
Abstract
Purpose:
The pathogenesis of chronic rhinosinusitis (CRS) is thought to include a complex interaction between environmental exposures and host immune responses that generates a self-perpetuating inflammatory process. As molecular pathways continue to be explored, the impact of environmental exposures on CRS pathogenesis and exacerbation must not be overlooked. This review will explore the association between environmental exposures and CRS, specifically focusing on tobacco smoke, occupational inhalational exposures, air pollution, particulate matter, and wildfire smoke.
Major Findings:
Tobacco smoke is associated with increased prevalence of CRS symptoms and formal diagnosis with worse surgical outcomes observed in both adults and children exposed to tobacco smoke. Numerous occupational exposures have been associated with increased sinonasal symptoms, though exposures and disease definitions are often poorly characterized. Pollution and microparticle exposure has been associated with an increased likelihood of CRS diagnosis, as well as increased need for surgery. Last, while wildfire smoke has been attributed to increased hospital and emergency room visits for respiratory-related complaints, no primary research has yet been performed regarding CRS and wildfire smoke, though in-vitro studies support an association.
Conclusions:
Population-based studies bolstered by in-vitro mechanistic data support an association between numerous environmental exposures and the onset and severity of CRS.
Introduction
Chronic rhinosinusitis (CRS) is a complex inflammatory condition of the paranasal sinuses defined according to the phenotype with which patients present: nasal congestion, nasal discharge, sinus pain/pressure, and decreased sense of smell with confirmation of objective disease by either computed tomography (CT) or nasal endoscopy. 1 Further delineation by the presence or absence of polyps remains the predominant classification scheme; however, research within the past 2 decades has defined CRS endotypes based on predominating cytokines. 2 As 21st century medicine transitions to a more personalized and etiological approach to pathology, the pathophysiological mechanisms underpinning CRS have taken on greater significance. Ongoing research hopes that through a better understanding of the complex molecular host pathways and environmental interactions, clinically-relevant markers of disease that double as therapeutic targets may be uncovered. The authors of the 2021 International Consensus statement on Allergy and Rhinology: Rhinosinusitis refer to these as “Treatable traits,” borrowing the concept from a consortium of respiratory clinicians advancing therapies of pulmonary conditions.1,3 The recent success of biologic therapies, such as dupilumab and omalizumab, coincidentally also borrowed from the pulmonary field, are proofs of concept.4,5
As cytokine and inflammatory profiles of CRS are slowly coming into focus, so too are the contributions of environmental exposures to pathogenesis and disease severity. The purpose of this review is to synthesize the recent relevant literature related to these contributions. The association between aeroallergens and the potentiation of sinonasal disease has been well-established and discussed extensively elsewhere.6-10 This review will instead focus on the impact of smoke and irritant inhalation and CRS. After reviewing well-studied associations among tobacco smoke, occupational exposures, and CRS, the remainder of the review will focus on literature published in the past 5-7 years regarding the emerging threats to sinonasal health represented in air pollution, particulate matter (PM), and wildfires. With the unified airway theory positing a strong association between upper and lower respiratory physiology and pathophysiology, primary data, and outcomes within each subtopic will be viewed relative to research performed in the lower respiratory tract. Using this paradigm, extant gaps in the literature will be highlighted.
Methods
Between December 15, 2024 and February 12, 2025, PubMed was queried with combinations of the following search terms: “Chronic rhinosinusitis,” “Sinusitis,” “Tobacco,” “Smoke,” “Cigarette smoke,” “Pollution,” “Pollutant,” “Air pollution,” “Microparticles,” “Particulate matter,” “Environment,” “Ambient,” “Occupational,” “Occupational exposure,” “Burn pit,” “Military,” “Deployment,” “Low molecular weight,” “Low molecular weight irritants,” “Lung,” “Chronic obstructive pulmonary disease,” “Lower respiratory,” “Mucociliary clearance,” “Respiratory tract changes,” “Histopathologic changes,” “Airway disease,” “Endotypes,” “Wildfire,” “Landscape fire,” “Wildfire smoke,” Landscape fire smoke,” “Mold,” “Mold exposure,” “Microplastics,” and “Inhalational exposure.” Inclusion criteria included studies evaluating the effects of environmental exposures on sinonasal disease prevalence, severity, recalcitrance, and postoperative outcomes. Non-English articles were excluded. Abstracts were screened and full texts imported into Rayyan™ for review and categorization. 11 Similar articles and references for each included study were explored for additional potential studies.
