
Abstract
Purpose:
This study aimed to explore survival outcomes of and prognostic factors in nasopharyngeal mucoepidermoid carcinoma (NPMEC).
Patients and Methods:
We reviewed a total of 57 patients diagnosed with NPMEC, including 19 patients in our center and 38 patients with detailed individual survival data in the literature. The Kaplan-Meier method and the log-rank test were used to assess overall survival (OS) and progression-free survival (PFS). Furthermore, the multivariate survival analysis was evaluated using the Cox regression model.
Results:
The average age of the patients was 45.8 years (range 13-71 years), with a male-to-female ratio of 0.84. During the mean follow-up time of 49 months (range, 3-149 months), the OS rates at 1, 3 and 5 years were 96.1%, 78.7%, and 62.8%, respectively, and the PFS rates at 1, 3 and 5 years were 91.4%, 71.6%, and 51.3%, respectively. The log-rank test showed that lymphatic metastasis affected OS and PFS, while stage T affected PFS. Multivariate regression analysis showed that lymphatic metastasis was associated with worse OS and PFS, that stage T was associated with unfavorable PFS, and that combined therapy improved PFS independently.
Conclusions:
Patients with NPMEC have favorable 5 year OS and PFS. Lymphatic metastasis was the independent factor for OS, while lymphatic metastasis, stage T, and treatment modality were the independent factors for PFS.
Introduction
Nasopharyngeal adenocarcinoma was first classified into 2 pathological types by Zong et al 1 salivary gland type (adenoid cystic carcinoma [ACC] and mucoepidermoid carcinoma [MEC]) and general type (papillary adenocarcinoma and acinic cell adenocarcinoma). In 2017, the WHO classified nasopharyngeal malignant tumors into nasopharyngeal carcinoma, nasopharyngeal papillary adenocarcinoma and salivary gland-type carcinomas. 2 It is worth noting that cancers of minor salivary glands in the nasopharynx are extremely rare, accounting for <2% of all nasopharyngeal cancers. 3 Specifically, nasopharyngeal mucoepidermoid carcinomas (NPMEC) comprise <15% of all nasopharyngeal salivary gland malignancies.4,5
Considering its rarity, only a few NPMEC studies have been published, of which most have been single case reports or small series studies. 3 Furthermore, NPMEC has been commonly reported with other nasopharyngeal adenocarcinoma or other head and neck MECs. However, the clinical behaviors between NPMEC and other nasopharyngeal adenocarcinomas are not similar. For example, NPMEC has a lower invasion of the cranial nerve and a greater disease-specific survival than ACC in the nasopharynx.6,7 The distant metastases rate for ACC and MEC is ~25.0%, 8 while the lymphatic and distant metastases for low-grade nasopharyngeal papillary adenocarcinoma are scarce and the prognosis is excellent, and most patients remain free of recurrent or metastatic tumors.7,9 Therefore, this calls for studies to explore the clinical features, survival, and prognosis of NPMEC. In this study, we explore the survival outcome of and prognostic factors for NPMEC by summarizing the experience in treating NPMEC at our center combined with that of the published literature.
Patients and Methods
We retrospectively reviewed medical records for all patients diagnosed with mucoepidermoid carcinoma that occurred in the nasopharynx between 2014 and 2020 at the Department of Otorhinolaryngology, Eye & ENT Hospital, Fudan University, China. Clinicopathological characteristics were recorded, including demographic data, clinical symptoms, imaging findings, treatment procedure, postoperative pathological diagnosis and stage (AJCC, eighth edition), follow-up and outcomes. All patients underwent endoscopic surgeries. Radiotherapy, chemotherapy, or chemoradiotherapy were performed preoperatively or postoperatively. Follow-up was performed every 3 months in the first year after surgery, every 6 months from the second to fifth year after surgery and once every year after 5 years. Enhanced magnetic resonance imaging (MRI) or computed tomography (CT) was performed at each follow-up. Signed informed consent forms were obtained from all patients.
A comprehensive literature search was also performed on the PubMed database for all NPMEC cases in articles in English. A total of 14 articles were identified, of which 9 studies with individual patient data of 38 patients were selected for a review of the literature. The other 5 articles were excluded because they lacked detailed patient data. Then, age, gender, T stage, node involvement, distant metastasis, treatment procedures and survival data were screened.
All cases were subjected to an overall survival (OS) analysis, and cases with a detailed stage of TNM and time of progression-free survival (PFS) were selected for prognostic factor analyses. OS was defined as the time to death or the last follow-up, whereas PFS was defined as the time to disease progression, including death, relapse, lymphatic metastasis, distant metastases or disease progression. The Kaplan-Meier method was used to assess OS and PFS according to different prognostic factors, while the log-rank test was used to evaluate the difference in OS and PFS according to sex, age, stage T, lymphatic involvement, and treatment modality. The Cox regression model was used for the univariate and multivariate survival analyses. In particular, the multivariate regression analysis included factors that showed statistical significance in the log-rank test, and factors that may influence patients’ OS and PFS according to clinical experience. The follow-up period was from the date of surgery to the date of death or the last follow-up. All statistical analyses were performed with the SPSS software, version 19.0 (IBM Corp, Armonk, NY, USA), and a 2-tailed P < .05 was considered statistically significant.
Results
A total of 57 patients were involved in this study, including 19 patients identified from our center and 38 patients from the relevant literature. Twenty-six patients were men (45.6%) and 31 were women (54.4%), with a mean ± standard deviation age of 45.8 ± 12.9 years (range, 13-71 years). The mean follow-up time was 49 months (range, 3-149 months). The results showed that the overall 1, 3 and 5 year survival rates were 96.1%, 78.7%, and 62.8%, respectively (Figure 1a), while the 1, 3, and 5 year PFS rates were 91.4%, 71.6%, and 51.3%, respectively (Figure 1b).
