
Abstract
Objective:
To investigate associations between traffic-related air pollution exposure and inflammatory markers, demographic characteristics, and quality-of-life measures in patients with chronic rhinosinusitis (CRS).
Methods:
Patients who underwent surgical treatment for CRS between September 2015 and September 2024 were enrolled in a longitudinal cohort study. Geospatial analysis quantified the total length of highways and arterial roads, as well as daily vehicle and truck traffic volumes, within a 1-km radius of patients’ home zip codes. Mucus cytokine levels were assessed using multiplex bead assays. Statistical analyses included Spearman correlations and multivariate linear regression to assess associations between traffic exposure and demographics, inflammatory cytokine levels, and quality-of-life scores.
Results:
A total of 567 patients with complete data were included. Proximity to arterial roads was significantly associated with patient race (P = .0084). In patients with CRS with nasal polyps, increased arterial road length was associated with lower IL-2 levels (P = .0313). Multivariate analysis did not demonstrate consistent or significant associations between traffic exposure and cytokine levels.
Conclusion:
Multivariate models did not show associations between traffic exposure and select inflammatory cytokines, suggesting a limited role of traffic-related emissions in driving airway inflammation in CRS, though environmental disparities may influence exposure patterns.
Level of Evidence:
Level 3.
Keywords
Introduction
Chronic rhinosinusitis (CRS) is a highly prevalent disease with large social and financial burdens. The condition is defined by at least 12 weeks of persistent symptoms, supported by endoscopic or radiographic evidence of sinusitis. 1 As one of the most common chronic airway diseases, CRS affects approximately 8% of the global population, including 40 million Americans, with prevalence continuing to rise.2 -4 Symptoms (like nasal congestion, facial pressure, rhinorrhea) and secondary consequences (like sleep impairment, anxiety, and depression) of CRS can decrease patients’ quality of life.5 -7 In the United States, CRS imposes substantial economic burdens, with direct healthcare costs estimated at USD 10 to 13 billion annually and indirect costs, including missed workdays, absenteeism, and reduced productivity, exceeding USD 20 billion per year.8 -11
The pathophysiology of CRS is influenced by a combination of genetic, environmental, and host-microbiome factors. 12 Among environmental contributors, air pollution, particularly particulate matter (PM), is strongly associated with the incidence, prevalence, and severity of CRS.13,14 PM and other pollutants arise from chemical reactions involving emissions from sources such as industrial plants and vehicles. 15 These pollutants generate reactive oxygen species, which cause DNA, lipid, and protein damage and amplify inflammatory responses.16 -19 Despite increasing traffic volumes, research directly linking CRS to traffic exposure remains limited. 20 In this study, we analyzed the proximity of patients’ home addresses to interstates and arterial roads, along with vehicle and truck traffic volumes. The data were then compared with demographic information, inflammatory markers, and quality-of-life measures to explore potential relationships, with the hypothesis that increased traffic exposure would be associated with increased sinonasal inflammation.
Methods
Study Population
This study received approval from the Institutional Review Board of Vanderbilt University Medical Center (#130114). Adult patients presenting to rhinology clinics at the Vanderbilt Asthma, Sinus, and Allergy Program or the Vanderbilt Bill Wilkerson Center between September 2015 and September 2024 were identified and enrolled in a longitudinal prospective cohort study after obtaining informed consent. The diagnosis of CRS was made according to the guidelines outlined in the European Position Paper on Rhinosinusitis and Nasal Polyps, as well as the International Consensus Statement on Allergy and Rhinology.21 -23 Chronic sinusitis with nasal polyps (CRSwNP) was diagnosed based on the presence of nasal polyps observed through nasal endoscopy in a clinical setting or during endoscopic sinus surgery. Patients were excluded if they had odontogenic rhinosinusitis, suspected mycetoma, current monoclonal antibody therapy, systemic steroid use within 1 month of surgery, cystic fibrosis, or known autoimmune disease.
Patient age, sex, race, and ethnicity were extracted from the medical record. Each patient’s preoperative Lund-McKay score was calculated based on a high-resolution computed tomography scan of the paranasal sinuses taken within 3 months before surgery. Patient-reported symptom severity was evaluated using the 22-item sinonasal outcome test (SNOT-22). 24
Average annual daily traffic (AADT) data were then obtained from the U.S. Department of Transportation Federal Highway Administration using the addAadtData package in R. Patient home addresses were first converted to latitude and longitude coordinates using tidygeocoder. AADT data within a 1000-m radius from a patient’s home address coordinates were then estimated. Key traffic data obtained included the total length of interstates, expressways, and freeways (TLIEF; meters), the total length of arterial roads (meters), average number of daily vehicles multiplied by the length of freeways/arterial roads (vehicle-meters), and the average number of daily trucks multiplied by the length of freeways/arterial roads (vehicle-meters).
Mucus Collection and Cytokine Measurement
The procedure for mucus collection and cytokine measurement has been previously described.25 -27 Briefly, cytokine levels from mucus samples collected from the middle meatus of the nasal cavity during endoscopic sinus surgery were analyzed using a multiplex flow cytometric bead assay (BD Sciences). Polyurethane sponges (Summit Medical) were placed in the middle meatus under endoscopic visualization and retrieved after 4 minutes for immediate analysis. Cytokine concentrations in each specimen were measured using a multiplex flow cytometric bead assay (BD Sciences). Cytokines measured included IL-1β, IL-2, IL-4, IL-5, IL-6, IL-7, IL-8, IL-9, IL-10, IL-12, IL-13, IL-17A, IL-21, tumor necrosis factor-α, interferon-γ, eotaxin, and regulated-upon-activation, normal T-cell-expressed and secreted. Cytokine values below the detection level were imputed with the minimum detectable value for the assay.