Tobacco Smoke
Smoking remains the number 1 cause of preventable death and disease worldwide, being directly responsible for 90% of lung cancer deaths and 80% of deaths due to chronic obstructive pulmonary disease (COPD).12,13 In the lower respiratory tract, cigarette smoke (CS) has been shown to disrupt epithelial barriers, 14 decrease mucociliary clearance, 15 promote goblet cell hyperplasia, 16 and generate oxidative stress. 17 These molecular and cellular changes then manifest as COPD and chronic bronchitis, which contribute to the 490,000 deaths each year from CS. 12 Serving as the first line of defense against inhaled pathogens for the lower respiratory tract, it stands to reason that the upper respiratory tract should be similarly affected.
Indeed, the impact of CS on the upper respiratory tract has been well-studied and its mechanisms mirror that of the lower respiratory tract. In a 2018 systematic review by Christensen et al, 11 of 13 studies showed an increased prevalence of CRS in primary smokers, with 3 studies showing a dose–response relationship. 18 A 2012 systematic review supported this finding demonstrating that smoking was positively associated with self-reported CRS in women with and without a history of allergy. CS was only associated with self-reported CRS in men without a history of allergy. 19
The impact of second-hand smoke exposure is less definitive. Hur et al published a systematic review of passive CS exposure and CRS in adults and children, reporting on a heterogeneous group of studies including surveys with self-reported CRS histories, as well as case–control studies with objective diagnoses. They demonstrate that most of the studies (68.4%) included in their systematic review found a positive association between second-hand smoke and CRS, even though the largest included study of 20,050 subjects (60.2% of all included subjects) found no association. Notably, of the 6 studies with objective diagnostic criteria for CRS (CT or nasal endoscopy), 5 found a positive association. 20 Three of the 6 studies in Christensen et al’s systematic review (different studies from those included by Hur et al) found a positive association, including 1 study of 3001 children <10 years old that showed a 69% prevalence of physician-diagnosed CRS in those exposed to second-hand smoke, compared to only 1.2% in those not exposed. 18
The pathogenesis of tobacco smoke-induced disease in the upper respiratory tract mirrors that of the lower respiratory tract. Fifteen of 16 studies in a 2020 systematic review on nasal mucociliary clearance in active smokers showed significantly decreased mucociliary clearance in active smokers compared to non-smokers. 21 Additionally, numerous studies have reported on reduced epithelial ion transport, increased mucous viscosity and altered ciliary beat frequency (CBF) secondary to smoke exposure.18,19,22 Curiously, there appears to be an initial compensatory increased CBF that then decreases with continued exposure, as evidenced by an increased CBF in those exposed to second-hand smoke relative to non-smokers, and an observed dose–response seen across multiple studies.19,22,23
Surgical outcomes in active smokers and those exposed to second-hand smoke are significantly worse than non-smokers. In adults, subjective symptomatic improvement following surgery is significantly less in smokers than non-smokers, as supported by 9 of 13 included studies by Christensen et al. Moreover, all included studies of children exposed to CS exhibited worse surgical outcomes compared to those unexposed. 18
As demonstrated, tobacco smoke exposure is associated with an increased prevalence of CRS, worse surgical outcomes and pathophysiological changes similar to those seen in severe lower respiratory pathology. It remains a significant contributor to sinonasal disease and its impact must be considered in the treatment of CRS patients.