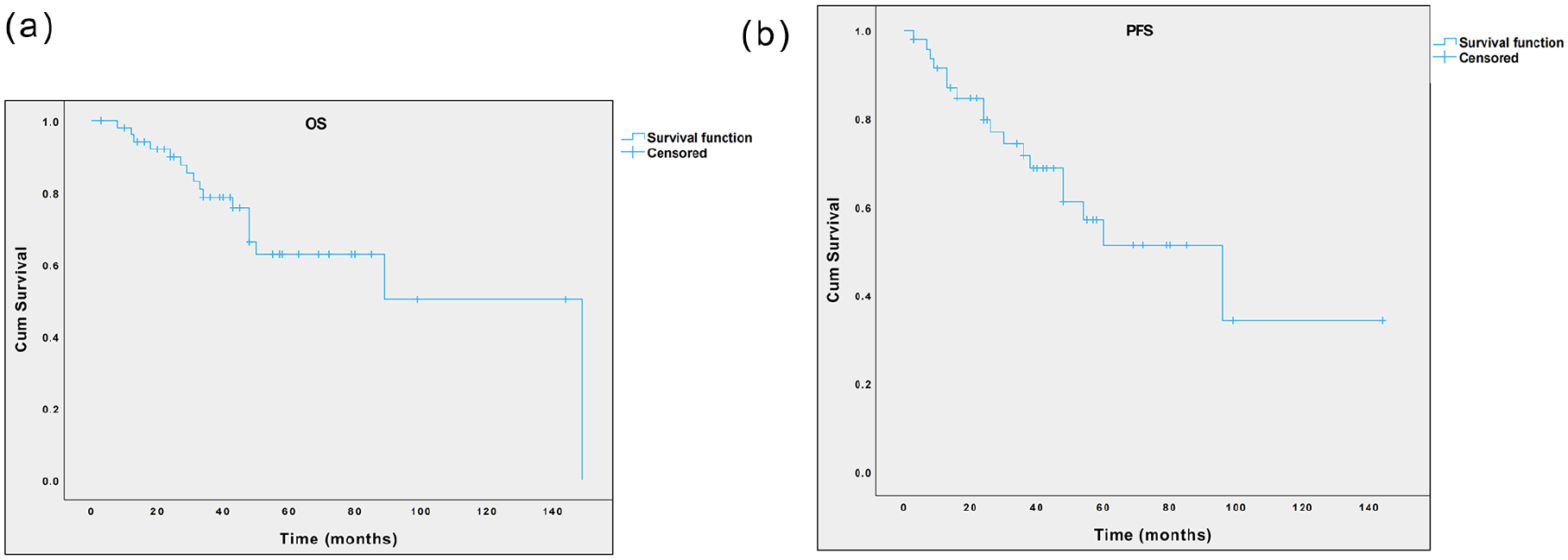
Kaplan-Meier curve of the overall survival probability (a) and the progression-free survival probability (b) of patients with NPMEC. NPMEC, nasopharyngeal mucoepidermoid carcinoma.
Table 1 shows a summary of the patients in our center. The most common presenting symptoms were nasal obstruction (8/19), bleeding (4/19), aural fullness (4/19), and tinnitus (2/19). None had symptoms or signs of cranial nerve paralysis at presentation, and only 1 patient had palpable neck masses. The average time of clinical symptoms was 8.6 months (range, 0.6-24 months). The majority of NPMEC cases were limited in the nasopharyngeal space (N = 9, 47.4%). Other invasion sites were the parapharyngeal space (N = 6, 31.6%), the oropharyngeal space (N = 4, 21.1%), the petrous process (N = 3, 10.5%), the base of the sphenoid bone (N = 3, 10.5%), and the oval foramen (N = 1, 5.3%). Three patients (15.8%) had lymphatic metastases, 3 patients had retropharyngeal lymphatic metastases, and 1 patient had unilateral lymphatic metastasis of the neck. According to the AJCC eighth edition staging system, 10 patients (52.6%) were diagnosed with stage I disease, 7 patients (36.8%) with stage II disease, 1 patient (5.3%) with stage III disease, and 1 patient (5.3%) with stage IVa disease. Two patients had undergone chemoradiotherapy 10 years ago (Table 1, case 11) and 3 years ago (Table 1, case 19), respectively, in other hospitals to treat NPMEC and only visited our hospital after recurrence occurred. Endoscopic surgery alone was performed in 8 patients, whereas endoscopic surgery combined with adjuvant therapies was performed in 11 patients. One patient had radical neck dissection. The internal carotid artery (ICA) was ligated in 2 patients after the balloon occlusion test (BOT), in which 1 patient had the tumor encasing the ICA at the nasopharyngeal level and the other patient had the tumor closely adjacent to the ICA. The pedicled nasoseptal flap was harvested to cover the skull base defect in 3 patients. Two of the 3 patients with neoadjuvant radiotherapy or chemoradiotherapy prior to surgery had significant tumor remission. One patient received neoadjuvant chemotherapy before surgery. Seven patients underwent postoperative radiotherapy or chemoradiotherapy. The nodes in 3 patients with retropharyngeal lymphatic metastasis remained stable after radiotherapy. Six patients experienced relapse, and 4 patients had postoperative lymphatic metastases. It should be noted that 3 patients succumbed to relapse and lymphatic metastases.
Features of 19 Cases With Nasopharygeal Mucoepidermoid Carcinoma in Our Department.