Statistical Analysis
Cytokine values were log-normalized to transform values into a normal distribution for subsequent analysis. Spearman correlations were then used to assess univariate relationships between estimates of traffic volume and clinicodemographic. We then used a multivariate linear regression model to examine cytokine levels as a function of traffic values, with adjustments for comorbid asthma, allergic rhinitis, age, body mass index, income, and rurality. An alpha level of 0.05 was set as a prespecified threshold for statistical significance.
Results
Patient Characteristics
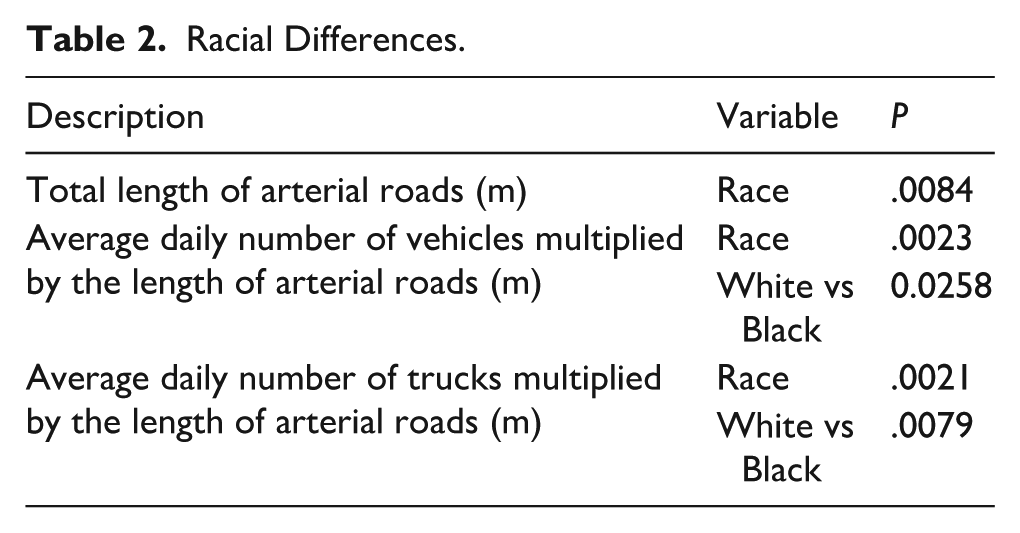
A total of 567 patients were included in this study. The study cohort was 44.4% female (n = 252), predominantly white (n = 484, 85.4%), and had a mean age of 46.2 (SD 15.8), as seen in Table 1. Allergic rhinitis was a common comorbidity, affecting 323 patients (57.0%). Asthma was also prevalent (n = 242, 42.7%). At 1000 m proximity, there were significant racial differences in exposure (P = .0084) in the context of total length of arterial roads, as seen in Table 2. The SNOT-22 psychological domain score also significantly differed for the TLIEF.