Occupational Exposures
Occupational inhalational exposures have long been theorized to play a role in the onset and worsening of CRS and population-based studies generally show a positive association. In a 2016 cross-sectional study performed across 8 different regions in China, several occupational-related exposures were found positively associated with CRS symptoms, which were self-reported. On multivariate analysis, a significantly increased prevalence of CRS symptoms was found with histories of clearance-related jobs [adjusted odds ratio (aOR) 1.56; 95% CI 1.07-2.27], occupational exposure to dust (aOR 2.32; 95% CI 1.82-2.91), occupational exposure to poisonous gas (aOR 2.75; 95% CI 2.05-3.69), and carpets in the workplace (aOR 6.55; 95% CI 4.60-9.32). 24
Hox et al published a case–control study in 2012 in which they surveyed 890 endoscopic sinus surgery (ESS) patients for histories of occupational exposures, comparing their responses to 182 non-CRS controls. The rate of reported occupational exposures increased linearly with the number of surgeries in CRS patients, with 12% of non-CRS patients reporting exposure, 21% in those who had 1 ESS and 44% in those who had 4 or more. After controlling for asthma, atopy, and smoking, these rates yielded aORs of 1.64 in those having more than 1 ESS and 1.97 in those needing 2 or more, suggesting that prior occupational exposures may lead to increased disease severity. 25
An association between low-molecular weight (LMW) agent and irritant exposure and CRS risk has been purported in numerous studies. Examples of LMW agents include isocyanates, acrylates, aldehydes, and anhydrides, while irritants include acid aerosols, bleach, dusts, thinners, ammonia, etc. 26 Hox et al found that LMW allergen and irritant exposure increased linearly with increasing numbers of surgeries. 25 In a very similar study, Dietz de Loos et al sampled CRS patients in a cross-sectional study in the Netherlands, again inquiring about previous occupational exposures by survey. Of the 410 respondents, 94.2% had undergone at least 1 ESS, of whom 30% reported a relevant occupational exposure as determined by an occupational medicine physician. This was significantly higher than the 4.8% response rate in the CRS patients who had not undergone an ESS. Of those reporting exposures, 70% recall exposure to irritants. 27 Thilsing et al also reported on an association between LMW agents and self-reported CRS in their survey of 3099 Danish adults, though this did not reach significance (aOR 1.29; 95% CI 0.87-1.90). 28 Last, Velasquez et al stratified CRS patients by occupational exposure to vapors, gases, dusts, fumes, fibers, and mists, finding that those with exposure were more likely to undergo ESS (34.5% vs 20.6%, P = .038) and had higher steroid doses (mean, 1095 vs 644.1 mg, P = .015) than unexposed CRS patients. 29
While single studies have purported associations between various exposures and CRS, many of the published studies have been flawed with potential recall bias and the lack of consistent definitions, both in exposures and diagnosis. Sundaresan et al published a systematic review in 2015 including 41 studies, none of which used CRS definitions consistent with current guidelines. Furthermore, exposure assessments were inconsistently defined and made a meta-analysis impossible. While the results of 2 similar studies could be pooled and used to conclude that grain, dairy, and swine farming was not associated with an increased risk of CRS, the authors were more struck by the inconsistent disease definitions, inaccurate exposure histories, predominance of cross-sectional studies, and the healthy worker bias that limited the field of research. 30 These findings were echoed in a 2024 scoping review by Monk et al, who noted substantial evidence for an association between occupational exposures and CRS while lamenting the variations in diagnostic criteria and heterogeneous populations. 31