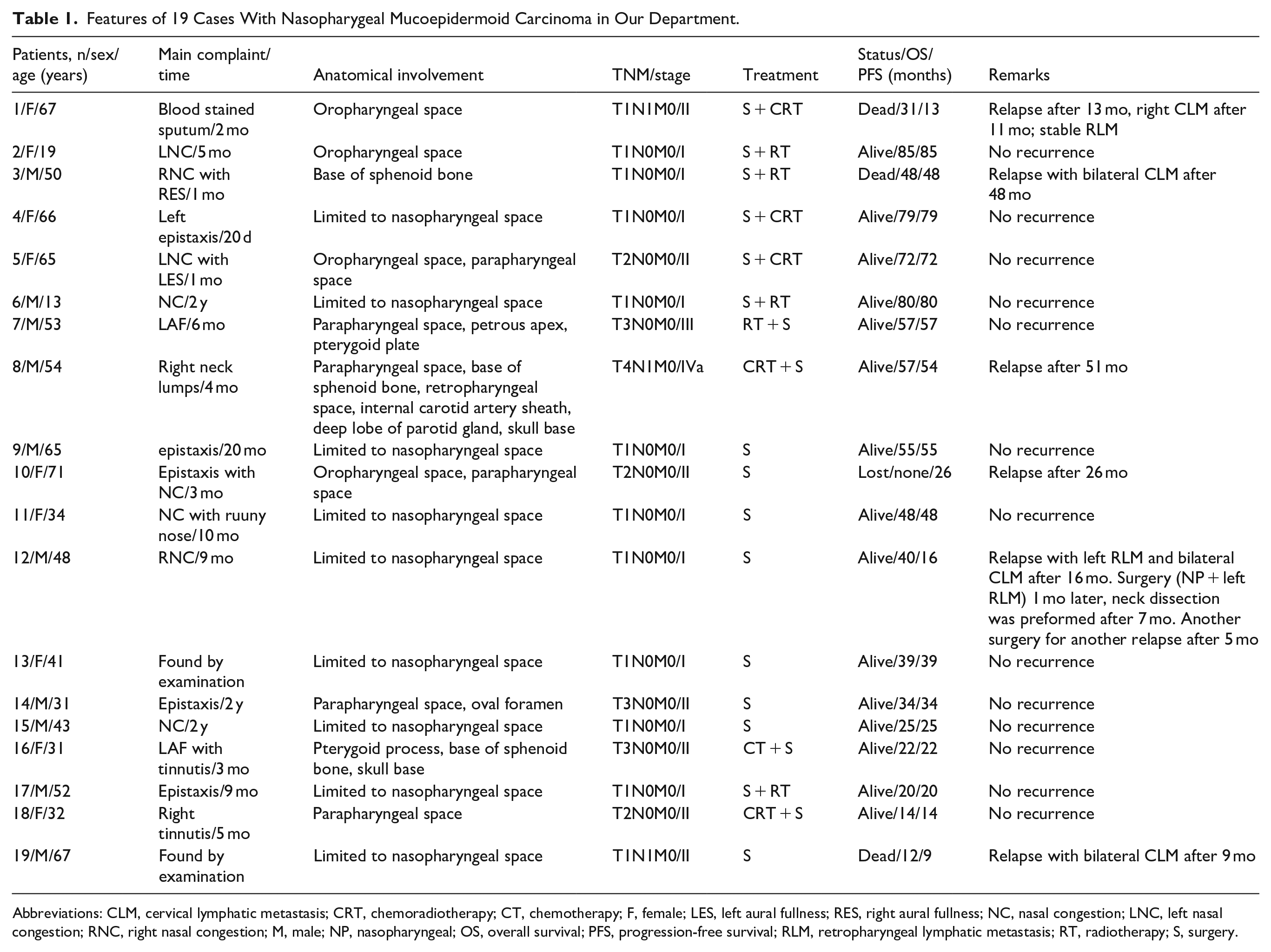
Abbreviations: CLM, cervical lymphatic metastasis; CRT, chemoradiotherapy; CT, chemotherapy; F, female; LES, left aural fullness; RES, right aural fullness; NC, nasal congestion; LNC, left nasal congestion; RNC, right nasal congestion; M, male; NP, nasopharyngeal; OS, overall survival; PFS, progression-free survival; RLM, retropharyngeal lymphatic metastasis; RT, radiotherapy; S, surgery.
Table 2 shows a summary of the patients identified in the literature. After conducting a literature review, a total of 38 patients were included, of which 2 had no T and N classification information. The remaining 36 patients were classified as follows: 6 patients in T1, 15 patients in T2, 7 patients in T3 and 8 patients in T4; and 28 patients in N0, 3 patients in N1, 2 patients in N2, and 3 patients in N3. Three patients underwent surgery alone, 24 patients underwent surgery combined with other therapies and 11 patients underwent radiotherapy or chemoradiotherapy. According to the last follow-up, 16 patients had succumbed, 22 patients were alive, and 4 patients were lost. After first treatments, 17 patients had progression of the disease, 9 patients experienced relapse, 2 patients had lymphatic metastases, 9 patients had distant metastases and 1 patient had uncontrolled tumor. The lung was the most common site of distant metastasis (n = 7), and the other sites included the liver (n = 1) and unknown site (n = 1).
Summary of the Patients Identified in the Literature.
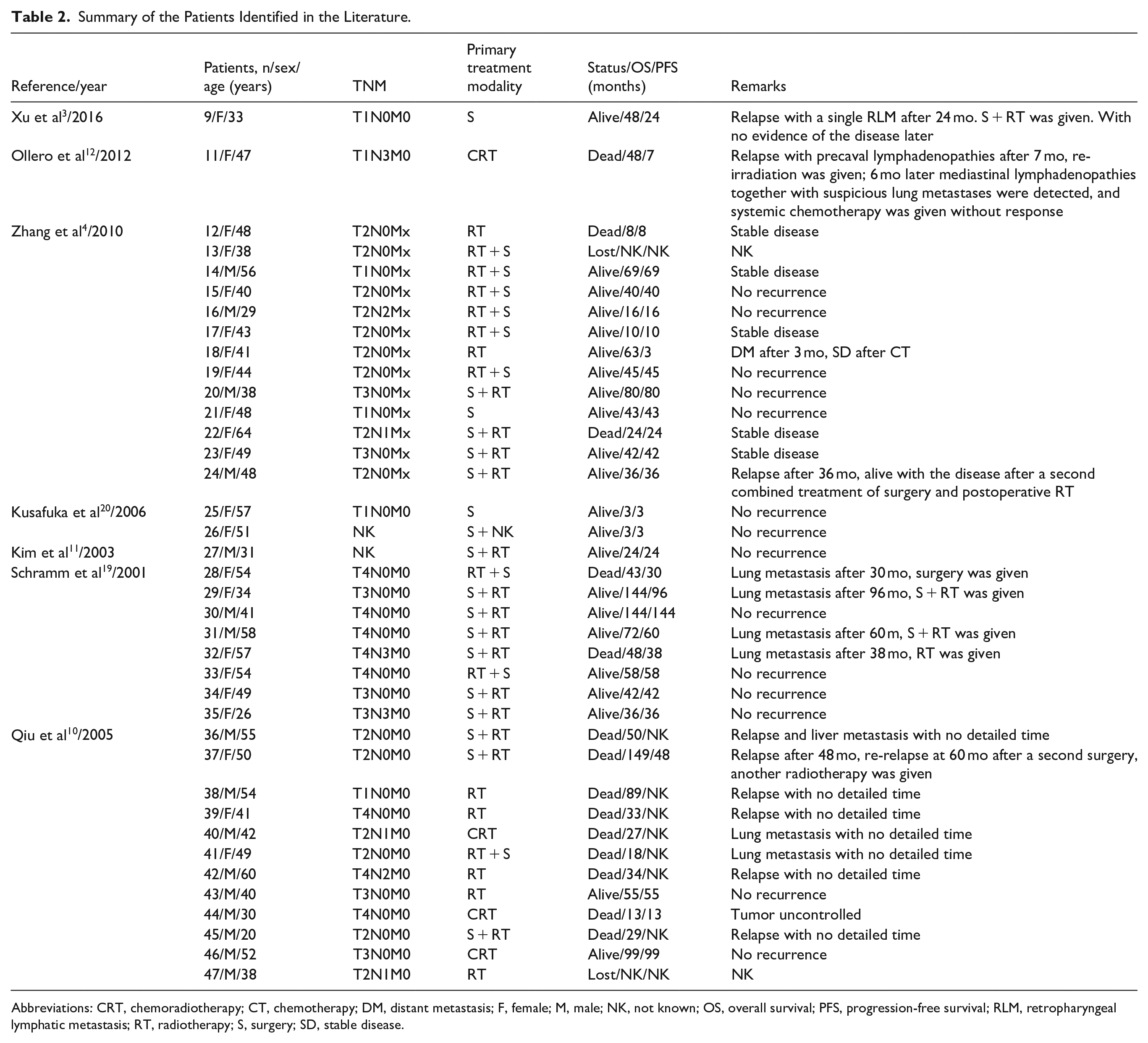
Abbreviations: CRT, chemoradiotherapy; CT, chemotherapy; DM, distant metastasis; F, female; M, male; NK, not known; OS, overall survival; PFS, progression-free survival; RLM, retropharyngeal lymphatic metastasis; RT, radiotherapy; S, surgery; SD, stable disease.