Patient Characteristics for All Patients.
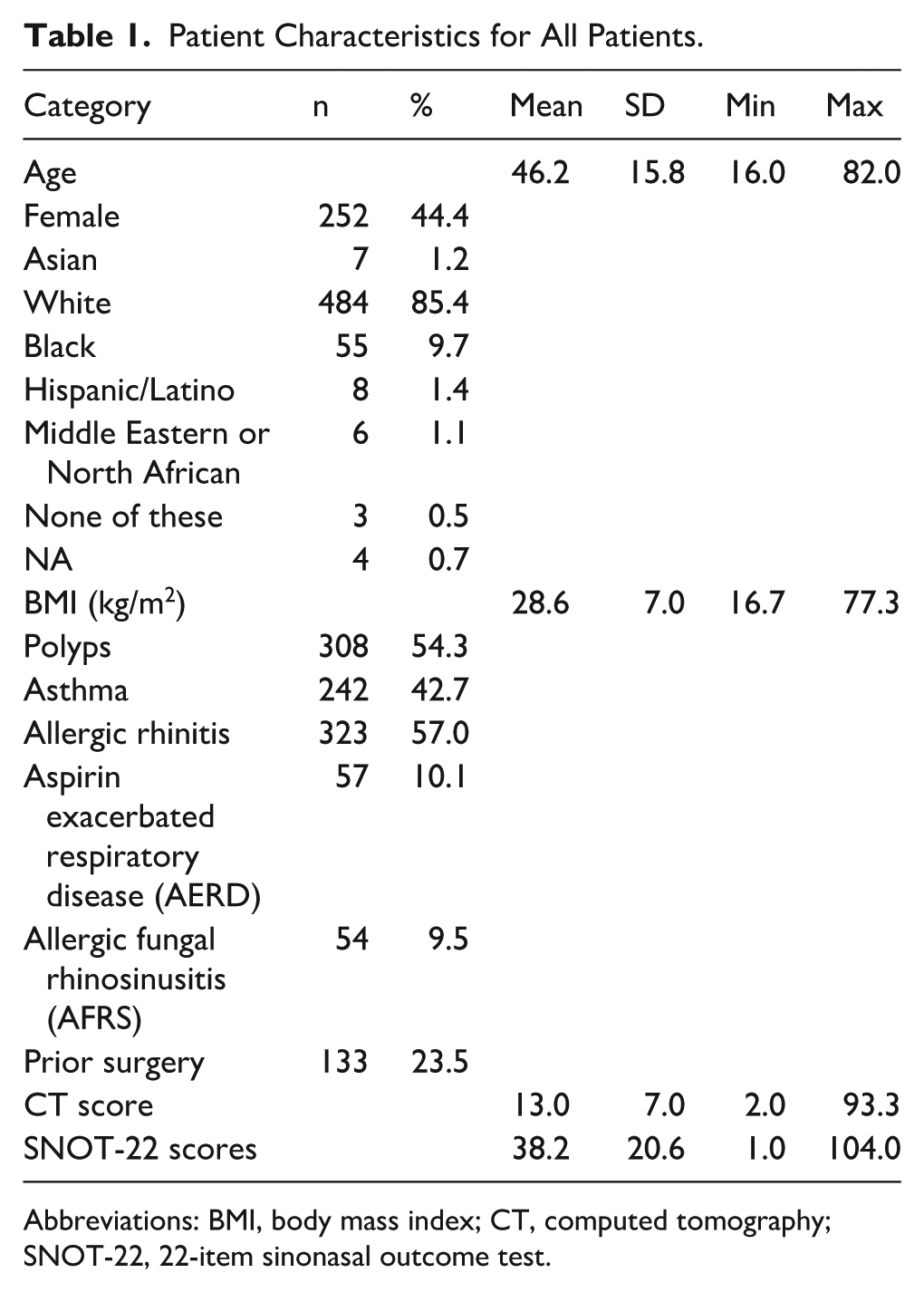
Abbreviations: BMI, body mass index; CT, computed tomography; SNOT-22, 22-item sinonasal outcome test.
Racial Differences.
Multivariate Cytokine Analysis
Multivariate analysis controlling for traffic exposure variables revealed that patients with CRSsNP exhibited significantly different levels of IL-12/IL-23p40 across multiple exposure metrics, including length moving (P = .00618), vehicle meters moving (P = .0155), and truck meters moving (P = .0106). In addition, IL-7 and IL-9 demonstrated significant associations with CRSsNP (P = .0324 and P = .00745, respectively). Among patients with CRSwNP, significant differences were observed in IL-2 (P = .02757) and IL-6 (P = .0166). A full summary of P-values for each cytokine and traffic exposure variable is provided in Tables 3 through 8.
Total Length of Arterial Roads.
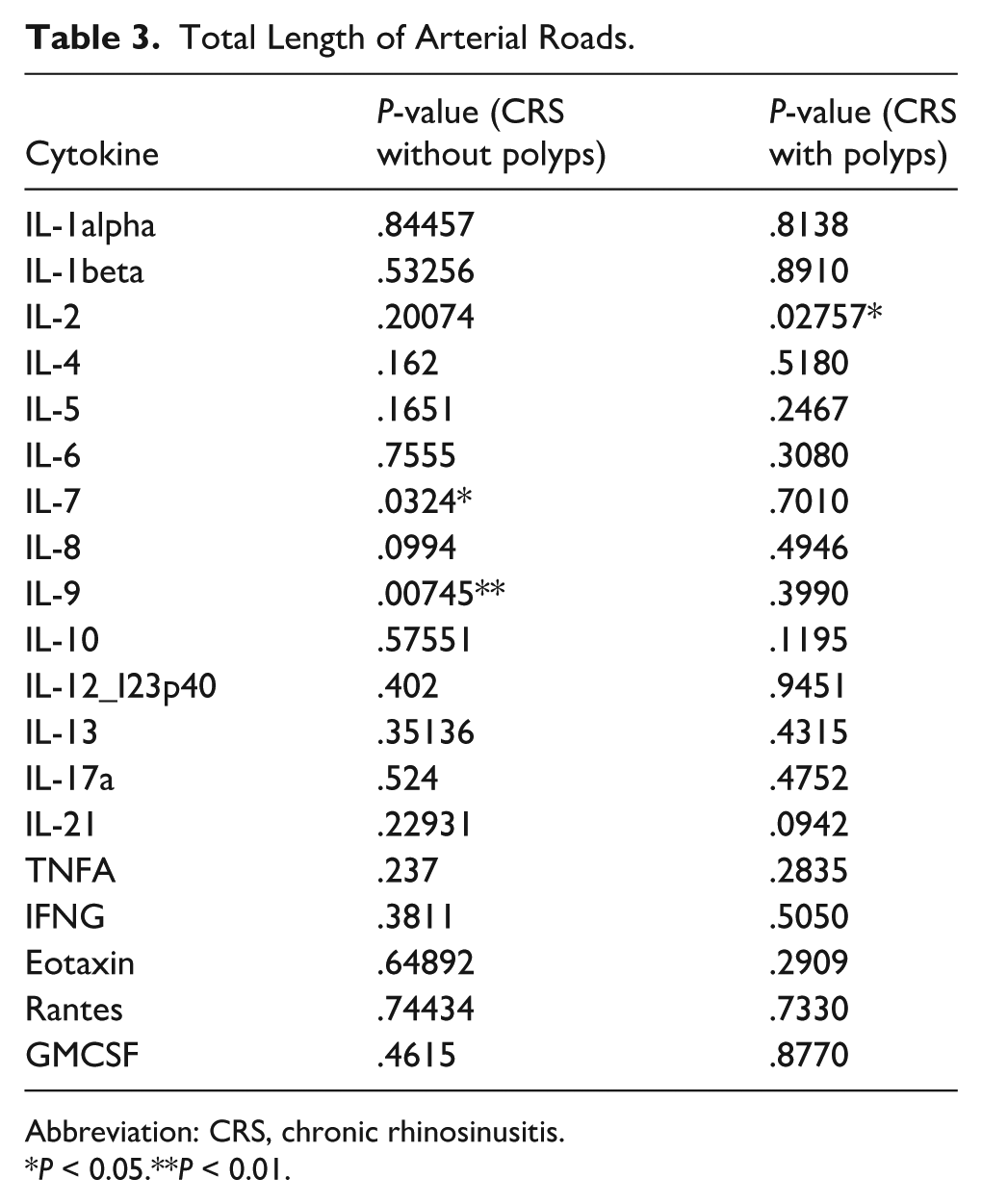
Abbreviation: CRS, chronic rhinosinusitis.
