy individual, with available preoperative MRI and intraoperative dissection images. Awareness of such vascular variants is crucial, as they can significantly increase the risk of inadvertent injury during common head and neck procedures. Thorough clinical examination, detailed interpretation of preoperative imaging, and the utilization of bedside ultrasound, especially in the emergency setting, are vital in identifying such anomalies and reducing the risk of severe intraoperative complications such as acute major hemorrhage.
Footnotes
Consent for Publication
Written informed consent was obtained from the patient for anonymized patient information and images to be published in this article.
Author Contributions
Conceptualization, K.C.; methodology, S.M. and K.C.; investigation, S.M., E.P., D.A., and K.C.; resources, S.M. and K.C.; data curation, S.M., M.K., and K.C.; writing-original draft preparation, S.M., E.P., and K.C.; writing-review and editing, D.A. and M.K.; supervision, K.S. All authors have read and agreed to the published version of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.