Table 3 shows the prognostic factors for the OS of NPMEC. Lymphatic metastasis adversely affected OS, with patients having a 3 year survival rate of 45%. On the contrary, the 3 year survival rate for patients without lymphatic metastasis was 74.9% (P = .001; Figure 2c). The results indicated that the T stage influenced survival, with 5 year survival rates of T1, T2, T3, and T4 being 69.9%, 44.5%, 100%, and 37.5%, respectively (P = .041; Figure 2d). Although the 5 year survival rate of patients with age ≤45 years (78.6%) was higher than that of patients with age >45 years (53.9%), age did not influence OS (P = .199; Figure 2a). The 5 year survival rate of the female patients (60.6%) and the male patients (65.3%) was comparable (P = .985; Figure 2b). The 5 year survival rate of combined treatment (65.5%) was higher than that of single treatment (58.9%), but there was no significant difference between the 2 groups (P = .218; Figure 2e). Moreover, the results of multivariate regression analysis showed that lymphatic metastasis was the independent prognostic factor for OS (P = .018; Table 4).
Log-Rank Test of Prognostic Factors for OS and PFS of Nasopharyngeal Mucoepidermoid Carcinoma.
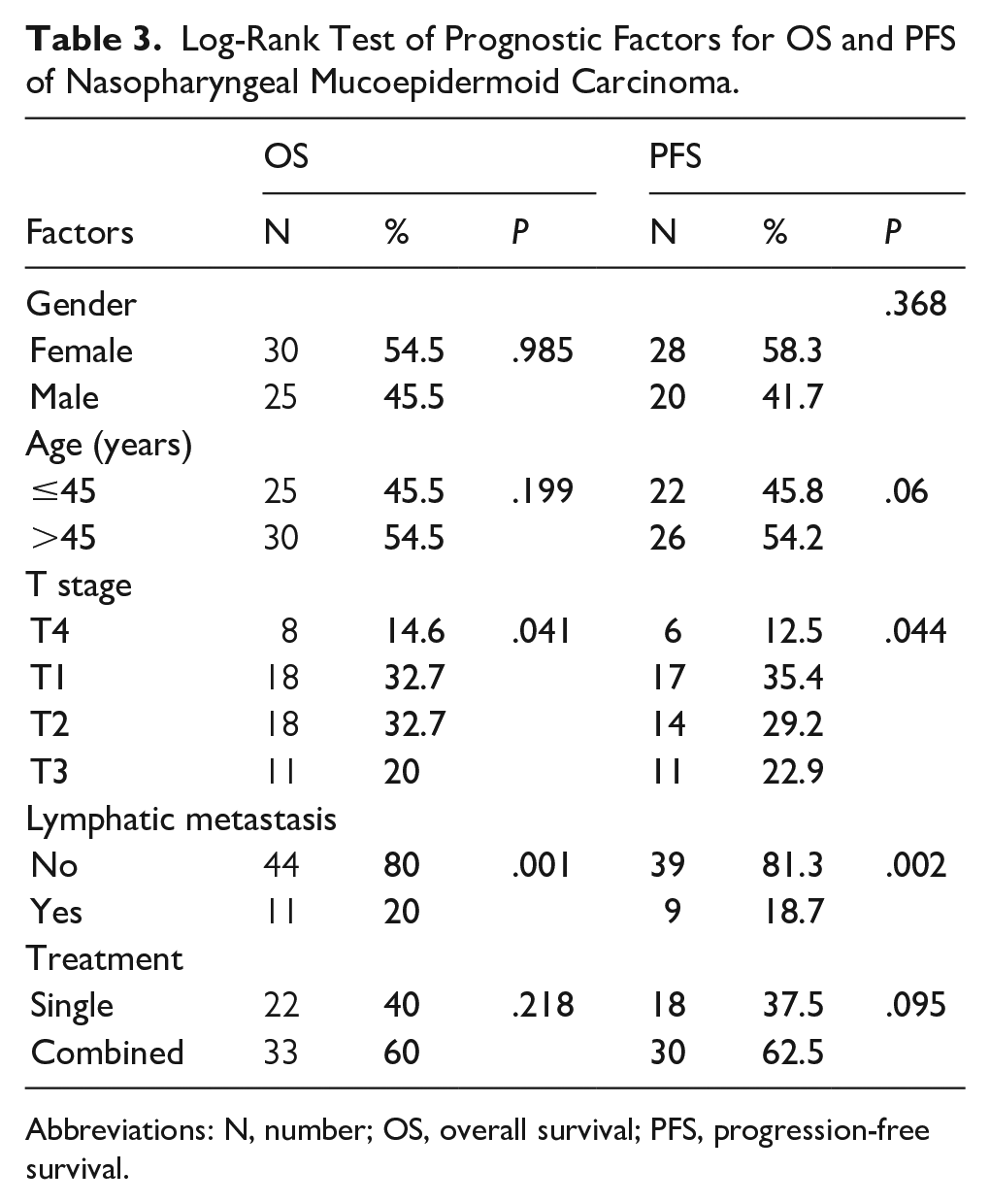
Abbreviations: N, number; OS, overall survival; PFS, progression-free survival.