P < 0.05.**P < 0.01.
Total Length of Interstates, Expressways, and Freeways.
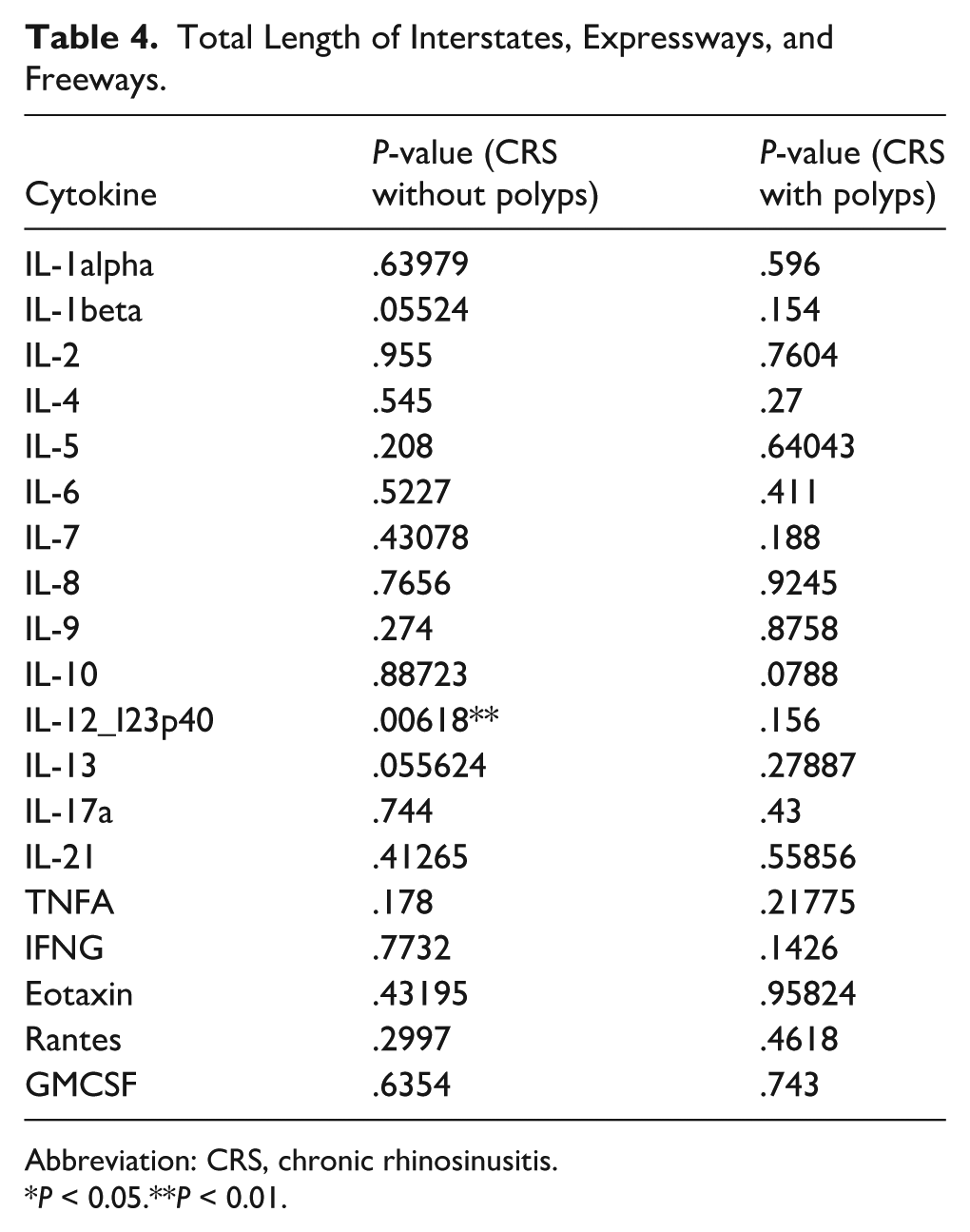
Abbreviation: CRS, chronic rhinosinusitis.