One subset of occupational inhalational exposure warrants particular attention. Military personnel and first responders are asked to willingly expose themselves to some of the most extreme environments in the line of duty, many of which have been shown to result in significant morbidity. While cardiopulmonary pathologies tend to dominate the literature, sinonasal sequelae of inhalational exposures in military, and first responders is emerging.32-35 Following the World Trade Center disaster, 45.1% of New York City firefighters who responded to ground zero possessed symptoms of rhinosinusitis one year after exposure, the number increasing to 47.8% at year 4. This is compared to a 4.4% incidence before the disaster. Interestingly, de la Hoz et al found that the prevalence of exposure-related upper airway disease following the World Trade Center disaster, which includes rhinosinusitis, did not vary by occupation, while lower airway disease was primarily limited to first responders. This suggests that a secondary sinonasal disease may be more ubiquitous following such an event and/or require less of an exposure. 36 Weakley et al found a dose-dependent relationship between timing of exposure relative to the collapse of the World Trade Center in Fire Department of New York (FDNY) firefighters and incidence of new-onset CRS diagnosis confirmed by CT or nasal endoscopy. They published a 23.5% incidence in the high exposure group (those that arrived the morning of September 11), 19% in the medium (arrived afternoon or anytime on September 12), and 12.4% in the low exposure group (arrived any day between September 13 and 24). 37
Military personnel deployed to Iraq and Afghanistan were exposed to significant environmental hazards, from air pollution to silica-laden dust to burn pits sanctioned for the disposal of everything from biomedical waste to munitions.38,39 Returning deployers reported increased nasal congestion, postnasal drip, rhinorrhea, and hyposmia and increased odds of sinusitis compared to non-deployed veterans (OR 1.3; 95% CI 1.13-1.49).40,41 Maccarone et al noted an association between pesticide application during deployments and increased odds of rhinitis, though this was not significant (OR 1.21; 95% CI 0.93-1.50). 42 A 2022 cross-sectional study evaluated subjective symptoms and objective sinus disease in Active Duty service members with and without self-reported burn pit exposure. Patients with burn pit exposure had significantly higher SNOT-22 scores (49 vs 31, P < .001), higher rates of CRS with nasal polyposis (CRSwNP; 27.8% vs 8.5%, P = .004), allergic rhinitis (61.1% vs 23.9%, P < .001), and prior ESS (32.1% vs 11.1%, P = .005), as well as worse Lund–Kennedy nasal endoscopy scores (3.3 vs 1.7, P = .003) than those who deployed but did not have burn pit exposure. This study was the first to associate subjective and objective sinonasal pathology with burn pit exposure. 43
There has been little published research to date investigating mechanisms for CRS pathogenesis or exacerbations following occupational inhalational exposure. In an attempt to standardize exposure histories for research purposes and ameliorate this knowledge gap, Worden et al recently published on a novel survey entitled Sinonasal Occupational and Airborne Pollutant Exposure survey. In their 2024 pilot study, they administered this exposure survey preoperatively to 27 ESS patients and found that high exposures correlated with higher preoperative CRS-related morbidity and likelihood of asthma. RNA sequencing data revealed a distinct subgroup of high exposure patients within the CRSwNP cohort that clustered together with 2113 differentially expressed genes (DEGs) on transcriptome analysis. Of the reported exposures, specifically smoke and fumes had the greatest impact on transcriptome analysis with 1126 DEGs. 44
While the quality of the published research is generally lacking, there is relative consistency in the literature that occupational inhalational exposure is associated with an increased prevalence of CRS and potentially increased disease severity. While ethics and clinical equipoise likely prohibit the randomized-controlled trials needed to conclusively link these exposures and outcomes, there is abundant evidence of association. That said, future research in this field must not neglect these limitations as we refine our understanding of the pathophysiology for therapeutic purposes. Well-designed prospective studies can minimize selection and recall bias. Direct measurement of inhalational exposure can limit heterogeneity and using predetermined definitions of disease will maximize generalizability. Collaboration between academic institutions with robust research infrastructure and government entities with abundant data (eg, between academic medical centers and the Department of Defense) offer such possibilities. While the association between exposure and disease state is present, more therapeutic targets are still needed and the quality of research in this area must improve accordingly.