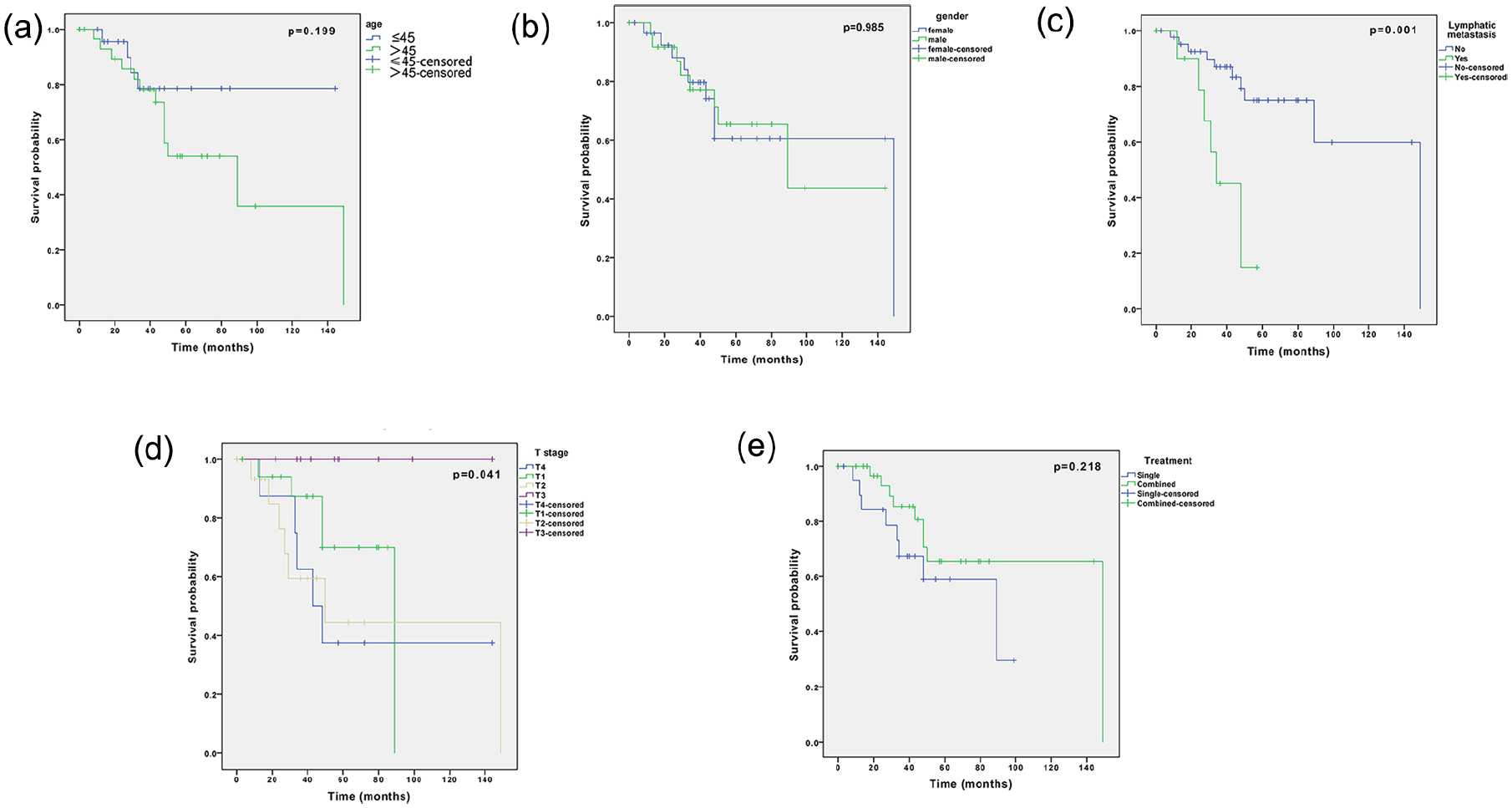
Kaplan-Meier curves for the overall survival probability of patients age >45 or age ≤45 (a), female and male (b), with or without lymphatic metastases (c), difference T stage (d), single or combined treatment (e).
Univariate and Multivariate Cox Regression Analyses of Prognostic Factors Associated With OS in Patients With Nasopharyngeal Mucoepidermoid Carcinoma.