P < 0.05.**P < 0.01.
Average Daily Number of Vehicles Multiplied by the Length of Arterial Roads.
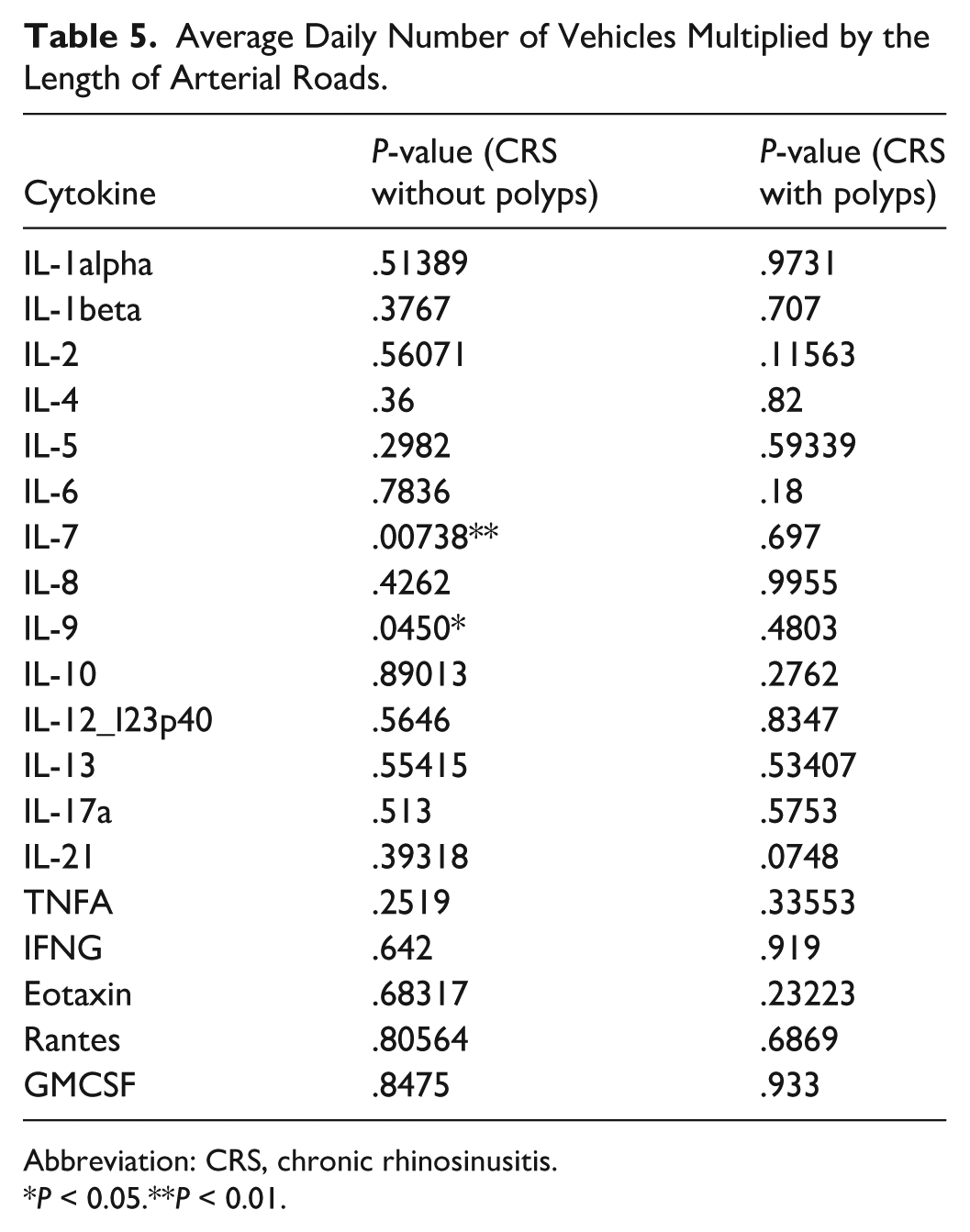
Abbreviation: CRS, chronic rhinosinusitis.
P < 0.05.**P < 0.01.
Average Daily Number of Vehicles Multiplied by the Length of Interstates, Expressways, and Freeways.