Pollution and Particulate Matter
In the ongoing effort to combat the effects of air pollution, the U.S. Environmental Protection Agency has identified 6 criteria air pollutants and provided air quality standards for each: Ozone, PM <10 and 2.5 μm (referred to as PM10 and PM2.5, respectively), carbon monoxide, lead, sulfur dioxide, and nitrogen dioxide. 45 These pollutants have been extensively linked to worsened asthma severity, increased asthma-related emergency department visits and contribute both to the development of COPD and an increased risk of cardiovascular mortality in COPD patients.46-48
As research has progressed in the upper respiratory field, similar associations have been found between air pollution and the onset and severity of CRS. In contrast to the published research on occupational exposures, which relied heavily on self-reported exposures and was subject to heterogeneity and recall bias, recent pollution research has leveraged land use regression (LUR) modeling, which incorporates local air quality sampling, topography, and meteorological data to provide higher fidelity exposure estimates at patients’ provided home addresses. Not without its own limitations, LUR modeling relies on fixed periods of air sampling which is extrapolated across longer periods of time, while also failing to account for patient-level variables such as daily movement, masking, home heating, ventilation and air conditioning (HVAC) or filtration systems, etc. In essence, it represents population-level exposure data to correspond with population-level outcomes. Using LUR modeling, Mady et al found that PM2.5 in Pittsburgh and the surrounding county was significantly associated with the need for ESS in CRS without nasal polyps (CRSsNP) patients, further noting that for each 1 unit increase in PM2.5, there was observed a 1.89-fold increased risk of CRSsNP patients requiring additional ESS. Black carbon (BC), an aerosol component that constitutes a proportion of PM, also showed a dose–response association with SNOT-22 scores in CRSsNP patients, with each 0.1 unit increase in BC yielding a 7.97 unit increase in Sinonasal Outcome Test-22 (SNOT-22) scores (P = .008). There was no such association in CRSwNP patients. 49
The different responses seen in CRSsNP and CRSwNP patients were further explored in a separate study published simultaneously by Mady et al, in which they further stratified CRS patients presenting with rhinitis by positive allergy testing. Allergy negative patients, regardless of polyp status, had significantly higher exposures to both PM2.5 (11.32 vs 11.07 μg/m3, P = .03) and BC (0.81 absorbance vs 0.76, P = .04) than their allergic counterparts. This trend held true within the CRSwNP cohort, with allergy negative polyp patients having higher PM2.5 exposures than polyp patients with positive allergy testing (11.48 vs 11.09 μg/m3, P = .032). 50 Taken together, these studies suggest that air pollution and PM2.5 may play a role in worsened CRS severity in CRSsNP patients, while also contributing to non-allergic rhinitis symptomatology regardless of polyp status.
In a 2021 letter to the editor, Zhang et al corroborated the Pittsburgh findings associating pollution and CRS in a large case–control study performed in Baltimore. PM2.5 levels measured using LUR modeling were compared in CRS patients (n = 2034) and non-CRS controls (n = 4068), both confirmed objectively with CT and/or nasal endoscopy, in the months leading up to diagnosis. CRS was more likely to be diagnosed in patients exposed to higher PM2.5 concentrations across all time periods (12, 24, 36, and 60 months) and within each anatomic location (eg, OR of ethmoid sinusitis 2.90, 95% CI 2.00-4.21 for each 5 μg/m3 12 month PM2.5 increase). 51 Peeters et al reported similar findings in their 2022 study performed in Belgium, in which they demonstrated higher CRS symptoms (measured on a 1-100 visual analog scale) with increasing exposure to PM2.5 and ozone in the spring and summer months. 52
Several mice and in-vitro studies have attempted to characterize the mechanism of pollution-mediated CRS. Ramanathan et al exposed mice to PM2.5 at levels lower than that found in major cities for 6 weeks and characterized nasal lavage fluid and histopathological changes. PM-exposed mice had higher numbers of macrophages, neutrophils and eosinophils in nasal lavage fluid, as well as higher expression of IL-1b, IL-13, eotaxin, and oncostatin M compared to mice exposed to ambient air. Serum albumin was also noted to be significantly elevated in nasal lavage fluid, a sign of epithelial barrier breakdown. 53 Patel et al coupled PM2.5 and ozone exposure with pathology specimens from CRS patients undergoing ESS, finding that greater ozone exposure was associated with increased inflammatory changes on logistic regression modeling. There was also a dose-dependent relationship between PM2.5/ozone exposure and eosinophilic aggregates and Charcot–Leyden crystals within the CRSwNP cohort. Curiously there was no such association between exposure and similar histopathologic changes in the CRSsNP cohort. 54 In a prospective study, Lubner et al demonstrated that preoperative PM2.5 levels correlated with increased IL-2, IL-5/IL-13, IL-12, and IL-21 in intraoperative mucous specimens taken from ESS patients. Tissue eosinophil counts also increased in line with increasing preoperative PM2.5 exposure. 55
Microsized inorganic particles represent an increasing health concern and the nasal cavity is no exception. Čábalová et al compared nasal tissue samples taken from CRS patients in the Czech Republic to non-CRS control specimens investigating the presence of microsized and nanosized inorganic particles, such as graphite, titanium dioxide, amorphous carbon, calcite, ankerite, and iron compounds, that may become inspired and deposit in sinonasal tissue. They found inorganic microsized and nanosized particles present in 90% of CRS patients along with histologic changes consistent with inflammation, whereas inorganic compounds were only found in 20% of cadaveric non-CRS controls with no evidence of inflammation. 56 Taş et al performed a prospective study comparing the nasal lavage fluid of 50 CRSsNP patients with 30 non-CRS controls, finding that CRS patients had significantly more microplastics in their lavage fluid (P < .001). 57 A response letter astutely pointed out the inherent confounder that CRS patients undoubtedly use more nasal sprays and irrigations (almost certainly from plastic bottles) than non-CRS controls and that this finding in no way implies causation. 58 Nonetheless, these studies underscore the potential role of microsized particles in CRS pathogenesis and emphasize the need for additional research in this largely unexplored field.