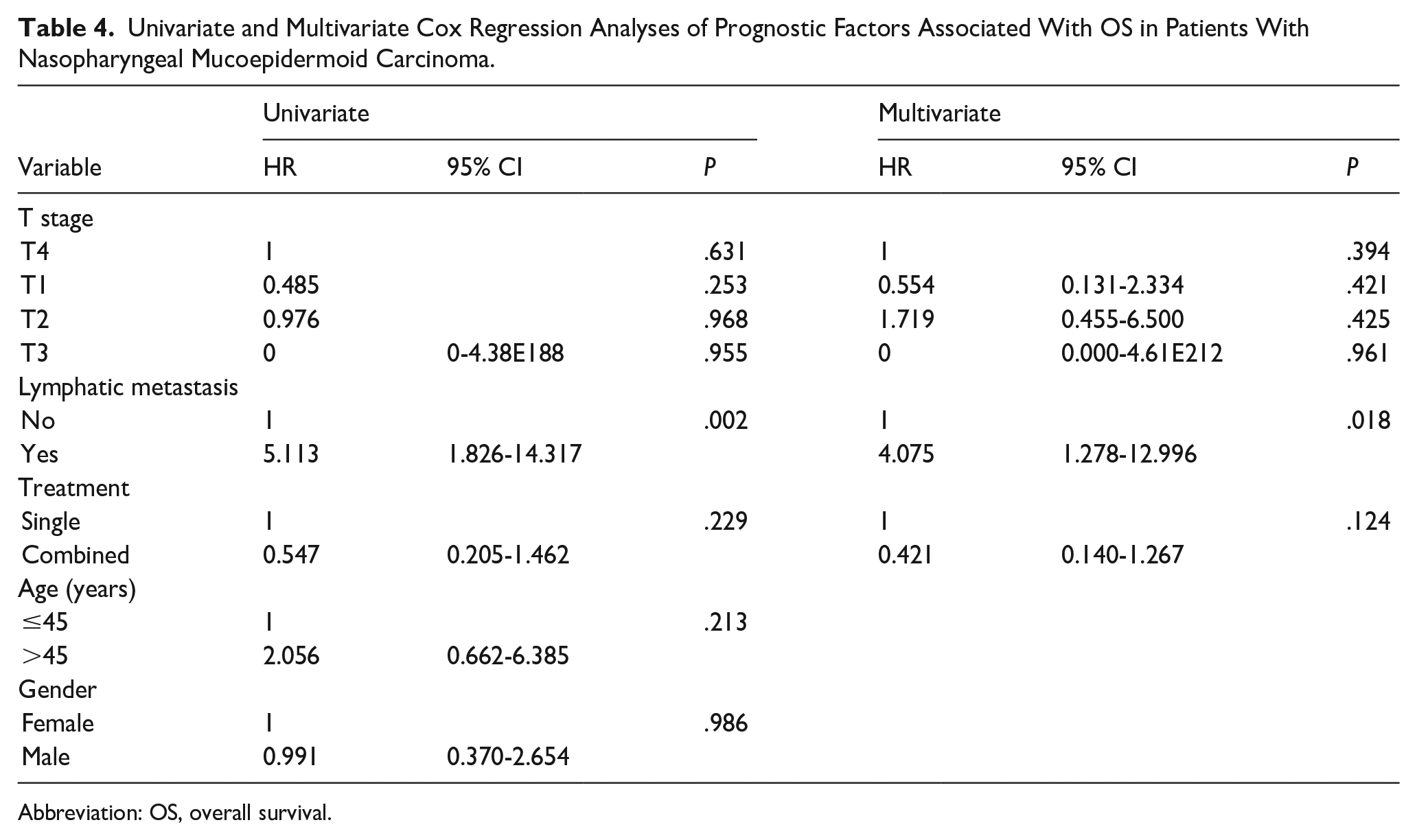
Abbreviation: OS, overall survival.
Table 3 also shows the prognostic factors for the PFS of NPMEC. The 3 year PFS rate of patients with lymphatic metastasis was significantly lower than for patients without lymphatic metastasis (46.9% vs 76.3%; P = .002; Figure 3c). The 5 year PFS rates of T1, T2, T3, and T4 were 58.4%, 23.8%, 100%, and 16.7%, respectively (P = .044; Figure 3d), indicating that stage T affected the PFS. The 5 year PFS rate of patients with age ≤45 years was higher than that of patients with age >45 years (83.3% vs 34.3%), but no significant difference was found between the groups (P = .060; Figure 3a). In addition, gender did not have an effect on the PFS rate (female to male: 53.1% vs 52.6%; P = .368; Figure 3b). The combined treatment group had a slightly higher 5 year PFS rate (55.5%) than that of single treatment group (49.4%), but there was no significant difference between the 2 groups (P = .095; Figure 3e). Importantly, the results of multivariate regression analysis showed that stage T (P = .040), lymphatic metastasis (P = .008), and treatment modality (P = .003) were independent prognostic factors for PFS (Table 5).
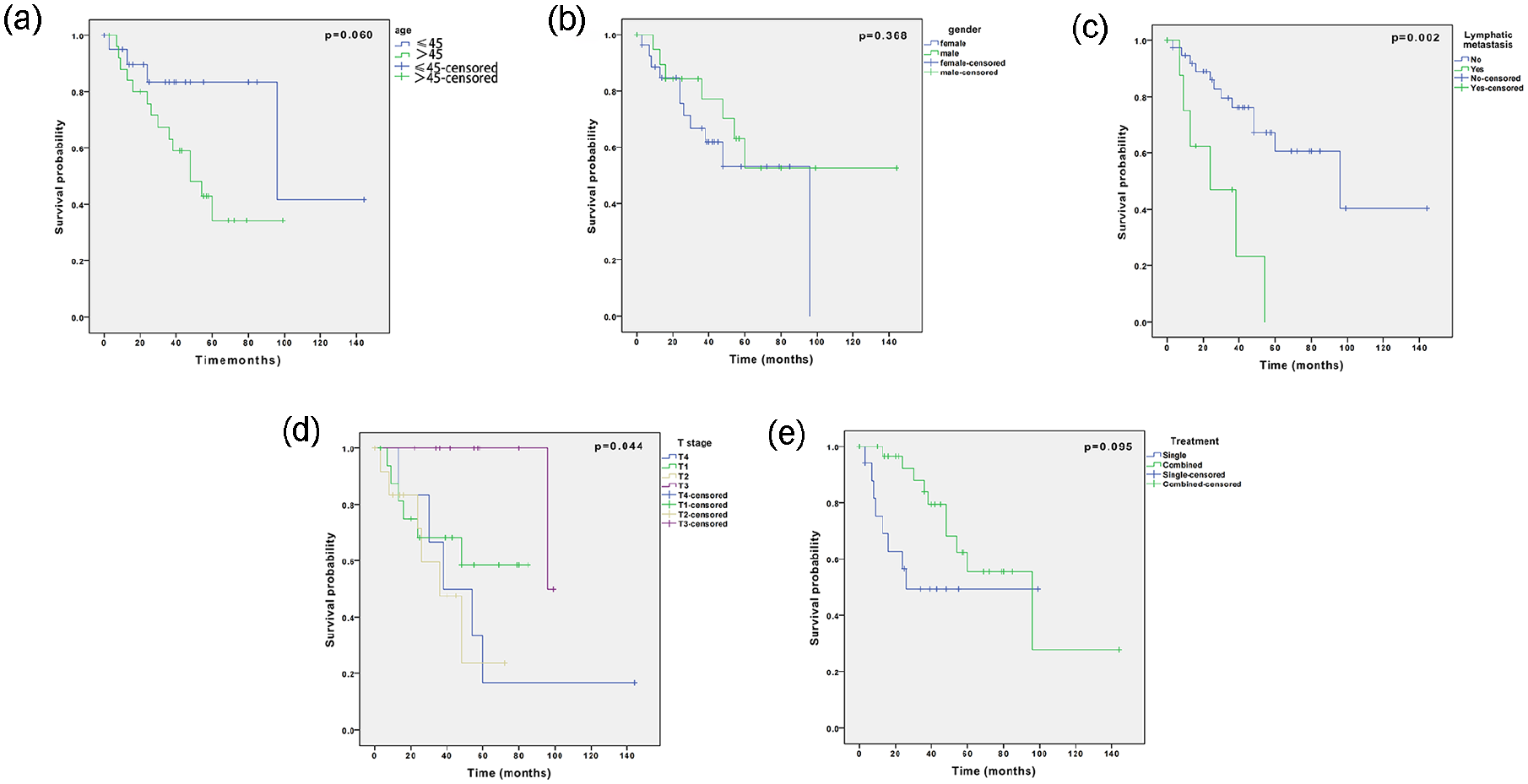
Kaplan-Meier curves for the progression-free survival probability of patients age >45 or age ≤45 (a), female and male (b), with or without lymphatic metastases (c), difference T stage (d), and single or combined treatment (e).