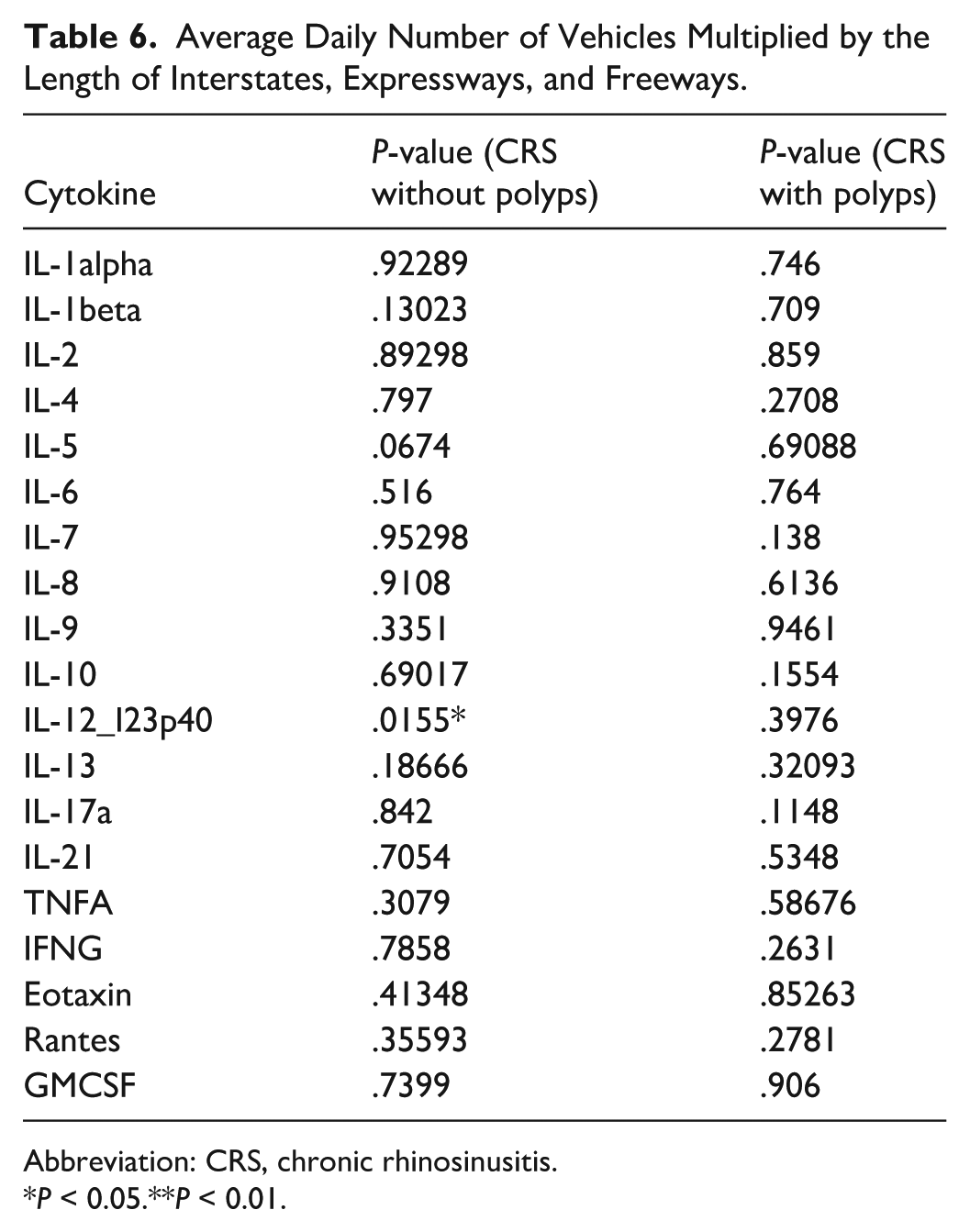
Abbreviation: CRS, chronic rhinosinusitis.
P < 0.05.**P < 0.01.
Average Daily Number of Trucks Multiplied by the Length of Arterial Roads.
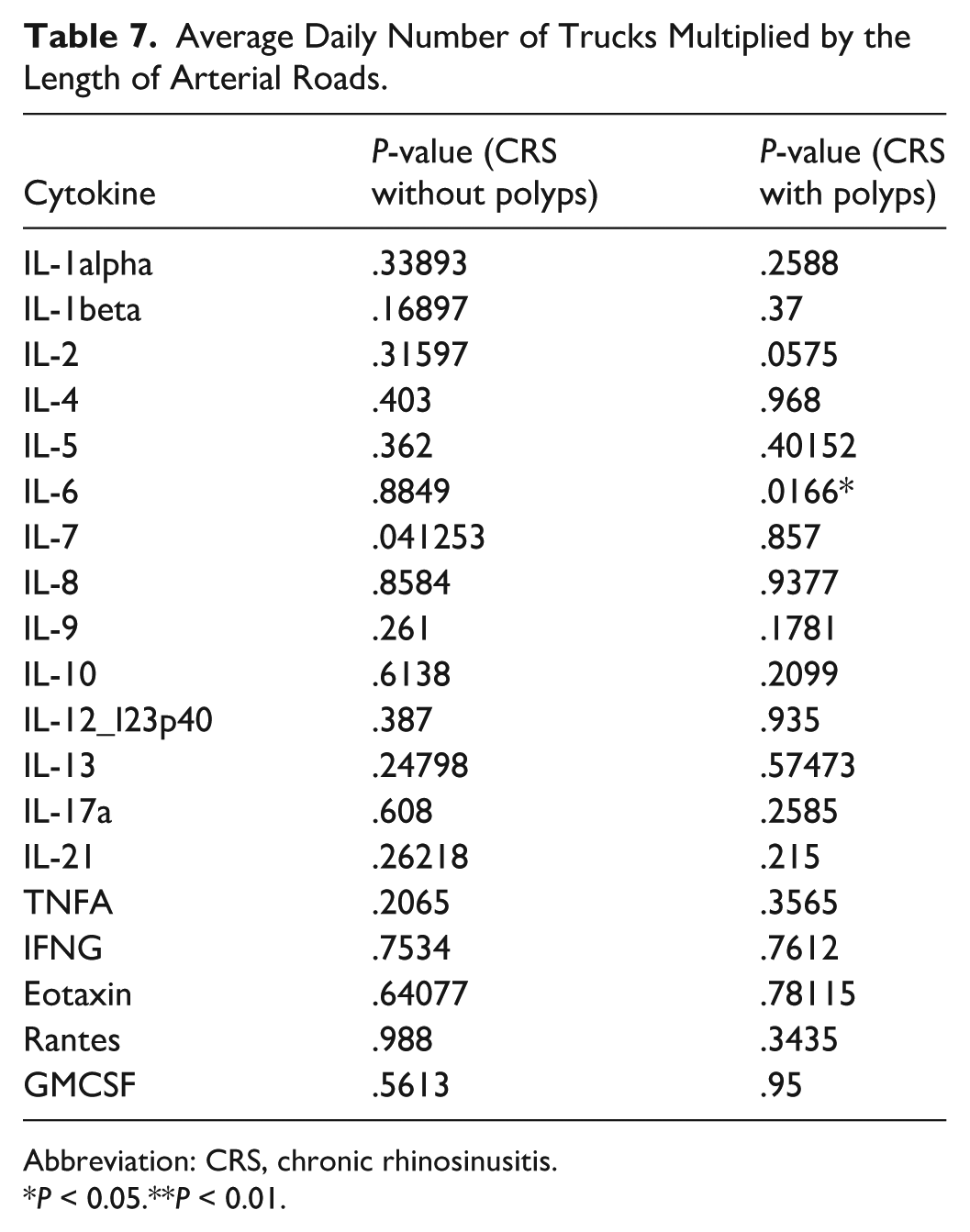