As in the pulmonary literature, large amounts of data corroborate that air pollution and microparticle exposure is associated with increased sinusitis symptoms and prevalence of diagnosed CRS. The Pittsburgh studies suggest the possibility that air pollution and microparticle exposure may drive a symptomatology independent of allergies and more pronounced in CRSsNP patients, though this nuanced finding has yet to be corroborated in other studies and in other geographic areas. While mechanisms are still being established, Otolaryngologists and primary care providers must not be so quick to dismiss patient concerns that the inspired air may be contributing to illness.
Wildfire Smoke
Thanks to effective legislation and air quality standards, PM2.5 levels declined nationwide between 2009 and 2018. However, concomitant with this decline has been a 350% increase in person-days of heavy density wildfire smoke exposure across the United States—wildfire smoke that now accounts for between 32% and 44% of PM2.5 emissions nationwide.59,60 Hospital and emergency room admissions data from recent wildfires in the western United States have revealed staggering morbidity secondary to this smoke exposure. While ambient PM2.5 was decreasing, PM2.5 attributable to wildfire smoke accounted for a 10% increase in respiratory-related admissions in southern California between 1999 and 2012. 61 A 2021 systematic review and meta-analysis on the respiratory impact of wildfire smoke in children pooled 4 studies encompassing 13,258 children to find a positive association between hospitalization for any respiratory cause and wildfire smoke. Pooling 557,454 participants from 8 studies demonstrated a positive association between wildfire smoke exposure and respiratory visits to the emergency department. 62 Five out of 6 studies in a 2015 systematic review demonstrated an association between wildfire smoke and hospital admissions for cardiovascular disease. 63 More specifically, patients with underlying cardiac conditions in Maryland were found to have a 20% increased adjusted odds for a clinical encounter during “hotspot days” in which PM2.5 levels exceeded air quality standards secondary to a wildfire 2100 miles away. 64 PM2.5 secondary to wildfires has also been shown to be uniquely dangerous. Aguilera et al found that PM2.5 generated by wildfires was 10 times more harmful than ambient PM2.5, accounting for increased respiratory admissions even when at similar levels to ambient microparticle concentrations. For each 10 μg/m3 increase in wildfire-generated PM2.5, there was a 1.3% to 10% increase in respiratory admissions compared to only 0.67% to 1.3% increase due to a commensurate change in ambient PM2.5.