Univariate and Multivariate Cox Regression Analyses of Prognostic Factors Associated With PFS in Patients With Nasopharyngeal Mucoepidermoid Carcinoma.
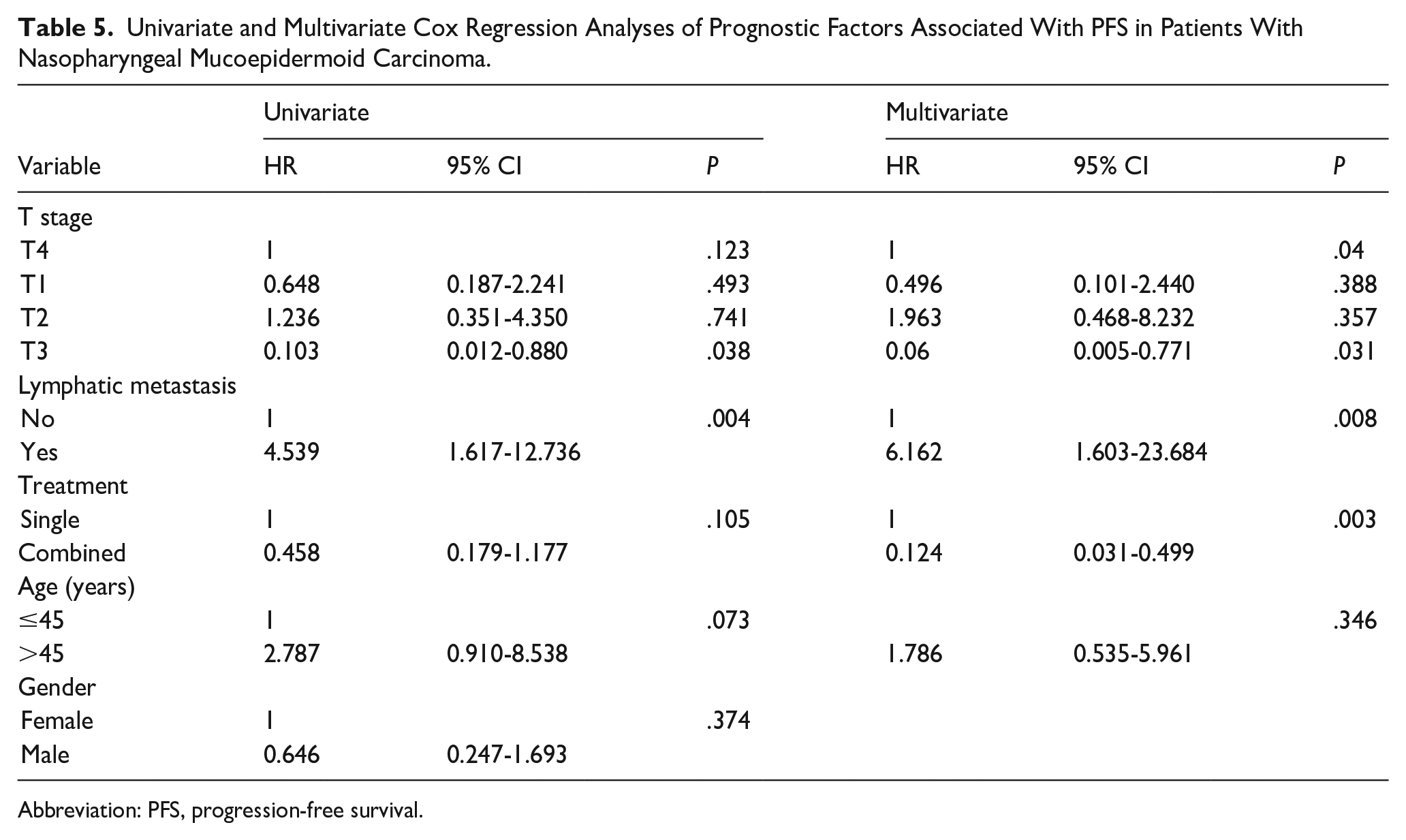
Abbreviation: PFS, progression-free survival.
Discussion
NPMEC accounts for a very small proportion of primary nasopharyngeal malignancies. Given its rarity and lack of research, there is no consensus on the management and prognosis of NPMEC, and the survival rate data are limited. To our knowledge, this study is the largest study of NPMEC (involving 57 patients, including 19 from our center). The results showed that the overall 1, 3, and 5 year survival rates were 96.1%, 78.7%, and 62.8%, respectively, and the 1, 3, and 5 year PFS rates were 91.4%, 71.6%, and 51.3%, respectively. Lymphatic metastasis was found to be the independent prognostic factor for both OS and PFS, and stage T and treatment modality were also independent prognostic factors for PFS. The patients were 31 women and 26 men, with a male-to-female ratio of 0.84 and an average age of 45.8 years (range, 13-71 years). Data obtained from our center indicated that nasal obstruction, bleeding, and aural fullness were the most common presentations, and the incidence of lymphatic metastasis for NPMEC was low (15.8%), which is consistent with the findings of a previous study. 4
Furthermore, we conducted a comprehensive literature search for data on OS of NPMEC. Zhang et al 4 reported an overall median survival of 43 months in a case series involving 13 patients. Liu et al 8 reported an overall 5 year survival rate of 56.3% in a series involving 8 patients. In this study, the overall 5 year survival rate was 62.8%, with an overall median survival of 149 months, which was better than in the previous 2 studies.4,8 This may be attributed to improved operative skills and equipment over the past decades. Another reason could be that there was no delay in the diagnosis of NPMEC as a result of better health awareness, with an average clinical presentation time of 8.6 months, and thus, the tumors could be resected at an early stage.