Abbreviation: CRS, chronic rhinosinusitis.
P < 0.05.**P < 0.01.
Average Daily Number of Trucks Multiplied by the Length of Interstates, Expressways, and Freeways.
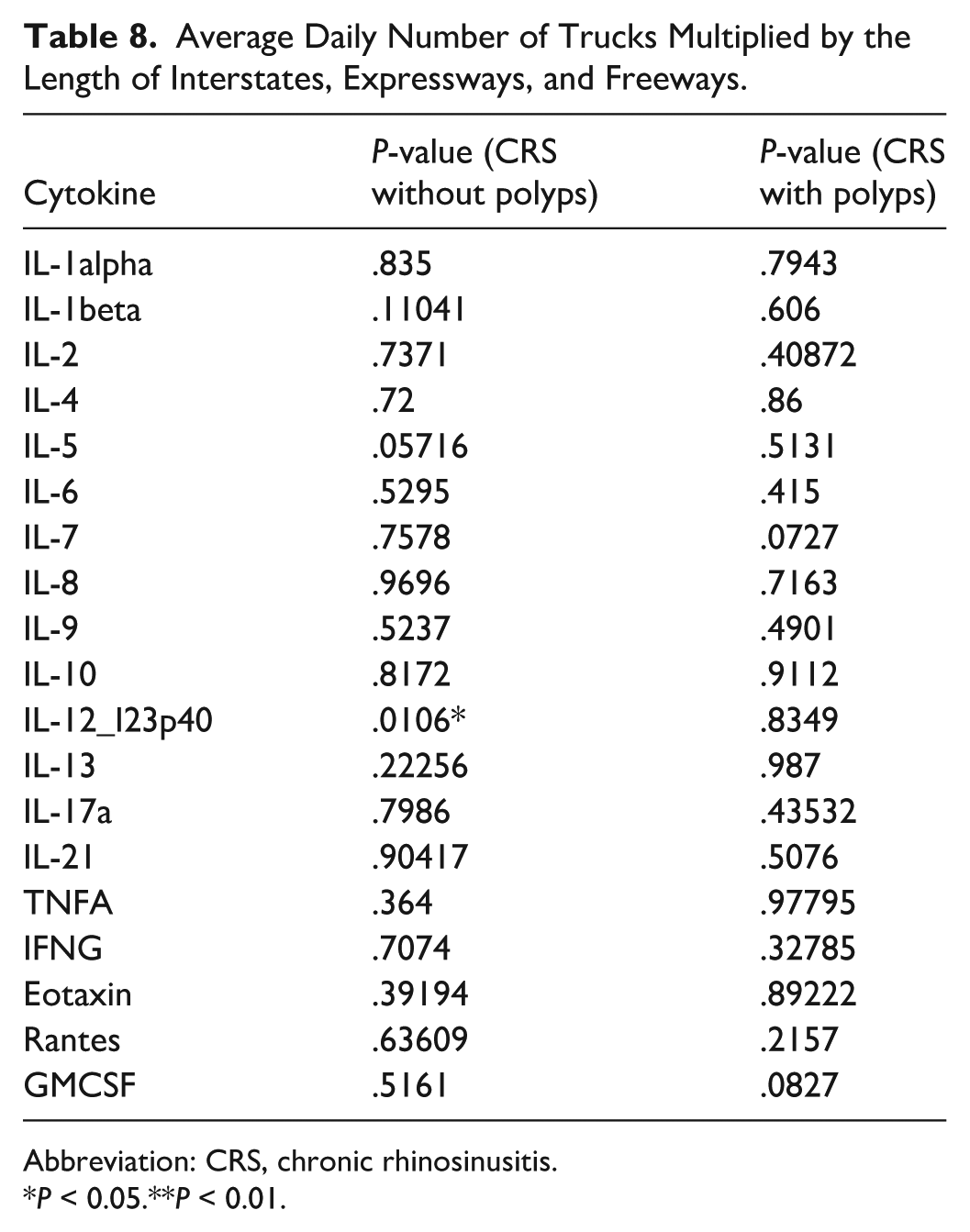
Abbreviation: CRS, chronic rhinosinusitis.