Noticeably absent are population-based and epidemiological studies assessing similar exposure-outcome associations in CRS. Henry et al found that itchy/watery eyes, sneezing, sore throat, and rhinitis had a positive association with wildfire smoke in their 2021 systematic review, though this evidence was of low certainty. 62 In a 2023 review on ambient and wildfire air pollution, rhinosinusitis, and olfactory dysfunction, Yu et al were unable to cite any primary studies pertaining to CRS and wildfire exposure. However, they put forth that they are “currently performing a large-scale epidemiological study pairing exposure (wildfire air pollution) to outcome (prevalence of CRS, severity of CRS symptoms, outpatient clinic visits for CRS, or medication and surgery utilization for symptom management).” 65
Curiously, there is perhaps more mechanistic in-vitro and animal data supporting a relationship between wildfire smoke and upper respiratory pathology, for once preceding the outcome-exposure data. Beginning in the lower respiratory tract, wildfire-generated PM has been shown to initiate neutrophilic and eosinophilic asthma via IL-17A release and the activation of aryl hydrocarbon receptor (AhR) in epithelial, dendritic, and T cells. 66 PM exposure in mice mimicking landscape and vegetation fire smoke generated airway hyperresponsiveness but without commensurate increases in inflammatory cell infiltrate on bronchoalveolar lavage. This is believed to be mediated by changes in calcium oscillation pathways in airway smooth muscle and if correct, would represent a steroid-insensitive phenotype. In this model, short-term landscape fire smoke exposure actually decreased the expression of AhR, as well as IL-6 and TNF-α. 67 In a human bronchoalveolar cell line, concentrations of smoldering plastic incineration emissions (PIEs), a more authentic representation of urban wildfires and burn pits, induced cellular oxidative stress as evidenced by increased glutathione oxidation, as well as upregulation of AhR. 68
Rogers et al also exposed human nasal epithelial cells to PIEs, finding an upregulation of inflammatory cytokines, such IL-8 and IL-1b, induced by exposure to high concentrations of smoldering PIEs (burned at 500°C), as well as both low and high concentrations of flaming PIEs (burned at 640°C). IL-4 and IL-13 secretion was increased in various conditions, while reverse transcription of RNA isolates also showed increased expression of IL-6, IL-10, and IL-1b. The authors conclude that the observed inflammation, oxidative imbalance, impaired mitochondrial function, and transcriptomic alterations in nasal epithelial cells are consistent with the development of upper respiratory disease. 68
With worldwide exposure to wildfire smoke increasing over the past 2 decades, a trend that is expected to continue, more research into wildfire smoke and chronic sinus disease is desperately needed. 69 As was the case with literature evaluating the effects of pollution, microparticles, and occupational exposures, there is a greater depth of literature and exposure-outcome data in the cardiopulmonary field. If history is any indication, however, similar outcomes will likely be found in the upper respiratory tract. Mice and in vitro studies performed in labs already primed with models for studying pollution have provided early indications of the inflammatory changes we are likely to behold in population studies of wildfire smoke and CRS. The gaps must now be filled in.
Gaps and Future Directions
As much of the current outcome data is derived from population-level research, more deliberate, well-designed studies are required if we are to achieve the level of knowledge necessary for therapeutic intervention. Exposures must be better characterized and coupled with patient-level evaluation of histologic, molecular, and transcriptomic changes. Addressing current gaps in exposure-outcome data in wildfire smoke would provide patient-centered justification for continued mechanistic research. Future research must also ensure consistency of disease definitions and diagnostic criteria. Workman et al estimate a positive predictive value of 38.9% when relying upon self-reported symptoms to diagnose CRS, emphasizing the need for objective evaluations to ensure generalizability. 70 Microplastics remain an under-explored field in the CRS domain and with the prevalence of plastic delivery vehicles for intranasal medications, it must not be overlooked. Lastly, based on the unified airway theory, sinonasal researchers would do well to maintain an eye on the lower respiratory literature. After all, the air believed to have caused the increased emergency room visits for asthma exacerbations once passed through the upper airway. Such research into the complex interconnection between environment and host can only bring us closer to the identification of “treatable traits.”
Conclusion
As the pathogenesis of CRS continues to be investigated, there is ample evidence for the association between environmental exposures and the onset and worsening of sinonasal disease. Tobacco smoke, occupational inhalational exposures, air pollution, PM, and wildfire smoke constitute but a fraction of the prospective potentiators of disease as the upper respiratory tract filters the air we breathe. While the present literature linking environmental exposures and CRS may be flawed, the general associations established across time and space should be more than sufficient for the education and counseling of patients. Therapeutic targets will follow with better refinement of research, though we must persist in following the smoke. After all, where there is smoke, there is fire (Table 1).
Summary of Significant Environmental Contributions to Chronic Rhinosinusitis.