Studies have recommended primary surgery as the standard treatment for NPMEC, and postoperative radiotherapy is administered when there are unfavorable conditions such as positive surgical margin, high-grade carcinomas, and macroscopic residual tumors.4,10,11 Radiotherapy or chemotherapy could also be given as a single treatment when the tumor is unresectable, with or without lymphatic or distant metastases. 12 Herein, multivariate Cox regression analyses of prognostic factors revealed that combined treatment was associated with better PFS than single treatment, although it did not influence patient’s OS, indicating that combined treatment was the optimal choice for NPMEC. This is consistent with the findings of Liu et al 13 who proposed combined surgical treatment and radiotherapy as the main treatment for primary salivary gland-type nasopharyngeal carcinomas.
In the past, various open approaches have been used to adequately expose and completely resect nasopharyngeal lesions, including lateral rhinotomy, transmaxillary swing, transoral-palatal, lateral infratemporal fossa, and subfrontal routes. 3 However, open surgery may cause severe cosmetic and functional damage in such an anatomically challenging region, which makes it not widely accepted as a practice of primary surgery. 4 Given the development of endoscopic equipment and skills, endoscopic surgery has been proposed as an alternative treatment because it provides a close-up visualization of the tumor and allows for more precise resection round it. In particular, all patients in our department underwent endoscopic surgeries without severe morbidity or complications.
One of the challenges of the nasopharyngeal endoscopic procedure is parapharyngeal ICA injury, which is a fatal complication with a rate of incidence between 0.4% and 3.8%. 14 The first step in avoiding intraoperative damage to the ICA is to know the relationship between the ICA and tumors. Based on the range of tumor surrounding the ICA, the tumor site, the ICA segment, the tumor blood supply, and the extent of tumor resection, our team recommended an ICA treatment strategy according to the score on the 5S ICA grading scale. 15 Preoperative ICA testing using BOT was recommended to accurately predict individual tolerance to the loss of the carotid artery in cases where it was impossible to separate tumors from the ICA. Thus, ICA could be sacrificed during surgery after ICA embolism was performed. In this study, to avoid intraoperative injury and significant hemorrhage, angioembolization was performed and the ICA was ligated during endoscopic procedures in 2 cases where the lesions were closely adjacent to or encasing the ICA.
It is not yet clear whether NPMEC is radioresistant. Zhang et al 4 suggested that NPMEC was radioresistant for tumors (8/12) receiving primary radiotherapy because they remained stable after irradiation except for 1 complete remission. However, the residual tumors (4/12) did not shrink at all after postoperative irradiation. Ollero et al 12 found that the tumor of the nasopharynx and lymphatic cervical levels could achieve complete remission after receiving primary chemoradiotherapy. In this study, 2 of the 3 patients with neoadjuvant irradiation presented significant nasopharyngeal tumor remissions. However, no conclusion could be made due to the small number of patients, and thus, further studies should be conducted to validate this finding.
Previous studies have reported that the incidence of lymphatic metastasis for NPMEC ranges between 11.9% and 25%.3,4,7,10 In our center, only 3 patients (15.8%) had lymph node involvement. Additionally, multivariate Cox regression analyses revealed that lymphatic metastasis was an independent prognostic factor for OS and PFS, which is consistent with a previous study. 16 This indicated that active measurements should be taken to address the lymph nodes involved. Retropharyngeal and cervical lymphatic metastases are commonly observed in head and neck malignancies. Studies have reported that the presence of retropharyngeal lymphatic metastases was associated with worse survival rates for sinonasal and nasopharyngeal squamous cell carcinoma, and the retropharyngeal lymphatic nodes were routinely covered during the radiotherapy procedure.17,18 In the cases from our center, the patient with bilateral retropharyngeal and unilateral cervical node involvement received neoadjuvant chemoradiotherapy that resulted in complete remission. Stable unilateral retropharyngeal lymph node involvement was detected in 1 patient after postoperative chemoradiotherapy. A patient received chemoradiotherapy for the retropharyngeal lymph node, which remained stable during follow-up. However, bilateral cervical node involvement was detected 9 months after endoscopic resection for NPMEC.
Although this study involved the largest cases of NPMEC, there were some limitations. First, survival and prognosis were analyzed based on the cases in our center combined with the cases in the previous literature; thus, the heterogeneity resulting from different clinical centers may lead to biased results. Second, the surgical modality during the different periods when the studies were performed could have affected the results. For example, open surgeries have been performed in the past 19 and endoscopic surgeries have tended to be performed in recent years. Third, although the histological grade of NPMEC has previously been reported to affect prognosis,20,21 we were unable to assess its influence on prognosis due to the lack of information on the grade of NPMEC in our center. Therefore, future prospective controlled multicenter studies should be conducted to elaborate the features and prognoses of NPMEC.
Conclusions
Patients with NPMEC have good 1, 3, and 5 year OS and PFS. Lymphatic metastasis is the independent prognostic factor for OS, while stage T, lymphatic metastasis, and treatment modality are the independent prognostic factors for PFS. It was evident that the management of NPMEC requires a combined therapy.
Footnotes
Ethical Considerations
The work is compliant with ethical standards and has been ethics- approved by the commission of Eye & ENT Hospital (EENTH) of Fudan University, China.
Author contributions
Yuting Lai was responsible for collecting data and conducted experiments and writing. Xiaole Song conducted the actual data analysis and reviewed the manuscript for scientific accuracy. Huankang Zhang collected data and created figures and tables. Wanpeng Li and Jingyi Yang helped collect data and conducted experiments. Xicai Sun participated in operating surgeries. Quan Liu participated in operating surgeries and supervised the research project. Dehui Wang participated in operating surgeries and provided guidance to the team. Hongmeng Yu identified the research problem, formulated the hypothesis, and designed the overall study framework.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the China National Natural Science Foundation (No. 82301278) and the New Technologies of Endoscopic Surgery in Skull Base Tumor: CAMS Innovation Fund for Medical Sciences (CIFMS; 2019-I2M-5-003).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article.