P < 0.05.**P < 0.01.
Discussion
In this study, we analyzed the proximity of patients’ home zip codes to interstates and arterial roads, along with vehicle and truck traffic volumes, and examined their associations with inflammatory markers and quality-of-life measures. We observed statistically significant differences in baseline SNOT-22 psychological domain scores based on roadway exposure, suggesting a potential impact on patient-reported outcomes. However, most cytokine findings were not statistically significant—particularly among patients with CRSwNP—indicating a largely negative study. These results are consistent with prior literature suggesting that traffic proximity may not be a major contributor to PM2.5-related inflammatory changes in CRS.
Combustion-related activities, such as vehicle emissions, produce particulate matter with a diameter of less than 2.5 μm (PM2.5).28 -30 PM2.5 has been related to adverse cardiovascular, neurological, and respiratory pathologies, including CRS.31,32 A study by Lubner et al. demonstrated that exposure to PM2.5 is significantly correlated with elevated levels of several inflammatory cytokines, including IL-2, IL-5/IL-13, IL-12, and IL-21, in patients with CRS. These correlations persisted even after adjusting for various confounding factors such as age, income, body mass index, rurality, polyps, asthma, and allergic rhinitis. 33 By contrast, our study found limited evidence of these associations, as multivariate models generally yielded non-significant or small effect sizes. This discrepancy may be explained by the relatively small contribution of traffic-related sources to overall PM2.5 levels—estimated at only 1.09% by Li et al.—suggesting that the more robust associations found in prior studies may reflect broader environmental exposures rather than traffic alone. 34 These findings provide limited support for traffic proximity as a major driver of PM2.5-related inflammatory changes in CRS.
Traffic emissions disproportionately affect people of color in the context of PM2.5 exposure and its health effects. Our study demonstrated a racial difference in proximity to high-traffic roads, whether arterial roads or highways. Several studies have demonstrated that African American populations in the United States are exposed to higher levels of PM2.5, largely due to traffic-related pollution.35,36 Other studies have shown that the majority of Hispanic neighborhoods were associated with higher air pollution exposures. 37 Exposure to PM2.5 in racial minorities increases the risk of developing CRS. 38 Correlations were noted between socioeconomic status, race, and air pollution exposure and CRS severity, post-surgical outcomes, and histopathologic changes in CRSwNP.39,40 These findings highlight the need to address environmental inequalities, as reducing traffic-related pollution could help mitigate its health impacts on affected communities.
Given the impacts of air pollution individuals’ health, increased efforts to regulate and control this pollution have the potential to impact millions of lives. Present approaches include the implementation of stricter vehicle emissions standards. For example, California’s aggressive vehicle emissions control policies from 2000 to 2019 resulted in a 65% reduction in statewide average PM2.5 exposure from on-road vehicles. However, despite these reductions, relative exposure disparities for people of color increased, driven mainly by light-duty vehicle emissions. 41 Other efforts target improved air quality monitoring, such as the regionalized air quality model performance hybrid method, which aims to improve exposure estimates and quantify exposure inequity to traffic-related air pollutants by integrating air quality observations with regional- and local-scale models. 42 The development of further strategies is crucial for addressing the persistent disparities in PM2.5 exposure among racial minorities, thereby reducing the associated health impacts such as CRS.
Our study is subject to several limitations. First, our analysis relied on patients’ home zip codes as a proxy for exposure, which may not accurately reflect personal exposure levels or variations in daily movement, workplace exposure, or time spent indoors. In addition, while we identified associations between roadway proximity and inflammatory markers, our study design does not establish causation, and other environmental or genetic factors may contribute to these findings. The lack of direct PM2.5 measurements further limits our ability to quantify specific pollutant exposure levels. The largely null results should be interpreted with caution, as they may reflect imprecise exposure measurement rather than a true absence of effect. More robust exposure metrics might reveal associations not detected here. Future research should incorporate more precise air-quality monitoring, personal exposure tracking, and longitudinal designs to better understand the long-term effects of traffic-related pollution on airway inflammation and disease progression. In addition, investigating potential interventions, such as urban planning strategies or air filtration measures, could provide actionable insights for mitigating the health burden of traffic-related emissions.
Conclusion
This study examined how proximity to high-traffic roads relates to cytokine expression and quality-of-life outcomes in patients with CRS. While some associations were observed, particularly in psychological symptom scores and select cytokines, most findings—especially for CRSwNP—were not statistically significant. These results suggest that traffic-related exposures may play a limited role in PM2.5-driven inflammation in CRS, though further research with more precise exposure measures is needed. The observed racial disparities in roadway proximity highlight the importance of continued efforts to address environmental inequities.
Footnotes
Author Note
This article was accepted as a poster at the 71st Annual Meeting of the American Rhinologic Society, October 10-11, 2025.
Ethical Considerations
This study received approval from the Institutional Review Board of Vanderbilt University Medical Center, IRB #130114
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.