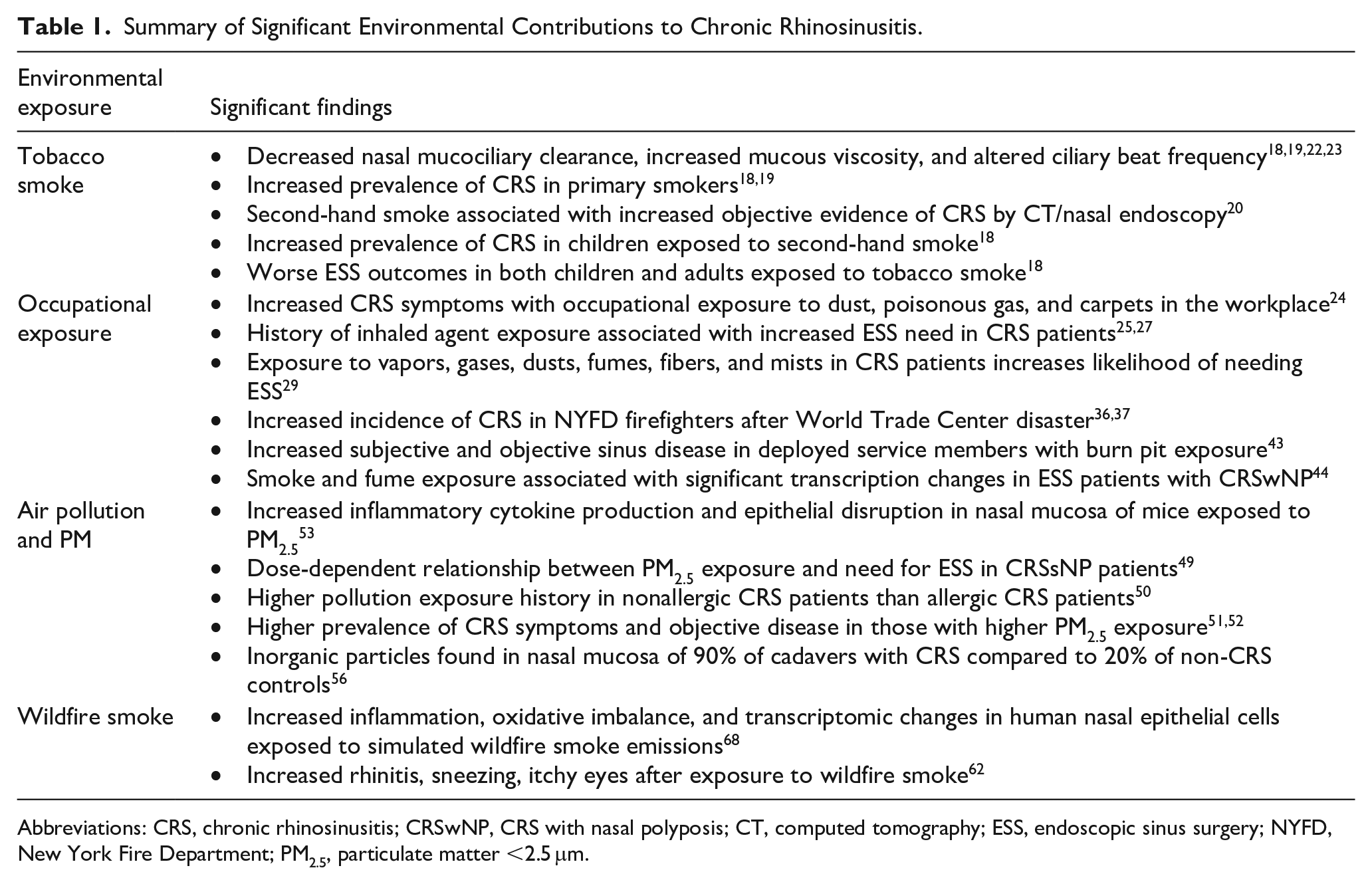
Abbreviations: CRS, chronic rhinosinusitis; CRSwNP, CRS with nasal polyposis; CT, computed tomography; ESS, endoscopic sinus surgery; NYFD, New York Fire Department; PM2.5, particulate matter <2.5 μm.
Footnotes
Author’s Note
The views expressed in this article reflect the results of research conducted by the author and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the United States Government. Dr. Hill is a military service member. His work was prepared as part of his official duties. Title 17 U.S.C. 105 provides that “Copyright protection under this title is not available for any work of the United States Government.” Title 17 U.S.C. 101 defines a United States Government work as a work prepared by a military service member or employee of the United States Government as part of that person’s official duties.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.